Download as pdf or txt
You might also like
- SN325 Cal Ipr BLRDocument380 pagesSN325 Cal Ipr BLRLic-Carlos MoretaNo ratings yet
- CKE6150 Spare Parts ManualDocument74 pagesCKE6150 Spare Parts ManualVanessa RiveraNo ratings yet
- Schedule of BenefitsDocument7 pagesSchedule of BenefitsMaddy CruzNo ratings yet
- Uhc Aawa24lp0123163 000 H1278028000 SB 21082023 030634 2024 SF20230921Document15 pagesUhc Aawa24lp0123163 000 H1278028000 SB 21082023 030634 2024 SF20230921kevin.mccreaNo ratings yet
- Medical Insurance BenifitsDocument13 pagesMedical Insurance BenifitsdhineshNo ratings yet
- Benefits Guide Colombia 2021Document10 pagesBenefits Guide Colombia 2021Luis Carlos Gutierrez PedrazaNo ratings yet
- Snic - Payless Tob 2021Document6 pagesSnic - Payless Tob 2021DIVYAS11No ratings yet
- Medstar Presentation - Medical Coverage OptionsDocument11 pagesMedstar Presentation - Medical Coverage OptionsSudhakar JayNo ratings yet
- Kick Off Plan Health Pack 2020Document22 pagesKick Off Plan Health Pack 2020Aneesh PrabhakaranNo ratings yet
- KP - Plan Summary Medical - PPODocument3 pagesKP - Plan Summary Medical - PPOshanegbaker51No ratings yet
- Lewermark Health Insurance Copay Plan For Delta State UniversityDocument3 pagesLewermark Health Insurance Copay Plan For Delta State Universityroby sorianoNo ratings yet
- Arogya Sanjeevani PremiumDocument16 pagesArogya Sanjeevani PremiumGiriMahaNo ratings yet
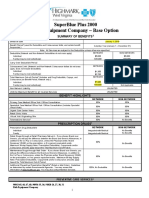
- Rish Equipment Base Plan Option Eff. 1.1.2019Document4 pagesRish Equipment Base Plan Option Eff. 1.1.2019michala anthonyNo ratings yet
- Premier Medic PartnerDocument2 pagesPremier Medic PartnerHihiNo ratings yet
- Individual Medical Policy For Employees - Emed: Table of BenefitsDocument6 pagesIndividual Medical Policy For Employees - Emed: Table of Benefitsrahul sNo ratings yet
- Health Insurance StudyDocument9 pagesHealth Insurance StudyKiran BathiniNo ratings yet
- SGP BWHO 24 Sales Brochure APR18Document5 pagesSGP BWHO 24 Sales Brochure APR18Ms. JenniferNo ratings yet
- USS Pre-Medicare PPO With RX PlanDocument3 pagesUSS Pre-Medicare PPO With RX PlanAnonymous w0egAgMouGNo ratings yet
- BCBS Enrollment GuideDocument6 pagesBCBS Enrollment GuideAnonymous Lri40PrlkNo ratings yet
- DHA Basic Dependents Parents TOB1Document10 pagesDHA Basic Dependents Parents TOB1REGEENANo ratings yet
- Table of Benefits: DHA Plans - Healthcare InsuranceDocument6 pagesTable of Benefits: DHA Plans - Healthcare InsuranceShoeb MohammedNo ratings yet
- 640az Ca NVNBPDocument10 pages640az Ca NVNBPapi-302551405No ratings yet
- CLTC1120Document6 pagesCLTC1120Miguel Angel Escobar ParraNo ratings yet
- Affinity Health Brochure 2024 Combined Plan Life LTD 16.10.2023 12h00Document4 pagesAffinity Health Brochure 2024 Combined Plan Life LTD 16.10.2023 12h00sakondathabisoNo ratings yet
- 2012 Blue Advantage Benefit TableDocument3 pages2012 Blue Advantage Benefit Tableapi-41207808No ratings yet
- Group Health Insurance - Policy Overview.Document14 pagesGroup Health Insurance - Policy Overview.Sai SandeepNo ratings yet
- Group Health Insurance - Policy OverviewDocument16 pagesGroup Health Insurance - Policy OverviewSujithaNo ratings yet
- Fhpv23apr231218j7r2 Veasna UkDocument6 pagesFhpv23apr231218j7r2 Veasna UkSela SinNo ratings yet
- ZoloSure GHI SummaryDocument8 pagesZoloSure GHI SummaryarnavNo ratings yet
- Employee Benefits-Wellness Guide 2023-24Document30 pagesEmployee Benefits-Wellness Guide 2023-24shanzeh2609No ratings yet
- Vanderbilt phf-21-22Document2 pagesVanderbilt phf-21-22api-458468763No ratings yet
- Us Apple Plus Ppo Feb2019 en 1Document3 pagesUs Apple Plus Ppo Feb2019 en 1Lucas Coleta AlmeidaNo ratings yet
- Product Information - DHA Plans Table of BenefitsDocument9 pagesProduct Information - DHA Plans Table of BenefitsMaxedus DotaNo ratings yet
- UnitedHealthcare - Fast, Easy ACA EnrollmentDocument5 pagesUnitedHealthcare - Fast, Easy ACA EnrollmentClaudiu IonNo ratings yet
- 05+Onsurity+Benefit+Summary+for+TopUp PDFDocument4 pages05+Onsurity+Benefit+Summary+for+TopUp PDFYohan BahlNo ratings yet
- SGP BWHO 24 Product Summary APR18Document8 pagesSGP BWHO 24 Product Summary APR18Ms. JenniferNo ratings yet
- Keystone HMO Bronze Essential 750070140700Document11 pagesKeystone HMO Bronze Essential 750070140700ANKIT SINGHNo ratings yet
- Core BronzeDocument4 pagesCore BronzeMohit MarwahNo ratings yet
- Employee Presentation SilverDocument24 pagesEmployee Presentation Silverkishan310No ratings yet
- CC Student 1-Pager 2024Document2 pagesCC Student 1-Pager 2024Cleopas ChigambaNo ratings yet
- MEDICLASSIC Gold One PagerDocument1 pageMEDICLASSIC Gold One Pagerjaluku jinNo ratings yet
- ISO Care Unlimited Student Insurance 2019Document14 pagesISO Care Unlimited Student Insurance 2019Ivory PlatypusNo ratings yet
- Aetna Y0001 H5521 380 PR25 SB24 M 2024 SF20240425Document23 pagesAetna Y0001 H5521 380 PR25 SB24 M 2024 SF20240425kevin.mccreaNo ratings yet
- Benefit Highlights: AARP Medicare Advantage Choice (PPO)Document3 pagesBenefit Highlights: AARP Medicare Advantage Choice (PPO)EstherNo ratings yet
- Aia Platinum Health BrochureDocument8 pagesAia Platinum Health BrochureRaymond AngNo ratings yet
- Diveintopython3 r802Document25 pagesDiveintopython3 r802Ashwin VargheseNo ratings yet
- GMR-Service PPT (2018-19)Document19 pagesGMR-Service PPT (2018-19)Sanjeet GaurNo ratings yet
- Medical Cover Guide-2Document5 pagesMedical Cover Guide-2Temitope AdelowoNo ratings yet
- WWW - Healthcare.gov/sbc-Glossary: Important Questions Answers Why This MattersDocument10 pagesWWW - Healthcare.gov/sbc-Glossary: Important Questions Answers Why This MattersRohitKumarNo ratings yet
- Keystone HMO Gold Preferred 4080650Document11 pagesKeystone HMO Gold Preferred 4080650ANKIT SINGHNo ratings yet
- Tailored Benefit Table - Dragon Oil - Nov23Document4 pagesTailored Benefit Table - Dragon Oil - Nov23David Adrian MuresanNo ratings yet
- MCI One Pager Version 1.0 Oct 2020Document1 pageMCI One Pager Version 1.0 Oct 2020naval730107No ratings yet
- HyBasic Plans Proposal - 2021CDocument3 pagesHyBasic Plans Proposal - 2021CRotimi Shitta-BeyNo ratings yet
- 76962CT0010006-01 en USDocument98 pages76962CT0010006-01 en USKathy ApergisNo ratings yet
- BMI - MediPlan - 250 - R7 - 11 - 1 - 21 - 1 ContratoDocument28 pagesBMI - MediPlan - 250 - R7 - 11 - 1 - 21 - 1 Contratoivantv2014No ratings yet
- Corona Kavach - One Pager - Version 1.0 - July - 2020 PDFDocument1 pageCorona Kavach - One Pager - Version 1.0 - July - 2020 PDFRanjeeta BhanjNo ratings yet
- Corona Kavach STAR One PagerDocument1 pageCorona Kavach STAR One PagerRajat GuptaNo ratings yet
- Schedule of Benefits (Core Silver Without Dental)Document5 pagesSchedule of Benefits (Core Silver Without Dental)Nael SwedanNo ratings yet
- Ne Plan 2 - 150K NextcareDocument6 pagesNe Plan 2 - 150K NextcareatherNo ratings yet
- Oman Basic PlanDocument7 pagesOman Basic Planrahul sNo ratings yet
- GSH Zcard Proof2Document2 pagesGSH Zcard Proof2RyanNo ratings yet
- Diagnostic Imaging of Infections and Inflammatory Diseases: A Multidiscplinary ApproachFrom EverandDiagnostic Imaging of Infections and Inflammatory Diseases: A Multidiscplinary ApproachNo ratings yet
- Scion-tC 2006 EN-US US 20b5ec8cd1Document256 pagesScion-tC 2006 EN-US US 20b5ec8cd1PSC RFQNo ratings yet
- 240 242 HR 06 17Document16 pages240 242 HR 06 17PSC RFQNo ratings yet
- Braco Double Compression Ss Glands SSWDocument1 pageBraco Double Compression Ss Glands SSWPSC RFQNo ratings yet
- All SS (SS 304) Pressure Gauge Bourdon Type: IBR CEDocument5 pagesAll SS (SS 304) Pressure Gauge Bourdon Type: IBR CEPSC RFQNo ratings yet
- 1.EPV NORTH SEA Exploded PartviewDocument45 pages1.EPV NORTH SEA Exploded PartviewPSC RFQNo ratings yet
- Harris N2Document1 pageHarris N2PSC RFQNo ratings yet
- UntitledDocument1 pageUntitledPSC RFQNo ratings yet
- Detcon - FP-524D-LEL - Datasheet 965-525420-100Document2 pagesDetcon - FP-524D-LEL - Datasheet 965-525420-100PSC RFQNo ratings yet
- UntitledDocument1 pageUntitledPSC RFQNo ratings yet
- Demco Valve Ordering GuideDocument8 pagesDemco Valve Ordering GuidePSC RFQNo ratings yet
- H-Drive2 OperationManual v0Document39 pagesH-Drive2 OperationManual v0PSC RFQNo ratings yet
- LatentView Hackathon 22-TNTDocument1 pageLatentView Hackathon 22-TNTPSC RFQNo ratings yet
- EOS00525Document1 pageEOS00525PSC RFQNo ratings yet
- Presentation 6Document2 pagesPresentation 6PSC RFQNo ratings yet
- To-Let: (For Shop) 2 FLOOR: 1200 S.FT Phone: 8179077473Document1 pageTo-Let: (For Shop) 2 FLOOR: 1200 S.FT Phone: 8179077473PSC RFQNo ratings yet
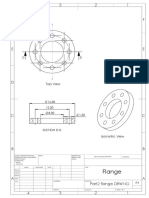
- Part2 Flange DRWNGDocument1 pagePart2 Flange DRWNGPSC RFQNo ratings yet
- Ball Bearing Assembly - Mounica PallaDocument1 pageBall Bearing Assembly - Mounica PallaPSC RFQNo ratings yet
- UntitledDocument3 pagesUntitledPSC RFQNo ratings yet
- Payslip Multi Format 3 NewDocument1 pagePayslip Multi Format 3 NewPSC RFQNo ratings yet
- Sbi ComplaintDocument8 pagesSbi ComplaintPSC RFQNo ratings yet
- Jr. Design Engineer - JDDocument1 pageJr. Design Engineer - JDPSC RFQNo ratings yet
- Bronze-7-Epo-1 1 22-12 31 22Document8 pagesBronze-7-Epo-1 1 22-12 31 22PSC RFQNo ratings yet
- Image 001Document60 pagesImage 001PSC RFQNo ratings yet
- Drawing For Autoclave ThreadsDocument1 pageDrawing For Autoclave ThreadsPSC RFQNo ratings yet
- HR AdvtDocument2 pagesHR AdvtPSC RFQNo ratings yet
- LT Valves Triple Offset Butterfly ValvesDocument20 pagesLT Valves Triple Offset Butterfly ValvesPSC RFQNo ratings yet
- Polar I ScopesDocument6 pagesPolar I Scopessaurabh_acmasNo ratings yet
- A Comparative Study On Selected Fitness Components of 13-19 Years Female Basketball and Volleyball PlayersDocument11 pagesA Comparative Study On Selected Fitness Components of 13-19 Years Female Basketball and Volleyball PlayersAnonymous CwJeBCAXpNo ratings yet
- DT QuizDocument7 pagesDT QuizpadmagurudathNo ratings yet
- 2fy2-01 Engineering Mathematics-I (A To D)Document3 pages2fy2-01 Engineering Mathematics-I (A To D)gwanfldlwjwuwNo ratings yet
- Statistical Softwares: Excel Stata SpssDocument1 pageStatistical Softwares: Excel Stata SpssJeison Manotas ScarpattisNo ratings yet
- LLaVA MEDDocument17 pagesLLaVA MED권오민 / 학생 / 전기·정보공학부No ratings yet
- L&T Process Ball Valves PDFDocument16 pagesL&T Process Ball Valves PDFUnna MalaiNo ratings yet
- A Project Report ON Amul Dairy: Somlalit Institute of Business AdministrationDocument39 pagesA Project Report ON Amul Dairy: Somlalit Institute of Business Administrationprathamesh kaduNo ratings yet
- Conservation Strategies Final DraftDocument61 pagesConservation Strategies Final DraftsebascianNo ratings yet
- Solution Manual Advanced Financial Accounting 8th Edition Baker Chap007 PDFDocument77 pagesSolution Manual Advanced Financial Accounting 8th Edition Baker Chap007 PDFYopie ChandraNo ratings yet
- D1780 - EN - 02 (Signets) GL314F3 - AlstomDocument224 pagesD1780 - EN - 02 (Signets) GL314F3 - Alstomtuantz206No ratings yet
- Datasheet RapASE CarView 092018Document2 pagesDatasheet RapASE CarView 092018Ahmed shabanNo ratings yet
- Hoja Tecnica Control de NivelDocument3 pagesHoja Tecnica Control de NivelpawerxlNo ratings yet
- Trust Bank Account InstructionsDocument5 pagesTrust Bank Account InstructionsGregNo ratings yet
- Dioscorea L. (PROSEA) - PlantUse EnglishDocument29 pagesDioscorea L. (PROSEA) - PlantUse Englishfortuna_dNo ratings yet
- Mechanisms of NSAID-Induced HepatotoxicityDocument16 pagesMechanisms of NSAID-Induced HepatotoxicityRonald WiradirnataNo ratings yet
- BRM Lecture4Document12 pagesBRM Lecture4amrj27609No ratings yet
- Bla BlaDocument8 pagesBla BladharwinNo ratings yet
- Brochure HCCDocument13 pagesBrochure HCCManu MohanNo ratings yet
- Acceptability of Banana Cheese Balls For Students in Colegio de Los BanosDocument4 pagesAcceptability of Banana Cheese Balls For Students in Colegio de Los BanosBSED SOCSTUD I-C Manese,JeremyNo ratings yet
- DLL-first-quarter Sci10Document4 pagesDLL-first-quarter Sci10Danilo Balbas, Jr.100% (1)
- Shelf-Life and Storage Requirement BS (Updated)Document1 pageShelf-Life and Storage Requirement BS (Updated)Jason Tiongco0% (1)
- Immobi Ad SpecsDocument32 pagesImmobi Ad SpecsManuj KhuranaNo ratings yet
- Trading PlanDocument12 pagesTrading Planpeterhash5No ratings yet
- GCSE Literature SyllabusDocument29 pagesGCSE Literature SyllabusJooby77No ratings yet
- Information Requirement AnalysisDocument3 pagesInformation Requirement Analysis5ladyNo ratings yet
- Lab Assignment 1 (TempRTD) 1Document6 pagesLab Assignment 1 (TempRTD) 1MuTaYaM_EmArAtINo ratings yet
- Demand For Documents, Citing ContemptDocument53 pagesDemand For Documents, Citing ContemptJoel Banner BairdNo ratings yet