Download as docx, pdf, or txt
You might also like
- Executive Order - BadacDocument5 pagesExecutive Order - BadacChristopher Torres100% (16)
- Psychiatric Mental Health Nurse Practitioner Job Description SampleDocument3 pagesPsychiatric Mental Health Nurse Practitioner Job Description Sampleapi-291172309No ratings yet
- Topic 4: Addiction Screening and Assessment Tools ChartDocument7 pagesTopic 4: Addiction Screening and Assessment Tools ChartAmelia KruegerNo ratings yet
- Psychiatric Mental Health Comprehensive Case StudyDocument14 pagesPsychiatric Mental Health Comprehensive Case Studyapi-546967314No ratings yet
- PC Resource GuideDocument4 pagesPC Resource GuideHannah MurrayNo ratings yet
- Psychiatric Mental Health Comprehensive Case StudyDocument14 pagesPsychiatric Mental Health Comprehensive Case Studyapi-739571998No ratings yet
- Case Study Mental Health KrsDocument14 pagesCase Study Mental Health Krsapi-657570532No ratings yet
- Mental HealthDocument13 pagesMental Healthapi-719825532No ratings yet
- MH Case StudyDocument12 pagesMH Case Studyapi-741800384No ratings yet
- Mental Health Case Study Spring 2024Document15 pagesMental Health Case Study Spring 2024api-740642728No ratings yet
- Case Study Final DraftDocument15 pagesCase Study Final Draftapi-608049224No ratings yet
- Psych Case StudyDocument13 pagesPsych Case Studyapi-736869233No ratings yet
- Psychiatric Mental Health Comprehensive Case StudyDocument14 pagesPsychiatric Mental Health Comprehensive Case Studyapi-662323379100% (1)
- Case Study Mental HealthDocument13 pagesCase Study Mental Healthapi-738695053No ratings yet
- Case StudyDocument16 pagesCase Studyapi-740431489No ratings yet
- MH Case StudyDocument13 pagesMH Case Studyapi-741959745No ratings yet
- Psychiatric Mental Health Comprehensive Case StudyDocument12 pagesPsychiatric Mental Health Comprehensive Case Studyapi-662890978No ratings yet
- Case Study Samantha Ditosti CompleteDocument13 pagesCase Study Samantha Ditosti Completeapi-662164351No ratings yet
- Mental Health Case Study CompletedDocument13 pagesMental Health Case Study Completedapi-730811728No ratings yet
- Case Study 2Document11 pagesCase Study 2api-663126174No ratings yet
- Mental Health Case StudyDocument12 pagesMental Health Case Studyapi-507993112No ratings yet
- Case Study - Izabella WertzDocument11 pagesCase Study - Izabella Wertzapi-663559916No ratings yet
- MH Case Study 1Document13 pagesMH Case Study 1api-601489653No ratings yet
- 10 Page Paper For Mental Health Sophia DelatoreDocument11 pages10 Page Paper For Mental Health Sophia Delatoreapi-663410827No ratings yet
- Case Study Caitlyn HoweDocument11 pagesCase Study Caitlyn Howeapi-738778945No ratings yet
- Case StudyDocument12 pagesCase Studyapi-663728377No ratings yet
- Psychiatric Mental Health Comprehensive Case StudyDocument13 pagesPsychiatric Mental Health Comprehensive Case Studyapi-604569933No ratings yet
- Psychiatric Mental Health Comprehensive Case StudyDocument13 pagesPsychiatric Mental Health Comprehensive Case Studyapi-736973985No ratings yet
- Pysch Case StudyDocument12 pagesPysch Case Studyapi-597683251No ratings yet
- Case StudyDocument12 pagesCase Studyapi-662613408No ratings yet
- Mental Health Clinical Case Study - Andreanna TocickiDocument13 pagesMental Health Clinical Case Study - Andreanna Tocickiapi-741174198No ratings yet
- Mental Health Case StudyDocument15 pagesMental Health Case Studyapi-663643642No ratings yet
- Case StudyDocument13 pagesCase Studyapi-663834833No ratings yet
- Case StudyDocument12 pagesCase Studyapi-731527860No ratings yet
- Running Head: Mental Health Comprehensive Case Study 1Document9 pagesRunning Head: Mental Health Comprehensive Case Study 1api-741216417No ratings yet
- Psychiatric Mental Health Comprehensive Case StudyDocument12 pagesPsychiatric Mental Health Comprehensive Case Studyapi-741551545No ratings yet
- MHC - Case StudyDocument15 pagesMHC - Case Studyapi-546488467No ratings yet
- Clincial Paper - PsychDocument12 pagesClincial Paper - Psychapi-651130562100% (1)
- Case StudyDocument14 pagesCase Studyapi-663318600No ratings yet
- Case StudyDocument12 pagesCase Studyapi-739129968No ratings yet
- MH Case StudyDocument14 pagesMH Case Studyapi-719766335No ratings yet
- Case Study PsychDocument12 pagesCase Study Psychapi-662489107No ratings yet
- Case StudyDocument14 pagesCase Studyapi-661467979No ratings yet
- Psych Case StudyDocument12 pagesPsych Case Studyapi-663631864No ratings yet
- Comprehensive Case Study MH - SantucciDocument15 pagesComprehensive Case Study MH - Santucciapi-663034532No ratings yet
- Psych Case StudyDocument11 pagesPsych Case Studyapi-663879907No ratings yet
- MH Case Study - Whiley DrymonDocument13 pagesMH Case Study - Whiley Drymonapi-664257988No ratings yet
- Apa Paper For Mental HealthDocument13 pagesApa Paper For Mental Healthapi-648586622No ratings yet
- Mental Health Comprehensive Case StudyDocument16 pagesMental Health Comprehensive Case Studyapi-741272284No ratings yet
- Mental Health Case StudyDocument14 pagesMental Health Case Studyapi-736949349No ratings yet
- Case Study MH FinalDocument13 pagesCase Study MH Finalapi-724442716No ratings yet
- Case StudyDocument17 pagesCase Studyapi-508597583No ratings yet
- MH Case Study 2Document12 pagesMH Case Study 2api-652166364No ratings yet
- Mental HealthDocument12 pagesMental Healthapi-662585161No ratings yet
- Mental Health Case Study Paper 2022Document13 pagesMental Health Case Study Paper 2022api-663434713No ratings yet
- Case Study Mental HealthDocument12 pagesCase Study Mental Healthapi-603895785No ratings yet
- Case Study - Steven LukacDocument13 pagesCase Study - Steven Lukacapi-508092399No ratings yet
- Meadows Paige Case StudyDocument16 pagesMeadows Paige Case Studyapi-607727110No ratings yet
- Mental Health Case Study 4Document17 pagesMental Health Case Study 4api-653306608No ratings yet
- Psychiatric Mental Health Comprehensive Case StudyDocument11 pagesPsychiatric Mental Health Comprehensive Case Studyapi-591372252No ratings yet
- Psych Case StudyDocument15 pagesPsych Case Studyapi-659158323No ratings yet
- 10 Page MH Comprehensive Case StudyDocument13 pages10 Page MH Comprehensive Case Studyapi-663783246No ratings yet
- Psychiatric Mental Health Comprehensive Case StudyDocument13 pagesPsychiatric Mental Health Comprehensive Case Studyapi-663135887No ratings yet
- Well Fest TopicDocument6 pagesWell Fest Topicapi-660321588No ratings yet
- Shoebox PresentationDocument28 pagesShoebox Presentationapi-660321588No ratings yet
- Clinical Nursing Judgment Senior Capstone - Emerson Fletcher - FinalDocument6 pagesClinical Nursing Judgment Senior Capstone - Emerson Fletcher - Finalapi-660321588No ratings yet
- Research Paper - FinalDocument14 pagesResearch Paper - Finalapi-660321588No ratings yet
- Peds Concept Map - FinalDocument6 pagesPeds Concept Map - Finalapi-660321588No ratings yet
- Resume - School - FinalDocument1 pageResume - School - Finalapi-660321588No ratings yet
- Reviewer in NSTPDocument13 pagesReviewer in NSTPAundrei ValdezNo ratings yet
- The American Psychiatric Association Publishing Textbook of Substance Use Disorder Treatment, Sixth Edition Kathleen T. BradyDocument70 pagesThe American Psychiatric Association Publishing Textbook of Substance Use Disorder Treatment, Sixth Edition Kathleen T. Bradybernardmccormack491148100% (5)
- Ebook Direct Social Work Practice Theory and Skills PDF Full Chapter PDFDocument67 pagesEbook Direct Social Work Practice Theory and Skills PDF Full Chapter PDFbrant.coots685100% (37)
- Chapter 13 Dispensing of Controlled SubstancesDocument12 pagesChapter 13 Dispensing of Controlled SubstancesMuhammad Kasi100% (4)
- Submitted To Submitted By: Subject: Community Health Nursing-IiDocument3 pagesSubmitted To Submitted By: Subject: Community Health Nursing-IiMahi RaperiaNo ratings yet
- Mental Health InterviewDocument5 pagesMental Health Interviewapi-571933034No ratings yet
- Teenage Drug Abuse Thesis StatementDocument4 pagesTeenage Drug Abuse Thesis Statementkatieboothwilmington100% (2)
- Top 10 Public Health Challenges To Track in 2023Document8 pagesTop 10 Public Health Challenges To Track in 2023Anne LauretaNo ratings yet
- Adlerian Case FormulationDocument24 pagesAdlerian Case FormulationJellie Mae LazaroNo ratings yet
- EAPP Quarter 1 - Module - 5.pdf Version 1Document10 pagesEAPP Quarter 1 - Module - 5.pdf Version 1edina mendozaNo ratings yet
- Maryland Marijuana Legalization Bill and SummaryDocument61 pagesMaryland Marijuana Legalization Bill and SummaryMarijuana MomentNo ratings yet
- Civic Education Grade 10 ... 1 PDFDocument41 pagesCivic Education Grade 10 ... 1 PDFKathryn Chongwe100% (1)
- Argumentative Essay MhykeDocument2 pagesArgumentative Essay MhykeAnne MarielNo ratings yet
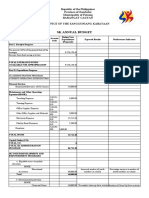
- SK Annual Budget 1 1Document2 pagesSK Annual Budget 1 1KENNETH ANINZO100% (1)
- Bermuda Drug Information Network: (Berdin)Document150 pagesBermuda Drug Information Network: (Berdin)BernewsAdminNo ratings yet
- Psychiatry: MedpgnotesDocument54 pagesPsychiatry: MedpgnotesShanmugam BalasubramaniamNo ratings yet
- Building Recovery Capital: Addiction, Recovery, and Recovery Support Services Among Young AdultsDocument105 pagesBuilding Recovery Capital: Addiction, Recovery, and Recovery Support Services Among Young AdultsThe Stacie Mathewson FoundationNo ratings yet
- Substance Abuse, Drugs and Addictions: GuidebookDocument114 pagesSubstance Abuse, Drugs and Addictions: GuidebookPugh Jutta67% (3)
- Research Chapter 1Document17 pagesResearch Chapter 1Jenek100% (2)
- Biology New Article ResearchDocument5 pagesBiology New Article ResearchDaph H.No ratings yet
- Codependency Treatment Systematic Review 2015Document12 pagesCodependency Treatment Systematic Review 2015Ryan PetersonNo ratings yet
- Types of Child AbuseDocument17 pagesTypes of Child AbuseSiva NeshNo ratings yet
- Surgeon General's Workshop On Women's Mental HealthDocument93 pagesSurgeon General's Workshop On Women's Mental HealthHollie1230100% (3)
- Parental Substance AbuseDocument10 pagesParental Substance Abuseapi-360330020No ratings yet
- BibliographyDocument7 pagesBibliographyMargarita Limon BalunesNo ratings yet