Download as pdf or txt
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5834)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1093)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (852)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (903)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (541)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (349)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (823)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (405)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Molecular Virology - Moses P. AdogaDocument178 pagesMolecular Virology - Moses P. AdogaDavid Orjuela100% (6)
- MSC Biotechnology Assignment QuestionpapersDocument1 pageMSC Biotechnology Assignment QuestionpapersAISHA MUHAMMADNo ratings yet
- Nagesh Gym Final Project Work2Document72 pagesNagesh Gym Final Project Work2Vishal PanditNo ratings yet
- Nutrigenomics: What Will We Be Eating TomorrowDocument10 pagesNutrigenomics: What Will We Be Eating TomorrowPutri OktaviantyNo ratings yet
- B.pharma 2 SemDocument13 pagesB.pharma 2 Semabhishek.thokeNo ratings yet
- REMEDIAL QUIZ q2m2Document3 pagesREMEDIAL QUIZ q2m2Vannie MonderoNo ratings yet
- Rajah 1 Menunjukkan Struktur Utama Membran Plasma.: Ulangkaji Topik Tingkatan 4 Biologi Pergerakan Bahan Mrentasi MembranDocument21 pagesRajah 1 Menunjukkan Struktur Utama Membran Plasma.: Ulangkaji Topik Tingkatan 4 Biologi Pergerakan Bahan Mrentasi MembranHerdawati HamdanNo ratings yet
- Arms PCRDocument14 pagesArms PCRuzmaNo ratings yet
- Module5 MARCHMIDTERMfinalmodule Biochemwithpages2021-22Document15 pagesModule5 MARCHMIDTERMfinalmodule Biochemwithpages2021-22Maden betoNo ratings yet
- 11 - Carbohydrate MetabolismDocument68 pages11 - Carbohydrate MetabolismcheckmateNo ratings yet
- Mericon™ Quant GMO HandbookDocument44 pagesMericon™ Quant GMO HandbookAnisoara HolbanNo ratings yet
- Chapter 5 The Fundamental Unit of LifeDocument18 pagesChapter 5 The Fundamental Unit of LifeTownship TownshipNo ratings yet
- Rational Drug Design Methods Gadavala SarahDocument25 pagesRational Drug Design Methods Gadavala SarahSejal khuman100% (1)
- MDRO A Review 2019Document9 pagesMDRO A Review 2019Muhammad Dody HermawanNo ratings yet
- Carbohydrates Post LabDocument4 pagesCarbohydrates Post LabAki OtaniNo ratings yet
- Biographic of YogiDocument21 pagesBiographic of YogiKaveen VijayNo ratings yet
- Biosynthesis and Pharmacognosy Lecture 2 - Biosynthesis of CarbohydratesDocument19 pagesBiosynthesis and Pharmacognosy Lecture 2 - Biosynthesis of CarbohydratesFrogWarriorNo ratings yet
- BIOL311new Course Outline Fall2021 2022 v2Document3 pagesBIOL311new Course Outline Fall2021 2022 v2Layan BayyaNo ratings yet
- PhysiologyWorkbook7 5Document267 pagesPhysiologyWorkbook7 5SophiaNo ratings yet
- Escherichia Coli As A Model Organism and Its Application in Biotechnology PDFDocument23 pagesEscherichia Coli As A Model Organism and Its Application in Biotechnology PDFPerla AlvaradoNo ratings yet
- 392BNYS SyllabusDocument165 pages392BNYS SyllabusDeepak BaidyaNo ratings yet
- Nonalcoholic Steatohepatitis DR Harbans SinghDocument3 pagesNonalcoholic Steatohepatitis DR Harbans SinghHarbans Singh100% (1)
- The Scientist - 2019 Tale of Two GenomesDocument5 pagesThe Scientist - 2019 Tale of Two GenomesOksanaNo ratings yet
- Bioinformatic Analysis of Selected Natural Compounds For Antidiabetic PotentialDocument12 pagesBioinformatic Analysis of Selected Natural Compounds For Antidiabetic PotentialEditor IJTSRDNo ratings yet
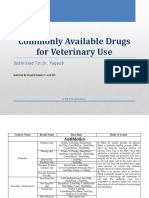
- Commonly Available Drugs For Veterinary Use: Submitted To: Dr. YaqoobDocument21 pagesCommonly Available Drugs For Veterinary Use: Submitted To: Dr. YaqoobUbaid HassanNo ratings yet
- 12054Document5 pages12054NehaGoyalNo ratings yet
- FT1043 Lecture 1Document40 pagesFT1043 Lecture 1Norzhafarina M. IsmailNo ratings yet
- Anti-Phospholipase A Receptor IIFT: A Milestone in The Diagnosis of IMNDocument1 pageAnti-Phospholipase A Receptor IIFT: A Milestone in The Diagnosis of IMNnbiolab6659No ratings yet
- DrMinaSamuel-BioEST-ACT-AP-Notes-3&4-Biochemistry & Enzymes-2022Document17 pagesDrMinaSamuel-BioEST-ACT-AP-Notes-3&4-Biochemistry & Enzymes-2022Nour ShahdNo ratings yet
- Materi Onkologi DasarDocument27 pagesMateri Onkologi DasarMfahrul RoziNo ratings yet