Download as pdf or txt
You might also like
- Pharmacy Calculation Workbook: 250 Questions to Prepare for the NAPLEX and PTCB ExamFrom EverandPharmacy Calculation Workbook: 250 Questions to Prepare for the NAPLEX and PTCB ExamRating: 5 out of 5 stars5/5 (2)
- Pedia TicklerDocument71 pagesPedia TicklermikayNo ratings yet
- Pedia NotesDocument9 pagesPedia NotesJitendra ChaudharyNo ratings yet
- Beta-Lactams Cephalosporins: Phenoxymethyl PenicillinDocument3 pagesBeta-Lactams Cephalosporins: Phenoxymethyl PenicillinBobet ReñaNo ratings yet
- Ok Ok Notes PediaDocument14 pagesOk Ok Notes PediaChristian PasicolanNo ratings yet
- Pedia EZ Notes PDFDocument102 pagesPedia EZ Notes PDFLuisa Paula LioanagNo ratings yet
- The Seven Habits of Highly Effective PeopleDocument60 pagesThe Seven Habits of Highly Effective PeopleBBCherriNo ratings yet
- Drugs and DosagesDocument4 pagesDrugs and DosagesDin-Din Que33% (3)
- TicklerDocument37 pagesTicklerLuis Elijah De CastroNo ratings yet
- Medical Intern S Handy NotesDocument23 pagesMedical Intern S Handy Notesdy dyNo ratings yet
- Pedia TicklerDocument66 pagesPedia TicklerCharles Jebb Belonio JuanitasNo ratings yet
- Notes On Common Pediatric Drugs FullDocument1 pageNotes On Common Pediatric Drugs FullfloramaeyecyecNo ratings yet
- TICKLER-PRINT Pedia PDFDocument8 pagesTICKLER-PRINT Pedia PDFCarlos H. AcuñaNo ratings yet
- Therapeutic Dosages For PEDIADocument7 pagesTherapeutic Dosages For PEDIAPatrick PalaypayonNo ratings yet
- Drugs For Tickler PDFDocument3 pagesDrugs For Tickler PDFBobet ReñaNo ratings yet
- Pedia Tickler 3Document24 pagesPedia Tickler 3Jane GarciaNo ratings yet
- Pedia TicklerDocument55 pagesPedia TicklerMa Louize Magbanua100% (1)
- BMC PediaDocument4 pagesBMC PediaRenette Uy100% (1)
- PediaidiotnotesDocument13 pagesPediaidiotnotesLeiza Tabora96% (23)
- Pedia NotesDocument3 pagesPedia NotesNikki DiocampoNo ratings yet
- Pedia NotesDocument2 pagesPedia NotesPaolo EvangelistaNo ratings yet
- Normal Values HR RR BPDocument28 pagesNormal Values HR RR BPKthrine CrronNo ratings yet
- Tickler Print PediaDocument8 pagesTickler Print PediaCarlos H. AcuñaNo ratings yet
- Pedia Idiot Notes 1Document12 pagesPedia Idiot Notes 1David JonesNo ratings yet
- Tickler 20print 202Document7 pagesTickler 20print 202Clav RamosNo ratings yet
- IV FLUIDS Drugs and DosagesDocument3 pagesIV FLUIDS Drugs and Dosagesdoc_geloNo ratings yet
- Drugs & DosagesDocument29 pagesDrugs & DosagesCristina VelasquezNo ratings yet
- Pedia ComputationsDocument5 pagesPedia ComputationsRheenz Fornoles100% (1)
- Pedia CardDocument4 pagesPedia CardPatricia Kate RegalaNo ratings yet
- Pedia Tickler 2 1 2Document106 pagesPedia Tickler 2 1 2Ma. Bernadette PinedaNo ratings yet
- TicklerDocument11 pagesTicklerJustine Issa YuNo ratings yet
- Common Drugs Used in The Out Patient DepartmentDocument1 pageCommon Drugs Used in The Out Patient DepartmentRenatoCosmeGalvanJuniorNo ratings yet
- Er Meds: DiclofenacDocument3 pagesEr Meds: Diclofenacmefav7778520No ratings yet
- ImportantPractical Notes PediaDocument11 pagesImportantPractical Notes PediaJun JunNo ratings yet
- Tickler Final PDFDocument29 pagesTickler Final PDFSerious LeoNo ratings yet
- Allergy and Immunology: Immunodeficiency 10 Warning Signs of ImmunodeficiencyDocument24 pagesAllergy and Immunology: Immunodeficiency 10 Warning Signs of Immunodeficiencyacque100% (2)
- Moonlighting 101Document20 pagesMoonlighting 101Dayanara Gener100% (1)
- Pedia TicklerDocument26 pagesPedia TicklerIsabelle SampangNo ratings yet
- Pedia NotesDocument11 pagesPedia NotesJohn Christopher Luces100% (1)
- Pedia NotesDocument97 pagesPedia NotesChristian Dave DoctoNo ratings yet
- Simplified Diagnostic Approach in Acute HepatitisDocument2 pagesSimplified Diagnostic Approach in Acute HepatitisJohn Christopher LucesNo ratings yet
- Pedia Notes Print2Document5 pagesPedia Notes Print2John Christopher LucesNo ratings yet
- Dem Tickler NotesDocument1 pageDem Tickler NotesSeff CausapinNo ratings yet
- Cheat Sheet (Draft)Document3 pagesCheat Sheet (Draft)bonziebuddyNo ratings yet
- Pedia NotesDocument7 pagesPedia NotesBonnyong MaNo ratings yet
- OB NotesDocument4 pagesOB NotesMaris Sarline OpenianoNo ratings yet
- Trans-Out Orders: NSVD Admitting Notes Postpartum OrdersDocument7 pagesTrans-Out Orders: NSVD Admitting Notes Postpartum OrdersDre ValdezNo ratings yet
- Moonlighting GuideDocument14 pagesMoonlighting GuideJulienneNo ratings yet
- OB Med Order KodigsDocument1 pageOB Med Order KodigsfloramaeyecyecNo ratings yet
- Pedia Revalida ReviewDocument83 pagesPedia Revalida Reviewcbac1990No ratings yet
- SURGERY Revalida Review 2019Document78 pagesSURGERY Revalida Review 2019anonymousNo ratings yet
- Notes For Pedia HandoutDocument2 pagesNotes For Pedia HandoutAiszel Angeli Pepito Ligo100% (2)
- Beta Lactams Macrolides: ST ND THDocument5 pagesBeta Lactams Macrolides: ST ND THRheenz FornolesNo ratings yet
- Pediatric DosageDocument2 pagesPediatric DosageAllene PaderangaNo ratings yet
- Notes On Common Pediatric Drugs, Dosaging and Package: For FeverDocument1 pageNotes On Common Pediatric Drugs, Dosaging and Package: For FeverMon DoceNo ratings yet
- Pedia Recommended DosageDocument5 pagesPedia Recommended DosageNerak LuNo ratings yet
- Opd Meds Jgej PDFDocument4 pagesOpd Meds Jgej PDFKaty SanchezNo ratings yet
- Pedia-TicklerDocument86 pagesPedia-TicklerPunsalan ChecaNo ratings yet
- Pedia TicklerDocument86 pagesPedia TicklerAnn Ross VidalNo ratings yet
- Common Medications and Computations in Pediatrics 1Document15 pagesCommon Medications and Computations in Pediatrics 1BelleNo ratings yet
- The Law of The Lord Is Perfect: Tes The Soul Ny Mo Ti Law The of Lord Fect, The Per Is of The Ing Vert Con TheDocument1 pageThe Law of The Lord Is Perfect: Tes The Soul Ny Mo Ti Law The of Lord Fect, The Per Is of The Ing Vert Con TheFG ArciagaNo ratings yet
- The Extremities and Spines: General ObjectivesDocument32 pagesThe Extremities and Spines: General ObjectivesFG ArciagaNo ratings yet
- Arciaga, FG - Ophtha Case Discussion 120622Document2 pagesArciaga, FG - Ophtha Case Discussion 120622FG ArciagaNo ratings yet
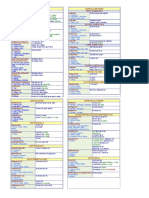
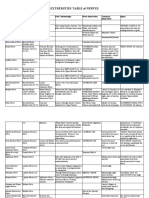
- Extremities Table of NervesDocument3 pagesExtremities Table of NervesFG ArciagaNo ratings yet
- Highest Blood Pressure Was 140/90 MMHGDocument5 pagesHighest Blood Pressure Was 140/90 MMHGFG ArciagaNo ratings yet
- Coronavirus GuidancecoinfectionsDocument2 pagesCoronavirus GuidancecoinfectionsFG ArciagaNo ratings yet
- Arciaga, FG-ParaSGD 063021Document4 pagesArciaga, FG-ParaSGD 063021FG ArciagaNo ratings yet
- Arciaga, FG - SGDPara 051221Document4 pagesArciaga, FG - SGDPara 051221FG ArciagaNo ratings yet
- Arciaga, FG - SGDMicroAnaerobesDocument7 pagesArciaga, FG - SGDMicroAnaerobesFG ArciagaNo ratings yet
- Arciaga, FG - PediaFC 051521Document10 pagesArciaga, FG - PediaFC 051521FG ArciagaNo ratings yet
- Cue and Clue Problem List and Initial Diagnosis PlanningDocument3 pagesCue and Clue Problem List and Initial Diagnosis PlanningWilujeng AnggrainiNo ratings yet
- The Role of Palliative Care at The End of LifeDocument6 pagesThe Role of Palliative Care at The End of LifeSvitlana YastremskaNo ratings yet
- ChakrasDocument44 pagesChakrasmiriNo ratings yet
- 5-Analyze The Role of Heredity and The EnvironmentDocument2 pages5-Analyze The Role of Heredity and The Environmentapi-295870335No ratings yet
- Non-Analgesic Effects of OpioidsDocument9 pagesNon-Analgesic Effects of OpioidsFrancisco MirettiNo ratings yet
- Pain Assessment 2020 ArticleDocument14 pagesPain Assessment 2020 Articlevcp2002No ratings yet
- pdf2 PDFDocument125 pagespdf2 PDFsushma shresthaNo ratings yet
- Discourse On Sex, Metasex, Ethics and Human SexualityDocument12 pagesDiscourse On Sex, Metasex, Ethics and Human SexualityPauline Fernandez100% (1)
- National Guideline For The Field Triage of Injured.19Document12 pagesNational Guideline For The Field Triage of Injured.19Vivi Permana SarieNo ratings yet
- Final Research ProposalDocument37 pagesFinal Research ProposalAhmed AbdoNo ratings yet
- Module 4 CytogeneticsDocument21 pagesModule 4 CytogeneticsFrances Riane SimoyNo ratings yet
- Curriculum Vitae: Khadeeja MunawarDocument6 pagesCurriculum Vitae: Khadeeja MunawarSohaib ArshadNo ratings yet
- Congestive Heart Failure 1 Concept Map !Document1 pageCongestive Heart Failure 1 Concept Map !Franklin A. Salaum IIINo ratings yet
- Effect of Preterm Infant Massage by The Mother On The Mood of Mothers Having Preterm InfantsDocument10 pagesEffect of Preterm Infant Massage by The Mother On The Mood of Mothers Having Preterm InfantsopanocayNo ratings yet
- Soal SMA Kelas 12 Bahasa Inggris SulitDocument10 pagesSoal SMA Kelas 12 Bahasa Inggris SulitsssssNo ratings yet
- NURS FPX 6610 Assessment 4 Case PresentationDocument5 pagesNURS FPX 6610 Assessment 4 Case Presentationjoohnsmith070No ratings yet
- Navigating The Gray Area: Managing Borderline Cases in OrthodonticsDocument6 pagesNavigating The Gray Area: Managing Borderline Cases in OrthodonticsInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Paediatric Cardiology: Post CSCST Training inDocument46 pagesPaediatric Cardiology: Post CSCST Training inmadimadi11No ratings yet
- Understanding of The Self - Sexual SelfDocument53 pagesUnderstanding of The Self - Sexual SelfDANE PIAMONTENo ratings yet
- The Process of Reproduction and Sexual Health and HygieneDocument28 pagesThe Process of Reproduction and Sexual Health and HygieneMila MagistradoNo ratings yet
- HLTH 499 Death Over Dinner Artifact 4Document5 pagesHLTH 499 Death Over Dinner Artifact 4api-582874658No ratings yet
- Asd Brochure - Michelle LauDocument5 pagesAsd Brochure - Michelle Lauapi-544801662No ratings yet
- Sample Examination Paper 1: Photosynthesis. Below Is An Outline of The Procedure The Students UsedDocument4 pagesSample Examination Paper 1: Photosynthesis. Below Is An Outline of The Procedure The Students UsedCarl Agape DavisNo ratings yet
- Middle Aged AdulthoodDocument2 pagesMiddle Aged AdulthoodDONITA DALUMPINESNo ratings yet
- Dimensions of Psychological Problems Replacing Diagnostic Categories With A More Science Based and Less Stigmatizing Alternative Lahey Full ChapterDocument68 pagesDimensions of Psychological Problems Replacing Diagnostic Categories With A More Science Based and Less Stigmatizing Alternative Lahey Full Chapteralla.adams464100% (17)
- UNIT - 2 Health Care Delivery SystemDocument177 pagesUNIT - 2 Health Care Delivery Systemraina menezesNo ratings yet
- Annotated BibliographyDocument3 pagesAnnotated BibliographySirJason AnaloNo ratings yet
- Name: Score:: Tomas Claudio Memorial College College of NursingDocument31 pagesName: Score:: Tomas Claudio Memorial College College of NursingOng, IvanNo ratings yet
- Abortus Habitualis Guideline PræsentationDocument26 pagesAbortus Habitualis Guideline PræsentationDurant HelonNo ratings yet
- Hypertensive Disorder in Pregnancy-5-19-2015-ZimbabweDocument39 pagesHypertensive Disorder in Pregnancy-5-19-2015-ZimbabwedanielNo ratings yet