Download as doc, pdf, or txt
You might also like
- Head Neck Assesment and Technique of Physical AssesmentDocument4 pagesHead Neck Assesment and Technique of Physical AssesmentFitriani PratiwiNo ratings yet
- Checklist 17: Head-to-Toe Assessment Disclaimer: Always Review and Follow Your Hospital Policy Regarding This Specific Skill. Safety ConsiderationsDocument3 pagesChecklist 17: Head-to-Toe Assessment Disclaimer: Always Review and Follow Your Hospital Policy Regarding This Specific Skill. Safety ConsiderationsKimberly Joy GregorioNo ratings yet
- Complete Physical Examination Eyes, Ears, Nose, ThroatDocument103 pagesComplete Physical Examination Eyes, Ears, Nose, Throatjennylyn guadalupe100% (3)
- General Principles of Physical ExaminationDocument35 pagesGeneral Principles of Physical Examinationjaish8904100% (4)
- Head To Toe Assessment in 5 MinutesDocument30 pagesHead To Toe Assessment in 5 Minutesdabyers8150No ratings yet
- Vawc Case StudiesDocument106 pagesVawc Case Studieskylexian1100% (4)
- Steel-Ply Concrete Forming SystemDocument72 pagesSteel-Ply Concrete Forming SystembetopagoadaNo ratings yet
- UntitledDocument11 pagesUntitledLile RajabaNo ratings yet
- Hysical Assessment/ Examination Head To ToeDocument14 pagesHysical Assessment/ Examination Head To ToeGio LlanosNo ratings yet
- Retdem Physical AssessmentDocument6 pagesRetdem Physical AssessmentTrishia May DanaoNo ratings yet
- Assessment - of - SKIN HAIR AND NAILS CHECKLISTDocument8 pagesAssessment - of - SKIN HAIR AND NAILS CHECKLISTJonah R. MeranoNo ratings yet
- Guidelines in RLE 1F Video AssignmentDocument5 pagesGuidelines in RLE 1F Video Assignment2D - Con-ui, Sofia ChantelleNo ratings yet
- Physical AsessmentDocument15 pagesPhysical AsessmentnonelNo ratings yet
- Physical Assessment/ Examination Head To Toe: Prepared by T: Sanaa Abdel HamedDocument33 pagesPhysical Assessment/ Examination Head To Toe: Prepared by T: Sanaa Abdel HamedAjdin RovcaninNo ratings yet
- Head To Toe AssessementDocument97 pagesHead To Toe AssessementHenry CalisuraNo ratings yet
- Nursing ProcessDocument5 pagesNursing ProcessWilton Norman JvmantocNo ratings yet
- Physical Assessment Script FinalDocument9 pagesPhysical Assessment Script FinalArabiah AbdullahNo ratings yet
- Buclb9nf9 - 3. SKL Checklist Assessment of HEENT With RationaleDocument8 pagesBuclb9nf9 - 3. SKL Checklist Assessment of HEENT With RationaleHecy CristoNo ratings yet
- PE GuidelinesDocument56 pagesPE GuidelinesGene LynNo ratings yet
- 6 Head To Toe Physical Assessment 2Document12 pages6 Head To Toe Physical Assessment 2rumasadraunaNo ratings yet
- Review of Systems For Current Health Problems (Health Assessment)Document5 pagesReview of Systems For Current Health Problems (Health Assessment)younggirldavid100% (1)
- Physical Examination: Presented To Mrs. Nisha Mane Assistant Professor D.Y.P.S.O.NDocument41 pagesPhysical Examination: Presented To Mrs. Nisha Mane Assistant Professor D.Y.P.S.O.NNilakshi Barik MandalNo ratings yet
- Physical AssessmentDocument6 pagesPhysical AssessmentDonna Flor NabuaNo ratings yet
- FINAL Genral Ward ADULT PHYSICAL ASSESSMENT CompressedDocument59 pagesFINAL Genral Ward ADULT PHYSICAL ASSESSMENT CompressedDustin AgsaludNo ratings yet
- Activity 6 Care of Older Person Roxane SDocument2 pagesActivity 6 Care of Older Person Roxane SRoxane AquillanNo ratings yet
- History Pe EntDocument44 pagesHistory Pe EntFalling HateNo ratings yet
- Head To Toe AssessementDocument97 pagesHead To Toe Assessementrootie100% (3)
- 'Span BibleDocument96 pages'Span BiblePatrice BlakeNo ratings yet
- Hair, Face, Nose, Neck, Skin, and NailsDocument4 pagesHair, Face, Nose, Neck, Skin, and NailsZJ GarcianoNo ratings yet
- MidtermsDocument41 pagesMidtermsgus peepNo ratings yet
- Physical AssessmentDocument5 pagesPhysical AssessmentIsabel DizonNo ratings yet
- Assessment Head To ToeDocument28 pagesAssessment Head To ToeDechy Lyn PalmaNo ratings yet
- Basic Nursing Fon I Lecture Notes Unit ViiDocument22 pagesBasic Nursing Fon I Lecture Notes Unit Viichisomokonkwo619No ratings yet
- Health Assessment ReviewerDocument8 pagesHealth Assessment ReviewerJane Heart AguilonNo ratings yet
- Physical Examination: Binal Joshi Assistant Professor Child Health Nursing Manikaka Topawala Institute of NursingDocument101 pagesPhysical Examination: Binal Joshi Assistant Professor Child Health Nursing Manikaka Topawala Institute of NursingBinal JoshiNo ratings yet
- Lesson (1) Pediatric History Taking and Physical ExaminationDocument27 pagesLesson (1) Pediatric History Taking and Physical ExaminationDrmirfat AlkashifNo ratings yet
- BCS General Principles of Physical ExaminationDocument43 pagesBCS General Principles of Physical ExaminationPande Indra PremanaNo ratings yet
- Pocket Card HEENT Assessment January2024Document3 pagesPocket Card HEENT Assessment January2024adnan MukhtarNo ratings yet
- HAinteg Mouth NoseDocument49 pagesHAinteg Mouth NoseInigo NaciancenoNo ratings yet
- Pocket Card - Head To Toe Assessment - August 2022Document3 pagesPocket Card - Head To Toe Assessment - August 2022Amram LanzaderasNo ratings yet
- Head and Face AssessmentDocument4 pagesHead and Face AssessmentDexter WongNo ratings yet
- IM Written Report August 2019Document3 pagesIM Written Report August 2019Fu Xiao ShanNo ratings yet
- GROUP 1 - Inspection, Palpation, Simple Sentences.Document22 pagesGROUP 1 - Inspection, Palpation, Simple Sentences.Andrea Estefania Apolo LomasNo ratings yet
- Health Assessment Lesson 1Document44 pagesHealth Assessment Lesson 1Bernice EbbiNo ratings yet
- Head Face Neck Eyes Ears ThroatDocument9 pagesHead Face Neck Eyes Ears ThroatDale Ros CollamatNo ratings yet
- ASESSMENT of Client With Diseases in Nervous SystemDocument16 pagesASESSMENT of Client With Diseases in Nervous SystemChristian San Jose TanNo ratings yet
- WEEK 3 - Head and NeckDocument22 pagesWEEK 3 - Head and NeckHashley CastellyNo ratings yet
- Extraoral Clinical Examination: Stature and Nutritional StatusDocument21 pagesExtraoral Clinical Examination: Stature and Nutritional StatusJheremy SolisNo ratings yet
- Physical AssessmentDocument7 pagesPhysical AssessmentRodolph Sean FamasNo ratings yet
- Newborn Exam Tutorial 5Document4 pagesNewborn Exam Tutorial 5Naomi OraengNo ratings yet
- Span RevisionDocument103 pagesSpan RevisionRolda FolkesNo ratings yet
- Ent AssessmentDocument23 pagesEnt AssessmentPdianghunNo ratings yet
- Pemeriksaan Fisik Kepala Dan LeherDocument39 pagesPemeriksaan Fisik Kepala Dan LeherdokteraanNo ratings yet
- Examination of The Head and Neck Is A Fundamental Part of The Standard Physical ExaminationDocument5 pagesExamination of The Head and Neck Is A Fundamental Part of The Standard Physical ExaminationDavidNo ratings yet
- 1rkippt - Physical AssessmentDocument36 pages1rkippt - Physical AssessmentIrfan NasrullahNo ratings yet
- Bates' Visual Guide To Physical Examination Vol. 7: Head, Eyes, and EarsDocument9 pagesBates' Visual Guide To Physical Examination Vol. 7: Head, Eyes, and EarsArlene DaroNo ratings yet
- Mass Casualty Incident MCIDocument20 pagesMass Casualty Incident MCIAiza Nicole BarelaNo ratings yet
- Module 2 Physical AssessmentDocument8 pagesModule 2 Physical AssessmentEsvinch EsvinchNo ratings yet
- OHNS--Otolaryngology; Head and Neck surgery: pocket field guideFrom EverandOHNS--Otolaryngology; Head and Neck surgery: pocket field guideNo ratings yet
- Oral Surgery Lec 5&6Document14 pagesOral Surgery Lec 5&6Mohammad RaadNo ratings yet
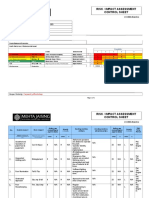
- Risk / Impact Assessment Control Sheet: CC/EHS/RA/014 ContractDocument4 pagesRisk / Impact Assessment Control Sheet: CC/EHS/RA/014 Contractsaurabh juwatkarNo ratings yet
- Bangladesh Barbados Bolivia Suriname TBPrize PDFDocument7 pagesBangladesh Barbados Bolivia Suriname TBPrize PDFRaheem Ullah KakarNo ratings yet
- Chrome Galvanize - AerosolDocument1 pageChrome Galvanize - AerosolJodyNo ratings yet
- PDF Rapid On Site Evaluation Rose A Practical Guide Guoping Cai Ebook Full ChapterDocument53 pagesPDF Rapid On Site Evaluation Rose A Practical Guide Guoping Cai Ebook Full Chapterjeffry.litzau621100% (1)
- CSL Recruitment 2024Document11 pagesCSL Recruitment 2024Chitikala RajeshNo ratings yet
- 3d Swot AnalysisDocument1 page3d Swot Analysisapi-491306234No ratings yet
- Mystery-Venusian Arts Handbook (Compact Edition) PDFDocument39 pagesMystery-Venusian Arts Handbook (Compact Edition) PDFjustnewaroundNo ratings yet
- Ord No.65 s.2007 Anti SmokingDocument12 pagesOrd No.65 s.2007 Anti SmokingDex CabalzaNo ratings yet
- Fabius Plus TD 9036798 enDocument172 pagesFabius Plus TD 9036798 enABDALLANo ratings yet
- Hiradc TableDocument1 pageHiradc TablejookapleeNo ratings yet
- Solid Waste Management Assessment ToolDocument2 pagesSolid Waste Management Assessment ToolMark RonanNo ratings yet
- FS Applying To The NDIS PDFDocument4 pagesFS Applying To The NDIS PDFAmmu JayanNo ratings yet
- DianPutriAliyya (2000026031)Document5 pagesDianPutriAliyya (2000026031)annawageNo ratings yet
- CG 2nd QuarterDocument9 pagesCG 2nd QuarterAura Anne Rose TanNo ratings yet
- 3D Printing AdvantagesDocument7 pages3D Printing AdvantagesionutmbNo ratings yet
- Ascorbic Acid Drug StudyDocument2 pagesAscorbic Acid Drug StudyJam Mohammad100% (5)
- NHIA - Hospital List - Jun2023Document22 pagesNHIA - Hospital List - Jun2023ilerioluwa akin-adeleyeNo ratings yet
- Contoh Soal PG Bahasa Inggris Kelas XI Semester 1 K13 Beserta JawabanDocument12 pagesContoh Soal PG Bahasa Inggris Kelas XI Semester 1 K13 Beserta JawabanIntan Wahyu DhamayantiNo ratings yet
- Front Office Report, Crimson HotelDocument75 pagesFront Office Report, Crimson HotelTravis AurelioNo ratings yet
- Personal StatementDocument2 pagesPersonal StatementTom Hayes67% (3)
- Postoperative HypocalsemiaDocument6 pagesPostoperative HypocalsemiaAdinda PasaribuNo ratings yet
- Hemoglobin Measured by Hemocue and A Reference Method in Venous and Capillary Blood: A Validation StudyDocument9 pagesHemoglobin Measured by Hemocue and A Reference Method in Venous and Capillary Blood: A Validation StudyMamad GGNo ratings yet
- Pink Flash Eyebrow - Google SearchDocument1 pagePink Flash Eyebrow - Google Searchserli altaNo ratings yet
- EAPP Week 1-5Document10 pagesEAPP Week 1-5Mon Rey B. DuranNo ratings yet
- Unit 4 First Aid-1Document8 pagesUnit 4 First Aid-1Muhammad Hamza HamzaNo ratings yet
- Cloning Technology-Bane or Boon To MankindDocument52 pagesCloning Technology-Bane or Boon To MankindDevain AroraNo ratings yet
- AIIMS Jodhpur Juniour Residents NoticeDocument4 pagesAIIMS Jodhpur Juniour Residents NoticeVijaya sharmaNo ratings yet
- Angelica Sanders ResumeDocument2 pagesAngelica Sanders Resumeapi-509815638No ratings yet