Download as pdf or txt
You might also like
- Ao2019 0026Document5 pagesAo2019 0026alissalvqs100% (2)
- M Test (Meridian Test) MukainoDocument11 pagesM Test (Meridian Test) MukainoVicente Acosta100% (1)
- Domiciliary Midwifery RDocument16 pagesDomiciliary Midwifery Rswillymadhu86% (7)
- Midwifery ScopeDocument4 pagesMidwifery Scopedfgdfjggkh100% (2)
- Midwife MeansDocument17 pagesMidwife Meansvarshasharma05100% (1)
- Soal Inggris PoltekkesDocument6 pagesSoal Inggris PoltekkesDheby Anggara100% (1)
- Professional AdjustmentDocument200 pagesProfessional AdjustmentElchastellie Castañeda67% (3)
- Holy Cross College: Sta. Ana, PampangaDocument35 pagesHoly Cross College: Sta. Ana, PampangaWinter Kyle Reyes DizonNo ratings yet
- Pregnancy and Childcare: Topic 4Document59 pagesPregnancy and Childcare: Topic 4iAmSoluna Exo-LNo ratings yet
- ROLE OF NURSE 3Document8 pagesROLE OF NURSE 3Ranjita GaudNo ratings yet
- Ao2019 0026 PDFDocument5 pagesAo2019 0026 PDFSAMUEL AUSTRIANo ratings yet
- C-Obs 41 Standards in Maternity Care Review Mar 12Document40 pagesC-Obs 41 Standards in Maternity Care Review Mar 12Ywagar YwagarNo ratings yet
- Ncma217 TransDocument34 pagesNcma217 Transpat delapenaNo ratings yet
- Postnatal - Care On Admission To The Ward PDFDocument3 pagesPostnatal - Care On Admission To The Ward PDFHellenKyakuwaireNo ratings yet
- .O ....... OU :2l2 - : Office of The SecretaryDocument7 pages.O ....... OU :2l2 - : Office of The SecretarysabrinajavellanaNo ratings yet
- Lapsus ISKDocument67 pagesLapsus ISKvioletgrayflameNo ratings yet
- Modified SOP of MidwivesDocument10 pagesModified SOP of MidwivesEmmanuel JNo ratings yet
- Role of Midwifery PracticeDocument17 pagesRole of Midwifery PracticeTania ThomasNo ratings yet
- Intrapartum CareDocument65 pagesIntrapartum Caremarkus_danusantosoNo ratings yet
- RCOG - Parto NormalDocument65 pagesRCOG - Parto Normaliker santiago castilloNo ratings yet
- Ncma 217a Lec Prelims Care of Mother Child Adolescent Well ClientDocument68 pagesNcma 217a Lec Prelims Care of Mother Child Adolescent Well ClientVanessa CabanlitNo ratings yet
- Intrapartum Care Intrapartum Care OverviewDocument11 pagesIntrapartum Care Intrapartum Care OverviewVrunda AppannagariNo ratings yet
- History of Present IllnessDocument30 pagesHistory of Present IllnessTrixia Joy R NachorNo ratings yet
- 5. Nursing Care in PregnancyDocument52 pages5. Nursing Care in Pregnancykuruvagadda sagarNo ratings yet
- Bemonc WordDocument10 pagesBemonc Wordmarkyabres100% (1)
- BPH313Family and Reproductive Health Group 9 Presentation, SID 027-491Document17 pagesBPH313Family and Reproductive Health Group 9 Presentation, SID 027-491duku mosesNo ratings yet
- Obg Unit IDocument19 pagesObg Unit IJeyachithra100% (3)
- Antenatal CareDocument3 pagesAntenatal CaremuleyazegetNo ratings yet
- WEEK 1 PharmaDocument5 pagesWEEK 1 PharmaKrystel Anne MilanNo ratings yet
- Circ22 2014 PDFDocument20 pagesCirc22 2014 PDFErnest Jerome MalamionNo ratings yet
- Maternal CareDocument13 pagesMaternal CareHannan AliNo ratings yet
- The Simplest Definition of MidwiferyDocument2 pagesThe Simplest Definition of MidwiferyRystaaRudiniNo ratings yet
- Role of CHN IN MCHDocument43 pagesRole of CHN IN MCHkrupa mathewNo ratings yet
- Lesson 5 - Pregnancy and Prenatal CareDocument24 pagesLesson 5 - Pregnancy and Prenatal CareAPRIL ALAPNo ratings yet
- Sexual, Reproductive and Maternal Health Services During COVID 19Document18 pagesSexual, Reproductive and Maternal Health Services During COVID 19khan7venNo ratings yet
- DOH Maternal Health ProgramDocument6 pagesDOH Maternal Health ProgramJinky TenezaNo ratings yet
- Coronavirus (COVID-19) Infection and Abortion CareDocument27 pagesCoronavirus (COVID-19) Infection and Abortion CareShaliniMargamNo ratings yet
- Assignment 2Document4 pagesAssignment 2chindobr8No ratings yet
- 1 2020-03-30-Guidance-For-Antenatal-And-Postnatal-Services-In-The-Evolving-Coronavirus-Covid-19-Pandemic-20200331Document13 pages1 2020-03-30-Guidance-For-Antenatal-And-Postnatal-Services-In-The-Evolving-Coronavirus-Covid-19-Pandemic-20200331Nuril IMSACNo ratings yet
- DOH Maternal Health ProgramDocument5 pagesDOH Maternal Health ProgramErwin Jake TagubaNo ratings yet
- Seminar On Preventive ObstetricsDocument49 pagesSeminar On Preventive ObstetricsRini Robert100% (3)
- Case and Guide QuestionsDocument5 pagesCase and Guide QuestionsKenneth NovenoNo ratings yet
- EMONCDocument17 pagesEMONCJessie OranoNo ratings yet
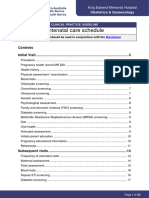
- Antenatal Care ScheduleKEM Hosp AUSTRAliaDocument20 pagesAntenatal Care ScheduleKEM Hosp AUSTRAliamill86No ratings yet
- Post - Abortion - Family - Planning IndiaDocument34 pagesPost - Abortion - Family - Planning Indiageorgeloto12No ratings yet
- Unit-2 Antenatal AssessmentDocument16 pagesUnit-2 Antenatal AssessmentAnil Patel100% (5)
- ROLES RESPONSIBILITIES OF A MC NURSE IN CHALENGEING SITUATIONS Merged Compressed Merged MergedDocument53 pagesROLES RESPONSIBILITIES OF A MC NURSE IN CHALENGEING SITUATIONS Merged Compressed Merged MergedYuuki Chitose (tai-kun)No ratings yet
- Reproductive HealthDocument87 pagesReproductive Healthayushmanc67No ratings yet
- Health TeachingDocument27 pagesHealth TeachingDaniel LaoatenNo ratings yet
- Maternal and Child Health Programmes AssignmentDocument11 pagesMaternal and Child Health Programmes Assignmentannu panchal80% (5)
- CMO No.33 s2007Document92 pagesCMO No.33 s2007queenfaustineeNo ratings yet
- All Qustions by Tuqa Jumaah2022Document67 pagesAll Qustions by Tuqa Jumaah2022Yanique BarrettNo ratings yet
- Women Who Have Concealed Their Pregnancy or Who Are Presenting For Ante Natal Care or To Give Birth That Are Booked To Receive Care ElsewhereDocument6 pagesWomen Who Have Concealed Their Pregnancy or Who Are Presenting For Ante Natal Care or To Give Birth That Are Booked To Receive Care Elsewheresliding_doorsNo ratings yet
- Chickenpox in Pregnancy Final September 2020 291021Document6 pagesChickenpox in Pregnancy Final September 2020 291021Dk YadavNo ratings yet
- AbortionDocument77 pagesAbortionfahadqazifreelancerNo ratings yet
- Maternity QuestionsDocument49 pagesMaternity Questionsdeb100% (17)
- NCM 107 Intro 1Document34 pagesNCM 107 Intro 1Riegne Chiara Fay AcuzarNo ratings yet
- Unit 1 - Introduction To MidwiferyDocument25 pagesUnit 1 - Introduction To Midwiferypriya100% (1)
- MDWF 2010 Carter Informed Disclosure For Midwifery CareDocument6 pagesMDWF 2010 Carter Informed Disclosure For Midwifery Careapi-366292665No ratings yet
- Inevitable AbortionDocument21 pagesInevitable AbortionJaysonPangilinanAbanNo ratings yet
- The Prospective Mother, a Handbook for Women During PregnancyFrom EverandThe Prospective Mother, a Handbook for Women During PregnancyNo ratings yet
- Perinatal Care Manual 4 EditionDocument457 pagesPerinatal Care Manual 4 EditionWei XinNo ratings yet
- ROZEMA Psychosocial Issues and Asthma ManagementDocument23 pagesROZEMA Psychosocial Issues and Asthma ManagementWei XinNo ratings yet
- NSG 222 SDSDocument4 pagesNSG 222 SDSWei XinNo ratings yet
- Comppgm 4Document27 pagesComppgm 4Wei XinNo ratings yet
- 2806 SMJ 10Document6 pages2806 SMJ 10Wei XinNo ratings yet
- Obstetric Flying SquadDocument3 pagesObstetric Flying SquadWei XinNo ratings yet
- 61 MainText 1125 1 10 20180712Document5 pages61 MainText 1125 1 10 20180712Wei XinNo ratings yet
- Yiruma - Room With A View (2021 Update)Document5 pagesYiruma - Room With A View (2021 Update)Wei XinNo ratings yet
- Kellgren and Lawrence Grading For Osteoartritis RadiographsDocument6 pagesKellgren and Lawrence Grading For Osteoartritis Radiographsnitu73100% (1)
- Ob AssessmentDocument7 pagesOb AssessmentAlyssa LippNo ratings yet
- Stress Among Charge NursesDocument10 pagesStress Among Charge NursesRey AllanNo ratings yet
- Emmanuel'S Resort: Samay, BalingasagDocument4 pagesEmmanuel'S Resort: Samay, BalingasagBryan LluismaNo ratings yet
- IntroductionDocument5 pagesIntroductionPaul OrbinoNo ratings yet
- Richard Legaspi Crohn's DiseaseDocument12 pagesRichard Legaspi Crohn's DiseaseRichard RLNo ratings yet
- Public Perception of Mental Health in Iraq: Research Open AccessDocument11 pagesPublic Perception of Mental Health in Iraq: Research Open AccessSri HariNo ratings yet
- Dr. Michael Tarver Emergency Suspension ComplaintDocument10 pagesDr. Michael Tarver Emergency Suspension ComplaintDentist The MenaceNo ratings yet
- Peripheral NeuropathyDocument30 pagesPeripheral NeuropathyLyn LynNo ratings yet
- Gen Z and Mental Health in The US - February 2022 ReportDocument26 pagesGen Z and Mental Health in The US - February 2022 ReportT VyNo ratings yet
- W9 Teori Akuntansi RS ASPDocument4 pagesW9 Teori Akuntansi RS ASPJessicaNo ratings yet
- Role of Nurses in Clinical ResearchDocument20 pagesRole of Nurses in Clinical ResearchOhoud ElsheikhNo ratings yet
- The Analysis of Pharmaceutical MarketDocument10 pagesThe Analysis of Pharmaceutical MarketAnamaria BejenariuNo ratings yet
- Xceed 1 Slide Per PageDocument31 pagesXceed 1 Slide Per Pagemccarthy121677100% (1)
- MBT and TraumaDocument19 pagesMBT and Traumassanagav0% (1)
- Management of Patients Receiving Local Anaesthesia 2021Document76 pagesManagement of Patients Receiving Local Anaesthesia 2021Micheal ShawkyNo ratings yet
- Hipaa Privacy NoticeDocument5 pagesHipaa Privacy Noticeapi-580264080No ratings yet
- Hse Induction: KYK Analysis of Potentially Hazardous Area (JSA)Document1 pageHse Induction: KYK Analysis of Potentially Hazardous Area (JSA)teman k3No ratings yet
- Case Module For Antenatal CaseDocument17 pagesCase Module For Antenatal CaseCyril JosephNo ratings yet
- Kerala Floods - 2018: A Report by Archbishop Andrews ThazhathDocument31 pagesKerala Floods - 2018: A Report by Archbishop Andrews Thazhathsunil unnithanNo ratings yet
- Effects of Alcoholism To The BehaviourDocument4 pagesEffects of Alcoholism To The BehaviourJoylyn PerezNo ratings yet
- Ubretid 5mg Tablets PIDocument3 pagesUbretid 5mg Tablets PInovitalumintusariNo ratings yet
- Ficha Seguridad 10w30 VentracDocument11 pagesFicha Seguridad 10w30 VentracCarlos VillanuevaNo ratings yet
- SHEA Position Paper: I C H EDocument17 pagesSHEA Position Paper: I C H EIFRS SimoNo ratings yet
- INDIA - NRHM Common Review Mission - Fifth ReportDocument252 pagesINDIA - NRHM Common Review Mission - Fifth ReportKaushik BanerjeeNo ratings yet
- Acute Management of Pulmonary Embolism - American College of CardiologyDocument22 pagesAcute Management of Pulmonary Embolism - American College of CardiologyRaja GopalNo ratings yet
- Truddi ChaseDocument10 pagesTruddi ChaseAnalia WriterNo ratings yet
- PresentationDocument40 pagesPresentationabimub100% (1)