Download as pdf or txt
You might also like
- Electrical Quality Control Plan SampleDocument25 pagesElectrical Quality Control Plan Sampleshah1980100% (1)
- National Blood Bank Network System (Nbbnets) Registration Form Blood Service Facility DataDocument4 pagesNational Blood Bank Network System (Nbbnets) Registration Form Blood Service Facility DataKathrine Ann Favorito100% (2)
- Individual EPPM4014Document15 pagesIndividual EPPM4014Yu XinleiNo ratings yet
- Nbs Purchase OrderDocument1 pageNbs Purchase Ordercatherine joy macalos0% (1)
- Work Comp C4Document5 pagesWork Comp C4ijustwanawriteNo ratings yet
- Water PT Reg FormDocument1 pageWater PT Reg Formblancomateresa642No ratings yet
- 2018 11 30 Calibration Application FormDocument2 pages2018 11 30 Calibration Application FormHaikalNo ratings yet
- 2020 NEQAS CC Registration Form and Order of PaymentDocument2 pages2020 NEQAS CC Registration Form and Order of PaymentNovie FeneciosNo ratings yet
- Date Customer Application Form InstitutionsDocument5 pagesDate Customer Application Form InstitutionsAnaliza Kitongan LantayanNo ratings yet
- Pi CSXL2023112301Document1 pagePi CSXL2023112301Dave BunquinNo ratings yet
- Please Choose One and CheckDocument2 pagesPlease Choose One and CheckcyrhenmieNo ratings yet
- Hospital Bill 1Document2 pagesHospital Bill 1Süññy MäñèNo ratings yet
- 1SDTL Water Analysis Training Davao June 2018 Invitation PDFDocument3 pages1SDTL Water Analysis Training Davao June 2018 Invitation PDFCo-chon ChoNo ratings yet
- NTP Referral FormDocument2 pagesNTP Referral FormCarl RamosNo ratings yet
- Testing Application Form:: Contact Person:: Contact No.Document2 pagesTesting Application Form:: Contact Person:: Contact No.Roy SNo ratings yet
- Malaysian Standard (MS) Order Form: Yes No Cash Credit/Debit Card Eft Cash Deposit Cheque Purchase OrderDocument1 pageMalaysian Standard (MS) Order Form: Yes No Cash Credit/Debit Card Eft Cash Deposit Cheque Purchase OrderLaila MajnunNo ratings yet
- SDTL & Water Analysis Training-Davao - Rev2Document3 pagesSDTL & Water Analysis Training-Davao - Rev2HSQMRAD MPINo ratings yet
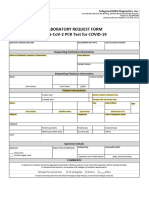
- Laboratory Request Form - SDDI SEED PASAYDocument2 pagesLaboratory Request Form - SDDI SEED PASAY899vm2gszjNo ratings yet
- Modelo Proforma Invoice PIDocument1 pageModelo Proforma Invoice PIferdinand jhnatanNo ratings yet
- Rabies Serology Certificate 22dec23Document13 pagesRabies Serology Certificate 22dec23hendra utamaNo ratings yet
- Bupa Global Reimbursement FormDocument5 pagesBupa Global Reimbursement Formshena0% (1)
- 1564948120Document1 page1564948120Lonmar L. Lentch LopezNo ratings yet
- Lab ReportDocument1 pageLab Reportnishitagupta750No ratings yet
- Form 7 v050120Document2 pagesForm 7 v050120Northern Benguet District-hNo ratings yet
- Microbiology Test Request FormDocument4 pagesMicrobiology Test Request FormMegen PLCNo ratings yet
- TSAFDocument2 pagesTSAFrhizza basilioNo ratings yet
- Calibration Service Request Form: CLL Corporate Office and Central LaboratoryDocument3 pagesCalibration Service Request Form: CLL Corporate Office and Central LaboratoryReama QumsanNo ratings yet
- Registration Form: Reganion, Criselda Charisse TanDocument1 pageRegistration Form: Reganion, Criselda Charisse TanceeNo ratings yet
- ReferralDocument3 pagesReferralResh Aiken khoNo ratings yet
- Unit Trust Account Opening Form 13.12.2019 1Document4 pagesUnit Trust Account Opening Form 13.12.2019 1henrykibe01No ratings yet
- Distriphil Cif FormDocument3 pagesDistriphil Cif Formjimabil ramirezNo ratings yet
- Standard Diagnostic Bill 1Document2 pagesStandard Diagnostic Bill 1Süññy MäñèNo ratings yet
- All Transactions - Registration of Aircraft On The South African Civil Aircraft Register (Sacar) - CA 61-91Document2 pagesAll Transactions - Registration of Aircraft On The South African Civil Aircraft Register (Sacar) - CA 61-91Jack ArcherNo ratings yet
- Form Berlangganan QuantumDocument2 pagesForm Berlangganan Quantumvitri darleneNo ratings yet
- Pacific Corp: Application FormDocument1 pagePacific Corp: Application FormErwin ArcilaNo ratings yet
- Form 7 v050120Document2 pagesForm 7 v050120nursing sectionNo ratings yet
- Paramount Health Services & Insurance Tpa Private Limited: Deficiency Letter Without PrejudiceDocument2 pagesParamount Health Services & Insurance Tpa Private Limited: Deficiency Letter Without PrejudiceHemantNo ratings yet
- Request For Refund or Test Date Transfer Form 29 Julv2Document2 pagesRequest For Refund or Test Date Transfer Form 29 Julv2Azril AzmiNo ratings yet
- Dotpay Merchant Application FormDocument3 pagesDotpay Merchant Application FormBayudamai ArielNo ratings yet
- NEQAS Registration Form 2020-SerologyDocument2 pagesNEQAS Registration Form 2020-SerologyMark Jefferson Sanchez Merto100% (5)
- Implant FormDocument2 pagesImplant FormAstha TimothyNo ratings yet
- Patient Uc Authorization FormDocument2 pagesPatient Uc Authorization FormTimothy PostulkaNo ratings yet
- C 4amrDocument2 pagesC 4amrGreen TinaNo ratings yet
- PT6311Document1 pagePT6311soaresNo ratings yet
- Ilovepdf MergedDocument8 pagesIlovepdf MergedRaju BhuyanNo ratings yet
- JR PI For Flame DetectorDocument1 pageJR PI For Flame Detectormohammed ayedNo ratings yet
- Registration Form: Tugaoen, Sam Denielle SalvacionDocument1 pageRegistration Form: Tugaoen, Sam Denielle SalvacionSam Denielle TugaoenNo ratings yet
- Power Tools Plus Account Application V3Document2 pagesPower Tools Plus Account Application V3alvin.alsruralcontractingNo ratings yet
- USTFMS ERB F01 Application FormDocument2 pagesUSTFMS ERB F01 Application FormJeriz Marie GamboaNo ratings yet
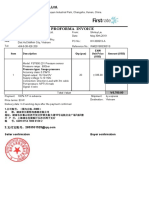
- 2019.5.30 PI From Firstrate Sensor, Shirley PDFDocument1 page2019.5.30 PI From Firstrate Sensor, Shirley PDFBuiDucVinhNo ratings yet
- Clinical Registration FormDocument2 pagesClinical Registration Formabbas jadoonNo ratings yet
- Read Before RegisteringDocument3 pagesRead Before RegisteringkanagarajodishaNo ratings yet
- Western Leyte College of Ormoc City, Inc.: Official ReceiptDocument2 pagesWestern Leyte College of Ormoc City, Inc.: Official ReceiptKyeienNo ratings yet
- TN Enrollment Document For 87726 Created 6-12-2023 37731414Document2 pagesTN Enrollment Document For 87726 Created 6-12-2023 37731414kalinalveyNo ratings yet
- Christian Medical CollegeDocument1 pageChristian Medical CollegeJhumon DharNo ratings yet
- 2019 Registration FormDocument3 pages2019 Registration FormJoanne Jaramilla Dollente33% (3)
- OCA - 115c - Initial Application (Processing & Trading) - 181119Document4 pagesOCA - 115c - Initial Application (Processing & Trading) - 181119jamil voraNo ratings yet
- Eqas 2019 Form - NewDocument2 pagesEqas 2019 Form - NewAlfreah Jean Tambasen100% (3)
- EQAS 2019 Form - New PDFDocument2 pagesEQAS 2019 Form - New PDFSharon ChuaNo ratings yet
- PT Aa International Indonesia: Panel Provider Application FormDocument3 pagesPT Aa International Indonesia: Panel Provider Application Formrinova intanNo ratings yet
- cpcsp-01 2009Document1 pagecpcsp-01 2009mentecuerpoNo ratings yet
- DtlStatement 08082022055359Document17 pagesDtlStatement 08082022055359Aralt visaNo ratings yet
- Definitions,: UNIT - I: Energy Audit PrinciplesDocument2 pagesDefinitions,: UNIT - I: Energy Audit PrinciplesNmg KumarNo ratings yet
- PDF 89369899 Wiring Diagram FM PDF CompressDocument100 pagesPDF 89369899 Wiring Diagram FM PDF CompressCristhian Monge RojasNo ratings yet
- Thesis of Major Project Alpha Stirling Engine-1Document32 pagesThesis of Major Project Alpha Stirling Engine-1SakshiNo ratings yet
- Eem Challenge Change ControlDocument1 pageEem Challenge Change ControlPA2 ksplNo ratings yet
- Eva-200 201 210 Ome 070515Document36 pagesEva-200 201 210 Ome 070515Hikmat RahimovNo ratings yet
- SAP Interview QuestionsDocument4 pagesSAP Interview QuestionsmohammedtahmedNo ratings yet
- BSC in CS For Cohorts 2019-2020Document23 pagesBSC in CS For Cohorts 2019-2020Ashraf Al hinaiNo ratings yet
- Gdam Namria PagenetDocument20 pagesGdam Namria Pagenetalchemer05No ratings yet
- Audio CircuitDocument4 pagesAudio CircuitTanya PiriyabunharnNo ratings yet
- Change Management Process For IT ServicesDocument8 pagesChange Management Process For IT ServicesEddy ManurungNo ratings yet
- Spare Parts Catalogue Reservdelskatalog: Doc. No. EDITION 2.2011Document114 pagesSpare Parts Catalogue Reservdelskatalog: Doc. No. EDITION 2.2011kocak gaming mantap kaliNo ratings yet
- OpTransactionHistory19 11 2019Document14 pagesOpTransactionHistory19 11 2019maheshNo ratings yet
- IBS301m - International Business Strategy - Session 24 - 26Document17 pagesIBS301m - International Business Strategy - Session 24 - 26Nguyen Trung Hau K14 FUG CTNo ratings yet
- Command For Underground Electrical System: Conn 10 Conn 11 CONN 12,13,17 6 5 CONN 18,19 Conn 16Document2 pagesCommand For Underground Electrical System: Conn 10 Conn 11 CONN 12,13,17 6 5 CONN 18,19 Conn 16Antonio Saraguro SotoNo ratings yet
- Calibration Eraser-C-EnDocument14 pagesCalibration Eraser-C-Enapi-538691317No ratings yet
- Prospekt RSNC enDocument6 pagesProspekt RSNC encroplaninecNo ratings yet
- Saina Nehwal: Personal LifeDocument9 pagesSaina Nehwal: Personal LifeMradul GuptaNo ratings yet
- 10-3 Installing Software AG ProductsDocument79 pages10-3 Installing Software AG Productsram GehlotNo ratings yet
- Toyota - Linear Valve Learn Value InitializationDocument4 pagesToyota - Linear Valve Learn Value InitializationGerald Louie Uy MeguizoNo ratings yet
- Responsibilities of A Test Manager and Test Lead (Shared Both)Document3 pagesResponsibilities of A Test Manager and Test Lead (Shared Both)Dat Van TienNo ratings yet
- Form No.2Document4 pagesForm No.2sibasish patelNo ratings yet
- 5G and Its Economic Aspects Literature Review and Selection of A Connection Portfolio Under RiskDocument164 pages5G and Its Economic Aspects Literature Review and Selection of A Connection Portfolio Under RiskĐức TrungNo ratings yet
- ASM2 AdvancedProgramming PDFDocument26 pagesASM2 AdvancedProgramming PDFKhanh QNo ratings yet
- PHD Thesis Business Process ManagementDocument5 pagesPHD Thesis Business Process Managementjpcbobkef100% (2)
- Module 2 CSS G11 1st Semweek 3-4Document44 pagesModule 2 CSS G11 1st Semweek 3-4Clark Domingo100% (1)
- ISSE 2023 - Deck 190523Document33 pagesISSE 2023 - Deck 190523Steven AdrianusNo ratings yet
- FMP Getting Started Guide - v5Document13 pagesFMP Getting Started Guide - v5shahidNo ratings yet