
MedeAnalytics - Building A Hospital Scorecard - White Paper
MedeAnalytics - Building A Hospital Scorecard - White Paper
You might also like
- 2020 WHO Classification of Soft Tissue and Bone TumoursDocument617 pages2020 WHO Classification of Soft Tissue and Bone TumoursOlteanu Dragos-Nicolae91% (11)
- PharmaDoc Pharmacy AppDocument109 pagesPharmaDoc Pharmacy AppUsama Malik100% (1)
- ADEX. MP Resume Template 0604.12 (NY) .6.24.15 (1) (005) (002) (0B7)Document6 pagesADEX. MP Resume Template 0604.12 (NY) .6.24.15 (1) (005) (002) (0B7)Baniwas Marie AgnesNo ratings yet
- Bemsivir: 210 X 148 MM 210 X 148 MMDocument2 pagesBemsivir: 210 X 148 MM 210 X 148 MMSaifur Rahman SuzonNo ratings yet
- Presentation Fabrication of Storage TankDocument43 pagesPresentation Fabrication of Storage TankAbdul Manaf100% (1)
- Spiritual EmergencyDocument15 pagesSpiritual EmergencyClaudioRussoNo ratings yet
- Drug AddictionDocument19 pagesDrug Addictiontrigui amir100% (1)
- Impact of Applying Artificial Intelligence: Healthcare Professionals Insight (A Qualitative Survey Study in Hafr-Elbatin, Saudi Arabia)Document8 pagesImpact of Applying Artificial Intelligence: Healthcare Professionals Insight (A Qualitative Survey Study in Hafr-Elbatin, Saudi Arabia)IJAR JOURNALNo ratings yet
- Kims HospitalDocument547 pagesKims Hospitalmanish.wbsNo ratings yet
- Social Determinants of Health PDF - 3 Per Page NotesDocument8 pagesSocial Determinants of Health PDF - 3 Per Page Notesapi-657470217No ratings yet
- RetrieveDocument9 pagesRetrievebinabazighNo ratings yet
- Kiran Somshetwar CVDocument1 pageKiran Somshetwar CVGajananNo ratings yet
- Hemodynamics of Mechanical Circulatory SupportDocument12 pagesHemodynamics of Mechanical Circulatory Supportjairo enrique de la peña lopezNo ratings yet
- Premium Value FormularyDocument69 pagesPremium Value FormularyWalter PilimonNo ratings yet
- Research Study Tool Phototherapy enDocument25 pagesResearch Study Tool Phototherapy encarlos100% (1)
- Pharmacology of Heparin and Related Drugs: An UpdateDocument105 pagesPharmacology of Heparin and Related Drugs: An Updaterodcam1No ratings yet
- AstraZeneca AR 2018 PDFDocument248 pagesAstraZeneca AR 2018 PDFChristian nelNo ratings yet
- Unit 4 Ndds 7th SemesterDocument18 pagesUnit 4 Ndds 7th SemesterThe Aryan SharmaNo ratings yet
- Occupational Healt1Document119 pagesOccupational Healt1Krisna NoorNo ratings yet
- Cat 22 0269Document18 pagesCat 22 0269Dra. Elizabeth PaukerNo ratings yet
- History of Hospital-Acquired InfectionsDocument16 pagesHistory of Hospital-Acquired InfectionsRasha MuhammadNo ratings yet
- Cincinnati Police Department Survey ResultsDocument22 pagesCincinnati Police Department Survey ResultsSACoolidgeNo ratings yet
- 7 AHM Antibiotic PolicyDocument98 pages7 AHM Antibiotic PolicyfaisalNo ratings yet
- Python End Sem AnswerDocument23 pagesPython End Sem AnswerSahil Chauahan100% (1)
- MODULE 1 Overview of The InstitutionDocument45 pagesMODULE 1 Overview of The InstitutionShannen CostoNo ratings yet
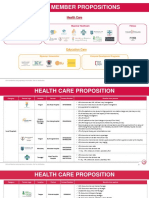
- Aia Member Propositions: Health CareDocument9 pagesAia Member Propositions: Health CareMin H. OONo ratings yet
- Cerner ListDocument9 pagesCerner ListDEIVEEGAN MATHINo ratings yet
- KLE Pharmacy - NPC Brochure 2022Document13 pagesKLE Pharmacy - NPC Brochure 2022Bhaskar PandeyNo ratings yet
- Treeage Pro Healthcare Module User'S ManualDocument164 pagesTreeage Pro Healthcare Module User'S ManualvanyadjNo ratings yet
- Getz Pharma Life and Times Newsletter Volume 13Document44 pagesGetz Pharma Life and Times Newsletter Volume 13Saman AbbasiNo ratings yet
- 2022 Indirect Procurementt ReportDocument44 pages2022 Indirect Procurementt ReportBlaze PanevNo ratings yet
- Big Data in Healthcare Systems and ResearchDocument4 pagesBig Data in Healthcare Systems and ResearchInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Booklet Clostridioides Difficile Infections Educational Booklet Offered by BiomerieuxDocument23 pagesBooklet Clostridioides Difficile Infections Educational Booklet Offered by BiomerieuxChs IvankarNo ratings yet
- Best Healthcare Payer Contract Negotiations TipsDocument10 pagesBest Healthcare Payer Contract Negotiations TipsZeeshana AliaNo ratings yet
- Survanta 25mg - ML Suspension - Summary of Product Characteristics (SMPC) - (Emc)Document7 pagesSurvanta 25mg - ML Suspension - Summary of Product Characteristics (SMPC) - (Emc)Mohadese hosseini zabetNo ratings yet
- Ajptr 102021 111Document16 pagesAjptr 102021 11188-pranjal VasavNo ratings yet
- A. I. in HealthcareDocument14 pagesA. I. in HealthcaremjNo ratings yet
- Product BookletDocument46 pagesProduct BookletNARESH JANDIALNo ratings yet
- Enhanced Recovery After Elective Caesarean A RapidDocument11 pagesEnhanced Recovery After Elective Caesarean A Rapidselfie rijalNo ratings yet
- Drug Discovery & Development Process by Piramal Pharma SolutionsDocument2 pagesDrug Discovery & Development Process by Piramal Pharma SolutionsAadityaRoyNo ratings yet
- Risk Management PolicyDocument19 pagesRisk Management PolicySonukrishnaNo ratings yet
- Benefit 1Document10 pagesBenefit 1HL LauNo ratings yet
- Disease Prediction Using Machine LearningDocument9 pagesDisease Prediction Using Machine LearningIJRASETPublicationsNo ratings yet
- Topic+3 Health+Sector+2023Document54 pagesTopic+3 Health+Sector+2023Fedelyn Mae Acaylar100% (1)
- Capstone Poster 2021 Chi NguyenDocument1 pageCapstone Poster 2021 Chi Nguyenapi-487551161No ratings yet
- 837P CMS 1500Document8 pages837P CMS 1500Gajapathi KNo ratings yet
- Chaps 9 and 2Document65 pagesChaps 9 and 2Lady DanielleNo ratings yet
- Latin America: Understanding Regulatory Compliance Requirements Across The Life Science Industry (Pharmaceuticals, Biologics, Medical Devices, IVDs)Document4 pagesLatin America: Understanding Regulatory Compliance Requirements Across The Life Science Industry (Pharmaceuticals, Biologics, Medical Devices, IVDs)ComplianceOnlineNo ratings yet
- Oracle® Health Sciences Clinical One Platform: Sponsor and CRO User GuideDocument297 pagesOracle® Health Sciences Clinical One Platform: Sponsor and CRO User GuideArjun TalwakarNo ratings yet
- Newsletter-Fall21-Links 1Document15 pagesNewsletter-Fall21-Links 1api-398712370No ratings yet
- Theatre Operational PolicyDocument26 pagesTheatre Operational PolicyEmma Sunday OdyenyNo ratings yet
- WEEK 1 Drug Development and Ethical ConsiderationsDocument142 pagesWEEK 1 Drug Development and Ethical ConsiderationsMaureen CuartoNo ratings yet
- UntitledDocument4,686 pagesUntitledAng'ila JuniorNo ratings yet
- Delivering Cloud-Based Solutions For Hospitals, Physicians, Clinics, Patients, and PopulationDocument4 pagesDelivering Cloud-Based Solutions For Hospitals, Physicians, Clinics, Patients, and PopulationsomyaNo ratings yet
- Nursing ResearchDocument21 pagesNursing ResearchMargareth SaquibalNo ratings yet
- Pharmacy Informatics and Healthcare Data Analytics Week 4 Pharmacy Claims Data Update 5-14-22Document24 pagesPharmacy Informatics and Healthcare Data Analytics Week 4 Pharmacy Claims Data Update 5-14-22andreaNo ratings yet
- AACN BSN Essentials PaperDocument9 pagesAACN BSN Essentials PaperSikany S EmmanNo ratings yet
- Pharmacy Cbahi Questions 2022Document12 pagesPharmacy Cbahi Questions 2022osama hosni100% (1)
- 4.3 InfectiousDocument29 pages4.3 InfectiousJohn Anthony de GùzmanNo ratings yet
- Quality AssuranceDocument15 pagesQuality AssurancePallabi BhaktaNo ratings yet
- IVF Treatment InsuranceDocument7 pagesIVF Treatment InsuranceindoreinfertilityclinicNo ratings yet
- Health Information Systems Utilization: A Comparison of Extent and Magnitude in Public and Private Health Facilities in Dar Es Salaam, TanzaniaDocument10 pagesHealth Information Systems Utilization: A Comparison of Extent and Magnitude in Public and Private Health Facilities in Dar Es Salaam, TanzaniaAJHSSR JournalNo ratings yet
- EDI ERP and DSSDocument5 pagesEDI ERP and DSSLowell DuranoNo ratings yet
- Paint IndustryDocument2 pagesPaint IndustryitseaziNo ratings yet
- Masterpact NT12 H1 User ManualDocument56 pagesMasterpact NT12 H1 User ManualSlaxNo ratings yet
- Research Paper On Greenhouse Effect PDFDocument8 pagesResearch Paper On Greenhouse Effect PDFgz8reqdc100% (1)
- General Chemistry 2Document10 pagesGeneral Chemistry 2Aubrey GuilaranNo ratings yet
- Fish MorphologyDocument9 pagesFish Morphologydev_sharma1986100% (1)
- Production & Operation Management - POM PDFDocument4 pagesProduction & Operation Management - POM PDFHiren Kotadia0% (2)
- Uenr8357uenr8357 SisDocument8 pagesUenr8357uenr8357 Sisjhonas del marNo ratings yet
- Bomb Calorimeter TheoryDocument2 pagesBomb Calorimeter TheoryTub Pitthayuth33% (3)
- Satip X 600 02Document15 pagesSatip X 600 02spravin231No ratings yet
- List of Periodic Checks Life Saving & Fire Fighting EquipmentDocument5 pagesList of Periodic Checks Life Saving & Fire Fighting EquipmentSandro CheNo ratings yet
- Cerebrovascular AccidentDocument42 pagesCerebrovascular AccidentGideon HaburaNo ratings yet
- Jocd 18 1215Document9 pagesJocd 18 1215vanessa_werbickyNo ratings yet
- 1 - FLD-25 3D Printer Filament MachineDocument11 pages1 - FLD-25 3D Printer Filament MachineNitin PatilNo ratings yet
- BookAppointmentTest CareV2 Silver. 1579881536.8462949Document1 pageBookAppointmentTest CareV2 Silver. 1579881536.8462949ankitNo ratings yet
- Bass Drum TechniqueDocument5 pagesBass Drum TechniqueRudy LievensNo ratings yet
- De Ce of Eterm Emen F The Mina NT by e Solu Ation y Pho Ubiliz Nofa Otom Zed P Alum Metric Prod Inum C Titr Uct Min Ratio NDocument2 pagesDe Ce of Eterm Emen F The Mina NT by e Solu Ation y Pho Ubiliz Nofa Otom Zed P Alum Metric Prod Inum C Titr Uct Min Ratio NRomy Iván Cruz VillarroelNo ratings yet
- Fall 2023 Grad TimetableDocument41 pagesFall 2023 Grad TimetableUsman AliNo ratings yet
- Disturbance in Sensory PerceptionDocument48 pagesDisturbance in Sensory PerceptionKristine Louise JavierNo ratings yet
- Phytochemical Screening and CharacterizationDocument5 pagesPhytochemical Screening and CharacterizationyamunaraviNo ratings yet
- Contract of ServiceDocument2 pagesContract of ServiceAnonymous 03JIPKRkNo ratings yet
- Fat Loss ProgramDocument2 pagesFat Loss Programrifkarofiah1No ratings yet
- J. Konvitz - Don't Waste A Crisis 2020-04-20Document48 pagesJ. Konvitz - Don't Waste A Crisis 2020-04-20Fondapol100% (1)
- Contents and Front Matter PDFDocument13 pagesContents and Front Matter PDFAbdelrhman MadyNo ratings yet
- Food Facility Self Inspection ChecklistDocument2 pagesFood Facility Self Inspection Checklistmelisizwe2016No ratings yet
- The Winners and Losers of GlobalizationDocument7 pagesThe Winners and Losers of GlobalizationRalucutsaNo ratings yet
- Analisis Efektivitas Biaya Kombinasi Obat Antihipertensi Pada Pasien Rawat Inap Di Rsud Dr. Soekardjo TasikmalayaDocument10 pagesAnalisis Efektivitas Biaya Kombinasi Obat Antihipertensi Pada Pasien Rawat Inap Di Rsud Dr. Soekardjo TasikmalayaEmiNo ratings yet
- Fibertec 1023 Solution Brochure ENDocument2 pagesFibertec 1023 Solution Brochure ENrani hindiNo ratings yet























































































Download as pdf or txt
You might also like
- 2020 WHO Classification of Soft Tissue and Bone TumoursDocument617 pages2020 WHO Classification of Soft Tissue and Bone TumoursOlteanu Dragos-Nicolae91% (11)
- PharmaDoc Pharmacy AppDocument109 pagesPharmaDoc Pharmacy AppUsama Malik100% (1)
- ADEX. MP Resume Template 0604.12 (NY) .6.24.15 (1) (005) (002) (0B7)Document6 pagesADEX. MP Resume Template 0604.12 (NY) .6.24.15 (1) (005) (002) (0B7)Baniwas Marie AgnesNo ratings yet
- Bemsivir: 210 X 148 MM 210 X 148 MMDocument2 pagesBemsivir: 210 X 148 MM 210 X 148 MMSaifur Rahman SuzonNo ratings yet
- Presentation Fabrication of Storage TankDocument43 pagesPresentation Fabrication of Storage TankAbdul Manaf100% (1)
- Spiritual EmergencyDocument15 pagesSpiritual EmergencyClaudioRussoNo ratings yet
- Drug AddictionDocument19 pagesDrug Addictiontrigui amir100% (1)
- Impact of Applying Artificial Intelligence: Healthcare Professionals Insight (A Qualitative Survey Study in Hafr-Elbatin, Saudi Arabia)Document8 pagesImpact of Applying Artificial Intelligence: Healthcare Professionals Insight (A Qualitative Survey Study in Hafr-Elbatin, Saudi Arabia)IJAR JOURNALNo ratings yet
- Kims HospitalDocument547 pagesKims Hospitalmanish.wbsNo ratings yet
- Social Determinants of Health PDF - 3 Per Page NotesDocument8 pagesSocial Determinants of Health PDF - 3 Per Page Notesapi-657470217No ratings yet
- RetrieveDocument9 pagesRetrievebinabazighNo ratings yet
- Kiran Somshetwar CVDocument1 pageKiran Somshetwar CVGajananNo ratings yet
- Hemodynamics of Mechanical Circulatory SupportDocument12 pagesHemodynamics of Mechanical Circulatory Supportjairo enrique de la peña lopezNo ratings yet
- Premium Value FormularyDocument69 pagesPremium Value FormularyWalter PilimonNo ratings yet
- Research Study Tool Phototherapy enDocument25 pagesResearch Study Tool Phototherapy encarlos100% (1)
- Pharmacology of Heparin and Related Drugs: An UpdateDocument105 pagesPharmacology of Heparin and Related Drugs: An Updaterodcam1No ratings yet
- AstraZeneca AR 2018 PDFDocument248 pagesAstraZeneca AR 2018 PDFChristian nelNo ratings yet
- Unit 4 Ndds 7th SemesterDocument18 pagesUnit 4 Ndds 7th SemesterThe Aryan SharmaNo ratings yet
- Occupational Healt1Document119 pagesOccupational Healt1Krisna NoorNo ratings yet
- Cat 22 0269Document18 pagesCat 22 0269Dra. Elizabeth PaukerNo ratings yet
- History of Hospital-Acquired InfectionsDocument16 pagesHistory of Hospital-Acquired InfectionsRasha MuhammadNo ratings yet
- Cincinnati Police Department Survey ResultsDocument22 pagesCincinnati Police Department Survey ResultsSACoolidgeNo ratings yet
- 7 AHM Antibiotic PolicyDocument98 pages7 AHM Antibiotic PolicyfaisalNo ratings yet
- Python End Sem AnswerDocument23 pagesPython End Sem AnswerSahil Chauahan100% (1)
- MODULE 1 Overview of The InstitutionDocument45 pagesMODULE 1 Overview of The InstitutionShannen CostoNo ratings yet
- Aia Member Propositions: Health CareDocument9 pagesAia Member Propositions: Health CareMin H. OONo ratings yet
- Cerner ListDocument9 pagesCerner ListDEIVEEGAN MATHINo ratings yet
- KLE Pharmacy - NPC Brochure 2022Document13 pagesKLE Pharmacy - NPC Brochure 2022Bhaskar PandeyNo ratings yet
- Treeage Pro Healthcare Module User'S ManualDocument164 pagesTreeage Pro Healthcare Module User'S ManualvanyadjNo ratings yet
- Getz Pharma Life and Times Newsletter Volume 13Document44 pagesGetz Pharma Life and Times Newsletter Volume 13Saman AbbasiNo ratings yet
- 2022 Indirect Procurementt ReportDocument44 pages2022 Indirect Procurementt ReportBlaze PanevNo ratings yet
- Big Data in Healthcare Systems and ResearchDocument4 pagesBig Data in Healthcare Systems and ResearchInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Booklet Clostridioides Difficile Infections Educational Booklet Offered by BiomerieuxDocument23 pagesBooklet Clostridioides Difficile Infections Educational Booklet Offered by BiomerieuxChs IvankarNo ratings yet
- Best Healthcare Payer Contract Negotiations TipsDocument10 pagesBest Healthcare Payer Contract Negotiations TipsZeeshana AliaNo ratings yet
- Survanta 25mg - ML Suspension - Summary of Product Characteristics (SMPC) - (Emc)Document7 pagesSurvanta 25mg - ML Suspension - Summary of Product Characteristics (SMPC) - (Emc)Mohadese hosseini zabetNo ratings yet
- Ajptr 102021 111Document16 pagesAjptr 102021 11188-pranjal VasavNo ratings yet
- A. I. in HealthcareDocument14 pagesA. I. in HealthcaremjNo ratings yet
- Product BookletDocument46 pagesProduct BookletNARESH JANDIALNo ratings yet
- Enhanced Recovery After Elective Caesarean A RapidDocument11 pagesEnhanced Recovery After Elective Caesarean A Rapidselfie rijalNo ratings yet
- Drug Discovery & Development Process by Piramal Pharma SolutionsDocument2 pagesDrug Discovery & Development Process by Piramal Pharma SolutionsAadityaRoyNo ratings yet
- Risk Management PolicyDocument19 pagesRisk Management PolicySonukrishnaNo ratings yet
- Benefit 1Document10 pagesBenefit 1HL LauNo ratings yet
- Disease Prediction Using Machine LearningDocument9 pagesDisease Prediction Using Machine LearningIJRASETPublicationsNo ratings yet
- Topic+3 Health+Sector+2023Document54 pagesTopic+3 Health+Sector+2023Fedelyn Mae Acaylar100% (1)
- Capstone Poster 2021 Chi NguyenDocument1 pageCapstone Poster 2021 Chi Nguyenapi-487551161No ratings yet
- 837P CMS 1500Document8 pages837P CMS 1500Gajapathi KNo ratings yet
- Chaps 9 and 2Document65 pagesChaps 9 and 2Lady DanielleNo ratings yet
- Latin America: Understanding Regulatory Compliance Requirements Across The Life Science Industry (Pharmaceuticals, Biologics, Medical Devices, IVDs)Document4 pagesLatin America: Understanding Regulatory Compliance Requirements Across The Life Science Industry (Pharmaceuticals, Biologics, Medical Devices, IVDs)ComplianceOnlineNo ratings yet
- Oracle® Health Sciences Clinical One Platform: Sponsor and CRO User GuideDocument297 pagesOracle® Health Sciences Clinical One Platform: Sponsor and CRO User GuideArjun TalwakarNo ratings yet
- Newsletter-Fall21-Links 1Document15 pagesNewsletter-Fall21-Links 1api-398712370No ratings yet
- Theatre Operational PolicyDocument26 pagesTheatre Operational PolicyEmma Sunday OdyenyNo ratings yet
- WEEK 1 Drug Development and Ethical ConsiderationsDocument142 pagesWEEK 1 Drug Development and Ethical ConsiderationsMaureen CuartoNo ratings yet
- UntitledDocument4,686 pagesUntitledAng'ila JuniorNo ratings yet
- Delivering Cloud-Based Solutions For Hospitals, Physicians, Clinics, Patients, and PopulationDocument4 pagesDelivering Cloud-Based Solutions For Hospitals, Physicians, Clinics, Patients, and PopulationsomyaNo ratings yet
- Nursing ResearchDocument21 pagesNursing ResearchMargareth SaquibalNo ratings yet
- Pharmacy Informatics and Healthcare Data Analytics Week 4 Pharmacy Claims Data Update 5-14-22Document24 pagesPharmacy Informatics and Healthcare Data Analytics Week 4 Pharmacy Claims Data Update 5-14-22andreaNo ratings yet
- AACN BSN Essentials PaperDocument9 pagesAACN BSN Essentials PaperSikany S EmmanNo ratings yet
- Pharmacy Cbahi Questions 2022Document12 pagesPharmacy Cbahi Questions 2022osama hosni100% (1)
- 4.3 InfectiousDocument29 pages4.3 InfectiousJohn Anthony de GùzmanNo ratings yet
- Quality AssuranceDocument15 pagesQuality AssurancePallabi BhaktaNo ratings yet
- IVF Treatment InsuranceDocument7 pagesIVF Treatment InsuranceindoreinfertilityclinicNo ratings yet
- Health Information Systems Utilization: A Comparison of Extent and Magnitude in Public and Private Health Facilities in Dar Es Salaam, TanzaniaDocument10 pagesHealth Information Systems Utilization: A Comparison of Extent and Magnitude in Public and Private Health Facilities in Dar Es Salaam, TanzaniaAJHSSR JournalNo ratings yet
- EDI ERP and DSSDocument5 pagesEDI ERP and DSSLowell DuranoNo ratings yet
- Paint IndustryDocument2 pagesPaint IndustryitseaziNo ratings yet
- Masterpact NT12 H1 User ManualDocument56 pagesMasterpact NT12 H1 User ManualSlaxNo ratings yet
- Research Paper On Greenhouse Effect PDFDocument8 pagesResearch Paper On Greenhouse Effect PDFgz8reqdc100% (1)
- General Chemistry 2Document10 pagesGeneral Chemistry 2Aubrey GuilaranNo ratings yet
- Fish MorphologyDocument9 pagesFish Morphologydev_sharma1986100% (1)
- Production & Operation Management - POM PDFDocument4 pagesProduction & Operation Management - POM PDFHiren Kotadia0% (2)
- Uenr8357uenr8357 SisDocument8 pagesUenr8357uenr8357 Sisjhonas del marNo ratings yet
- Bomb Calorimeter TheoryDocument2 pagesBomb Calorimeter TheoryTub Pitthayuth33% (3)
- Satip X 600 02Document15 pagesSatip X 600 02spravin231No ratings yet
- List of Periodic Checks Life Saving & Fire Fighting EquipmentDocument5 pagesList of Periodic Checks Life Saving & Fire Fighting EquipmentSandro CheNo ratings yet
- Cerebrovascular AccidentDocument42 pagesCerebrovascular AccidentGideon HaburaNo ratings yet
- Jocd 18 1215Document9 pagesJocd 18 1215vanessa_werbickyNo ratings yet
- 1 - FLD-25 3D Printer Filament MachineDocument11 pages1 - FLD-25 3D Printer Filament MachineNitin PatilNo ratings yet
- BookAppointmentTest CareV2 Silver. 1579881536.8462949Document1 pageBookAppointmentTest CareV2 Silver. 1579881536.8462949ankitNo ratings yet
- Bass Drum TechniqueDocument5 pagesBass Drum TechniqueRudy LievensNo ratings yet
- De Ce of Eterm Emen F The Mina NT by e Solu Ation y Pho Ubiliz Nofa Otom Zed P Alum Metric Prod Inum C Titr Uct Min Ratio NDocument2 pagesDe Ce of Eterm Emen F The Mina NT by e Solu Ation y Pho Ubiliz Nofa Otom Zed P Alum Metric Prod Inum C Titr Uct Min Ratio NRomy Iván Cruz VillarroelNo ratings yet
- Fall 2023 Grad TimetableDocument41 pagesFall 2023 Grad TimetableUsman AliNo ratings yet
- Disturbance in Sensory PerceptionDocument48 pagesDisturbance in Sensory PerceptionKristine Louise JavierNo ratings yet
- Phytochemical Screening and CharacterizationDocument5 pagesPhytochemical Screening and CharacterizationyamunaraviNo ratings yet
- Contract of ServiceDocument2 pagesContract of ServiceAnonymous 03JIPKRkNo ratings yet
- Fat Loss ProgramDocument2 pagesFat Loss Programrifkarofiah1No ratings yet
- J. Konvitz - Don't Waste A Crisis 2020-04-20Document48 pagesJ. Konvitz - Don't Waste A Crisis 2020-04-20Fondapol100% (1)
- Contents and Front Matter PDFDocument13 pagesContents and Front Matter PDFAbdelrhman MadyNo ratings yet
- Food Facility Self Inspection ChecklistDocument2 pagesFood Facility Self Inspection Checklistmelisizwe2016No ratings yet
- The Winners and Losers of GlobalizationDocument7 pagesThe Winners and Losers of GlobalizationRalucutsaNo ratings yet
- Analisis Efektivitas Biaya Kombinasi Obat Antihipertensi Pada Pasien Rawat Inap Di Rsud Dr. Soekardjo TasikmalayaDocument10 pagesAnalisis Efektivitas Biaya Kombinasi Obat Antihipertensi Pada Pasien Rawat Inap Di Rsud Dr. Soekardjo TasikmalayaEmiNo ratings yet
- Fibertec 1023 Solution Brochure ENDocument2 pagesFibertec 1023 Solution Brochure ENrani hindiNo ratings yet