Download as pdf or txt
You might also like
- Edexcel As Biology Revision Guide PDF FreeDocument108 pagesEdexcel As Biology Revision Guide PDF Freebody fayez100% (1)
- The Original Backnobber II Tool: User GuideDocument37 pagesThe Original Backnobber II Tool: User GuideAl BnNo ratings yet
- Obstetrics and Gynecology NOTESDocument73 pagesObstetrics and Gynecology NOTESAwais Awais100% (6)
- Osce Orthopedic Year 4Document3 pagesOsce Orthopedic Year 4Mazia Nadia Khairudin100% (9)
- AMETROPIADocument48 pagesAMETROPIARahul KirkNo ratings yet
- REFRACTIVE ERRORSDocument45 pagesREFRACTIVE ERRORSDrSuganthi AKNo ratings yet
- Refractive ErrorsDocument33 pagesRefractive ErrorsMathew Sebastian100% (3)
- Myopia SimpleDocument11 pagesMyopia SimpleburagohainaviNo ratings yet
- Gradual Loss of Vision-Nurses - 065937Document73 pagesGradual Loss of Vision-Nurses - 065937CosbyNo ratings yet
- Degenerative MyopiaDocument53 pagesDegenerative MyopiaNiloy BasakNo ratings yet
- DR Ajai Agrawal Additional Professor Department of Ophthalmology AIIMS RishikeshDocument48 pagesDR Ajai Agrawal Additional Professor Department of Ophthalmology AIIMS RishikeshSrishti KhullarNo ratings yet
- Lecture 11 Special Senses Part 6-VisionDocument48 pagesLecture 11 Special Senses Part 6-VisionMoses Jr KazevuNo ratings yet
- Ug Class Refractive Error 28-02Document60 pagesUg Class Refractive Error 28-02Writabrata RoyNo ratings yet
- Vision LossDocument56 pagesVision LossIsraa AlaaNo ratings yet
- Opthalmic Emergencies PresentationDocument85 pagesOpthalmic Emergencies PresentationvictoreffiomNo ratings yet
- Secondary Angle Closure GlaucomaDocument35 pagesSecondary Angle Closure GlaucomaAndriati NadhilaNo ratings yet
- Refractive Disorders Blok VisualDocument27 pagesRefractive Disorders Blok Visualmuhammad ajiNo ratings yet
- L6 Refractive Errors and PaedsDocument37 pagesL6 Refractive Errors and PaedsSofíaGriggsNo ratings yet
- Congenital CataractDocument27 pagesCongenital CataractbharatpurhosNo ratings yet
- Glaucoma: Defitaria Permatasari I11109005Document46 pagesGlaucoma: Defitaria Permatasari I11109005yusufharkianNo ratings yet
- Glaucoma: Consultant OphthalmologistDocument45 pagesGlaucoma: Consultant OphthalmologistGladys MainaNo ratings yet
- A Child Presenting With Visual Impairment 28/4/2020Document40 pagesA Child Presenting With Visual Impairment 28/4/2020Sindhu BabuNo ratings yet
- Chapter 11 Eye & Vision DisordersDocument72 pagesChapter 11 Eye & Vision DisordersMYLENE GRACE ELARCOSANo ratings yet
- InggrisDocument32 pagesInggrisRani Dwi HapsariNo ratings yet
- Errors of RefractionDocument34 pagesErrors of RefractionKhushi kansalNo ratings yet
- MyopiaDocument9 pagesMyopiaNavani TharanNo ratings yet
- Vision Impairment 1Document59 pagesVision Impairment 1122ritik goyalNo ratings yet
- Concomitant Squint: Noor Asmah MD Azmi Optometrist HsahDocument56 pagesConcomitant Squint: Noor Asmah MD Azmi Optometrist HsahAnonymous l2Fve4PpD33% (3)
- Opthalmoloy PDFDocument10 pagesOpthalmoloy PDFdrshekarforyouNo ratings yet
- 30secondary GlaucomasDocument19 pages30secondary GlaucomasShari' Si WahyuNo ratings yet
- MYOPIADocument21 pagesMYOPIARimi Sree DasNo ratings yet
- GLAUKOMADocument47 pagesGLAUKOMARahma GhnNo ratings yet
- Congenital Glaucoma FinalDocument48 pagesCongenital Glaucoma FinalMona MohammedNo ratings yet
- Glaucoma & CataractDocument53 pagesGlaucoma & CataractBenita100% (1)
- Impaired Vision and BlindnessDocument44 pagesImpaired Vision and BlindnessYujenNo ratings yet
- RefraksiDocument84 pagesRefraksinaroetocapkutilNo ratings yet
- Ophthalmology EmergenciesDocument60 pagesOphthalmology Emergenciesasraf amirullahNo ratings yet
- HeterophoriaDocument25 pagesHeterophoriatehreem tanveerNo ratings yet
- OPTIC NEURITISDocument3 pagesOPTIC NEURITISshreyan.daniNo ratings yet
- GlaucomaDocument79 pagesGlaucomaranjan6602No ratings yet
- Presentation 2Document57 pagesPresentation 2medhanit anjuloNo ratings yet
- Ent Lesson 8Document45 pagesEnt Lesson 8favourednancie9No ratings yet
- EXOTROPIADocument20 pagesEXOTROPIAjay daxiniNo ratings yet
- 03 Eyes and Ears 2 1Document62 pages03 Eyes and Ears 2 1Gerald BatugalNo ratings yet
- Assessment and Management of Patients With Eye andDocument86 pagesAssessment and Management of Patients With Eye andEsmareldah Henry SirueNo ratings yet
- 1 CataractDocument31 pages1 CataractsnehalNo ratings yet
- Objective - Subjective Eye Examination-Referral System and When To ReferDocument56 pagesObjective - Subjective Eye Examination-Referral System and When To ReferClara Sainuka100% (1)
- Cataract: BY: Huda Hamdan Rubaalsheyab Maramalanbar AbeerhussainDocument59 pagesCataract: BY: Huda Hamdan Rubaalsheyab Maramalanbar AbeerhussainaliNo ratings yet
- Glaucoma FinalDocument40 pagesGlaucoma FinalAdoma SportsNo ratings yet
- DT LeukocoriaDocument43 pagesDT LeukocoriadeyshieNo ratings yet
- Ophthalmology Clerks: Alea, Denz Marc Custodio, Audreyfil Perez, Francis MiguelDocument14 pagesOphthalmology Clerks: Alea, Denz Marc Custodio, Audreyfil Perez, Francis MiguelDenz Marc AleaNo ratings yet
- 30secondary GlaucomasDocument15 pages30secondary GlaucomasShari' Si WahyuNo ratings yet
- Central Serous Retinopathy PPT-2Document28 pagesCentral Serous Retinopathy PPT-2Vaishu SgsNo ratings yet
- Open Open Ophtha For The Non OphthaDocument54 pagesOpen Open Ophtha For The Non OphthaVersion 1No ratings yet
- HypermetropiaDocument9 pagesHypermetropiaHana SetianingsihNo ratings yet
- Cataract: Done by Mo3taz Abu Rabiah A7mad LubaniDocument46 pagesCataract: Done by Mo3taz Abu Rabiah A7mad LubaniMaxwell C Jay KafwaniNo ratings yet
- Cataracts: ClassificationDocument9 pagesCataracts: ClassificationRafay ChacharNo ratings yet
- Eye Disorders: Structure of The EyeDocument13 pagesEye Disorders: Structure of The Eyeapi-3822433No ratings yet
- OT 677 Conditions Lecture 3Document66 pagesOT 677 Conditions Lecture 3Yuvaraaj NavaneethakrishnanNo ratings yet
- Ophthalmology - Optics and RefractionDocument10 pagesOphthalmology - Optics and RefractionjbtcmdtjjvNo ratings yet
- Eye Diseases Ppt. 2024Document43 pagesEye Diseases Ppt. 2024Sri Ram 07No ratings yet
- Double Vision / Diplopia: Dr. R. Handoko Pratomo, SPMDocument94 pagesDouble Vision / Diplopia: Dr. R. Handoko Pratomo, SPMNefri TiawarmanNo ratings yet
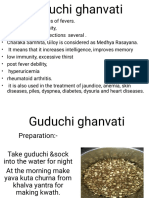
- Gudhuchi GhanvatiDocument7 pagesGudhuchi GhanvatiDrashti ChudasamaNo ratings yet
- UntitledDocument1 pageUntitledDrashti ChudasamaNo ratings yet
- UntitledDocument41 pagesUntitledDrashti ChudasamaNo ratings yet
- UntitledDocument15 pagesUntitledDrashti ChudasamaNo ratings yet
- Presented By:-: Dr. Preetam SahuDocument68 pagesPresented By:-: Dr. Preetam SahuDrashti ChudasamaNo ratings yet
- UntitledDocument12 pagesUntitledDrashti ChudasamaNo ratings yet
- Thyroid Disorders: Presented By:-Drashti Chudasama Guided By:-Dr. Milan SirDocument44 pagesThyroid Disorders: Presented By:-Drashti Chudasama Guided By:-Dr. Milan SirDrashti ChudasamaNo ratings yet
- Retina & Its DisorderDocument9 pagesRetina & Its DisorderDrashti ChudasamaNo ratings yet
- Government of Gujarat: Student Basic DetailsDocument3 pagesGovernment of Gujarat: Student Basic DetailsDrashti ChudasamaNo ratings yet
- Government of Gujarat: Student Personal DetailsDocument3 pagesGovernment of Gujarat: Student Personal DetailsDrashti ChudasamaNo ratings yet
- Government of Gujarat: Student Basic DetailsDocument3 pagesGovernment of Gujarat: Student Basic DetailsDrashti ChudasamaNo ratings yet
- Tax Invoice/Bill of Supply/Cash Memo: (Original For Recipient)Document1 pageTax Invoice/Bill of Supply/Cash Memo: (Original For Recipient)Drashti ChudasamaNo ratings yet
- 0 Tooth ExtractionDocument22 pages0 Tooth ExtractionDrashti ChudasamaNo ratings yet
- First Letter Last Name GameDocument6 pagesFirst Letter Last Name Gameapi-374841402No ratings yet
- 29 The EyeDocument12 pages29 The EyeFrinz RubioNo ratings yet
- Reaction Paper My Journey With Covid 19 PandemicDocument2 pagesReaction Paper My Journey With Covid 19 PandemicJohn Ralph CaguladaNo ratings yet
- Blood Bank Homework IDocument3 pagesBlood Bank Homework IMohamed MounirNo ratings yet
- Dr. DEEPAK.N.S (PG), Dr. PAGADPALLY SRINIVAS (Professor & Head) Dept. of Paediatrics, VMMC, KKLDocument2 pagesDr. DEEPAK.N.S (PG), Dr. PAGADPALLY SRINIVAS (Professor & Head) Dept. of Paediatrics, VMMC, KKLSumanth KumarNo ratings yet
- RH PATHO2022 - (Chapt 02 - Cell Injury, Death, Adaptations - A)Document9 pagesRH PATHO2022 - (Chapt 02 - Cell Injury, Death, Adaptations - A)Toka AlzoubiNo ratings yet
- Health-Related Quality of Life in Children With Congenital Adrenal HyperplasiaDocument7 pagesHealth-Related Quality of Life in Children With Congenital Adrenal Hyperplasiadiah budiartiNo ratings yet
- VNSG 1409 - Exam 3Document24 pagesVNSG 1409 - Exam 3luna nguyenNo ratings yet
- OET Writing Case Notes Nursing 16 35Document38 pagesOET Writing Case Notes Nursing 16 35adnanshakeelm1No ratings yet
- Breastfeeding, Physical Growth, and Cognitive DevelopmentDocument12 pagesBreastfeeding, Physical Growth, and Cognitive DevelopmentSebastiano SegaNo ratings yet
- CestodesDocument5 pagesCestodesGhina RizwanNo ratings yet
- Vulval CancerDocument9 pagesVulval CancerSana LodhiNo ratings yet
- English Medical VocabularyDocument2 pagesEnglish Medical VocabularysologuebNo ratings yet
- Functional Constipation: A Case Report: EpartmentDocument5 pagesFunctional Constipation: A Case Report: EpartmentArielIzaSuquilloNo ratings yet
- Session Schedule 20.4.2023Document32 pagesSession Schedule 20.4.2023Aditya RaiNo ratings yet
- Clinical Profile of Acute BronchiolitisDocument4 pagesClinical Profile of Acute BronchiolitisInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Arabic To Communicate With PatientsDocument19 pagesArabic To Communicate With PatientsDK Aquino GomezNo ratings yet
- Vita Vita: Joshua'S "Extreme"Document32 pagesVita Vita: Joshua'S "Extreme"Michael DennisNo ratings yet
- Bloodbld 2019003808 CDocument12 pagesBloodbld 2019003808 CBillal BenhaddadNo ratings yet
- Related Teenshealth Links: Health Problems SeriesDocument13 pagesRelated Teenshealth Links: Health Problems SeriesMario BadayosNo ratings yet
- Eap-Media-Mongolia Air Pollution Crisis ENGDocument82 pagesEap-Media-Mongolia Air Pollution Crisis ENGС. ЭнхмөрөнNo ratings yet
- Nomenklatur IBS Edit THTDocument291 pagesNomenklatur IBS Edit THTriezki_pattikratonMDNo ratings yet
- UHSAA Preparticipation FormDocument4 pagesUHSAA Preparticipation FormThe Salt Lake TribuneNo ratings yet
- Case PresentationDocument18 pagesCase Presentationreem.elkadyNo ratings yet
- The Exercise PrescriptionDocument68 pagesThe Exercise PrescriptionDario MoralesNo ratings yet
- PT1 Revision - Practice QuestionsDocument2 pagesPT1 Revision - Practice Questionsaliza42043No ratings yet