Download as pdf or txt
You might also like
- The Effect Back Massage To The Height of UterineDocument4 pagesThe Effect Back Massage To The Height of UterineMuhamammad Salamuddin Al-AzhafNo ratings yet
- SSS Maternity RequirementsDocument5 pagesSSS Maternity RequirementsWeng Malate67% (3)
- Maternal and Child Health Nursing, 8 Edition.: LESSON PREVIEW/REVIEW (5 Minutes)Document7 pagesMaternal and Child Health Nursing, 8 Edition.: LESSON PREVIEW/REVIEW (5 Minutes)raker boiNo ratings yet
- Ncma219 Lec MidtermDocument51 pagesNcma219 Lec MidtermMacababbad Joshua MiguelNo ratings yet
- MCN 4th QuizDocument27 pagesMCN 4th Quizastraeax pandaNo ratings yet
- DS (Ibuprofen)Document6 pagesDS (Ibuprofen)Mary April MendezNo ratings yet
- 2 The Reproductive SystemDocument122 pages2 The Reproductive SystemBryan Lloyd Ballestar RayatNo ratings yet
- Pros and Cons About AbortionDocument3 pagesPros and Cons About AbortionHeru PamitanMinggatt AssalamualaikumNo ratings yet
- Prelim Outline - Bioethics BSNDocument11 pagesPrelim Outline - Bioethics BSNSheenaNo ratings yet
- Module II: Care of At-Risk / High Risk and Sick Mother (Part I)Document47 pagesModule II: Care of At-Risk / High Risk and Sick Mother (Part I)Hakdog ShermolangNo ratings yet
- Prelim Reviewer 2023Document83 pagesPrelim Reviewer 2023jakexsanchez1515No ratings yet
- Finals Exam Ncm209Document91 pagesFinals Exam Ncm209Shang MarianoNo ratings yet
- NCMB312 RLE-Burn Injuries-Group 3Document56 pagesNCMB312 RLE-Burn Injuries-Group 3Maica LectanaNo ratings yet
- Obgyn Abbreviations For RotationDocument2 pagesObgyn Abbreviations For RotationBigBoostingNo ratings yet
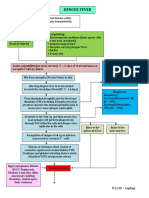
- Denguefever 180705234058Document2 pagesDenguefever 180705234058PLDT HOMENo ratings yet
- NCM 109 Week 8Document17 pagesNCM 109 Week 8Georgia Shayne CubeloNo ratings yet
- SDL - 4.pdf AnotherDocument3 pagesSDL - 4.pdf AnotherJose Troy NgoaNo ratings yet
- CHN1 LP 2 QuianoDocument27 pagesCHN1 LP 2 QuianoMargarette GeresNo ratings yet
- Drug-Study HydrocortisoneDocument4 pagesDrug-Study HydrocortisoneChristian Neil PonceNo ratings yet
- Hydrocephalus in Adult PresentDocument25 pagesHydrocephalus in Adult PresentmarthintoriNo ratings yet
- MCN Final ExamDocument39 pagesMCN Final ExamAshley RegisNo ratings yet
- BSN 2B 2d CASE STUDY FinalDocument35 pagesBSN 2B 2d CASE STUDY Finalann camposNo ratings yet
- Pediatric Community Acquired Pneumonia - Moderate Risk: University of The Cordilleras College of NursingDocument22 pagesPediatric Community Acquired Pneumonia - Moderate Risk: University of The Cordilleras College of NursingJemimah AdaclogNo ratings yet
- Patricia BennerDocument51 pagesPatricia BennerCzerwin JualesNo ratings yet
- Rle FinalsDocument9 pagesRle FinalsMary Florence VelardeNo ratings yet
- Diabetes Mellitus NCPDocument6 pagesDiabetes Mellitus NCPJOHN CARLO APATANNo ratings yet
- Ramos-2bn NCP Delivery RoomDocument2 pagesRamos-2bn NCP Delivery RoomLouwella RamosNo ratings yet
- Headnursing Final OutputDocument30 pagesHeadnursing Final OutputCharissa Magistrado De LeonNo ratings yet
- Group 2 - Technology As A Way of RevealingDocument50 pagesGroup 2 - Technology As A Way of Revealinggenar greg tubogNo ratings yet
- ParacetamolDocument4 pagesParacetamolGermin CesaNo ratings yet
- Chapter 12: Nursing Care To Promote Fetal and Maternal HealthDocument9 pagesChapter 12: Nursing Care To Promote Fetal and Maternal HealthAlyssaGrandeMontimorNo ratings yet
- SAS 13 - Capangpangan, Trisha Mariz M.Document3 pagesSAS 13 - Capangpangan, Trisha Mariz M.Bernadeth Barrientos ZamoraNo ratings yet
- Maternal and Child Health Nursing 1 Long ExamDocument7 pagesMaternal and Child Health Nursing 1 Long ExamAllyza Jane SartigaNo ratings yet
- Fluids and ElectrolytesDocument79 pagesFluids and ElectrolytesReignallienn Inocencio MartinNo ratings yet
- Health Teaching Plan For Newborn ScreeningDocument4 pagesHealth Teaching Plan For Newborn ScreeningPrincess Pauline AbrasaldoNo ratings yet
- Pharmacology Abbreviations and MeasurementDocument3 pagesPharmacology Abbreviations and Measurementronique reidNo ratings yet
- Ra 7600Document5 pagesRa 7600WeGovern InstituteNo ratings yet
- Stages of Labor and DeliveryDocument4 pagesStages of Labor and DeliveryvienreyNo ratings yet
- NCM 112 - Med SurgDocument7 pagesNCM 112 - Med SurgKierzteen Brianna TaromaNo ratings yet
- Case PresDocument100 pagesCase PresJoj BagnateNo ratings yet
- Newborn Journal PDFDocument8 pagesNewborn Journal PDFRose Ann ManalastasNo ratings yet
- RevisedDocument16 pagesRevisedZymer Lee AbasoloNo ratings yet
- Drug Study FUROSEMIDE (Eugene San)Document2 pagesDrug Study FUROSEMIDE (Eugene San)Ana LanticseNo ratings yet
- General Malvar ST., Davao CityDocument5 pagesGeneral Malvar ST., Davao CityKhim BalcitaNo ratings yet
- MCN MT 2Document19 pagesMCN MT 2Jekka Ann Dela CruzNo ratings yet
- BSN 1 J Case Application Interactive TheoriesDocument8 pagesBSN 1 J Case Application Interactive TheoriesAntonio EscotoNo ratings yet
- Community Health Survey ToolDocument6 pagesCommunity Health Survey ToolYna EstabilloNo ratings yet
- NCM 106 Quiz 1Document4 pagesNCM 106 Quiz 1poleene de leonNo ratings yet
- Martha Rogers, Dorothea Orem, Imogene KingDocument9 pagesMartha Rogers, Dorothea Orem, Imogene KingCASTRO, ANDREI KARL Z.No ratings yet
- Sas 11 LectureDocument3 pagesSas 11 LectureFretchel Grace Silverado MesaNo ratings yet
- Meniere's DiseaseDocument32 pagesMeniere's DiseaseMOISED MOisedm100% (1)
- SAS-7 Writing ENG189 FR PDFDocument5 pagesSAS-7 Writing ENG189 FR PDFTherese Joy Gernel SantaceraNo ratings yet
- Community DiagnosisDocument184 pagesCommunity Diagnosisstephanie valerioNo ratings yet
- Module 3 Responsibilities of A Beginning Nurse ResearcherDocument9 pagesModule 3 Responsibilities of A Beginning Nurse ResearcherCaitlynNo ratings yet
- OB Ward Exposure Prepared By: Group G and Group HDocument10 pagesOB Ward Exposure Prepared By: Group G and Group HJannah Marie A. DimaporoNo ratings yet
- Reflection PaperDocument3 pagesReflection PaperBRENCY CLAIRE ALURANNo ratings yet
- Guide in Making The FCA 1Document18 pagesGuide in Making The FCA 1Zedrake CaraanNo ratings yet
- Module 2Document11 pagesModule 2mirai desuNo ratings yet
- Minutes) Everybody WritesDocument15 pagesMinutes) Everybody WritesRanes AndyNo ratings yet
- Drug StudyDocument4 pagesDrug Studyjasper pachingelNo ratings yet
- NCM 109 Problems With Power DraftDocument3 pagesNCM 109 Problems With Power DraftJP Porras Ali100% (1)
- Leopold'S Maneuvers: Multiple ChoiceDocument11 pagesLeopold'S Maneuvers: Multiple ChoiceErcel ArellanoNo ratings yet
- Diagnosis, Evaluation, and Management of Diseases During PregnancyDocument344 pagesDiagnosis, Evaluation, and Management of Diseases During Pregnancyyk4vf286wzNo ratings yet
- Partido State University: Republic of The Philippines Goa, Camarines SurDocument2 pagesPartido State University: Republic of The Philippines Goa, Camarines SurChano Pacamarra100% (1)
- MTP Act 2021Document13 pagesMTP Act 2021hiranyaupadhyayaNo ratings yet
- Hepatitis B in Pregnancy PDFDocument38 pagesHepatitis B in Pregnancy PDFAlsyNo ratings yet
- 1 WichamDocument34 pages1 WichamBhawna JoshiNo ratings yet
- Abortion Controversy Paper PresentationDocument10 pagesAbortion Controversy Paper Presentationapi-507327723No ratings yet
- 5222sampul 130. 2Document19 pages5222sampul 130. 2Riskaa OktavianaNo ratings yet
- Complications of PregnancyDocument33 pagesComplications of PregnancyMilagros Maglasang100% (1)
- Biology AssignmentDocument32 pagesBiology AssignmentZul HanifNo ratings yet
- Pro-Choice Violence in MassachusettsDocument15 pagesPro-Choice Violence in MassachusettsHuman Life InternationalNo ratings yet
- Dr. Ysr University of Health Sciences, Ap, Vijayawada - 08 College Wise Allotment List of MSC Nursing Courses, (Phase I), 2022-23Document6 pagesDr. Ysr University of Health Sciences, Ap, Vijayawada - 08 College Wise Allotment List of MSC Nursing Courses, (Phase I), 2022-23Pattem StellaNo ratings yet
- Effects of The Male Deer Exercise:: 'Why The Strange Salutation?' 3 Big Tantric SecretsDocument1 pageEffects of The Male Deer Exercise:: 'Why The Strange Salutation?' 3 Big Tantric SecretsfahimNo ratings yet
- Molar PregnancyDocument1 pageMolar Pregnancymawel100% (1)
- Tantra and Female EjaculationDocument4 pagesTantra and Female EjaculationRockdorkNo ratings yet
- Lesson 6 SspeDocument12 pagesLesson 6 SspeMa. Leonor Nikka CuevasNo ratings yet
- Cephalopelvic Disproportion FinalDocument7 pagesCephalopelvic Disproportion FinalJesie Mel Bacena100% (2)
- Infertility, Investigation and Management: Dr. Raedah Al-FadhliDocument64 pagesInfertility, Investigation and Management: Dr. Raedah Al-Fadhliapi-3703352No ratings yet
- Cord Prolapse ScriptDocument9 pagesCord Prolapse ScriptDarwin QuirimitNo ratings yet
- RL 5.3 10 - Besar Penyakit Rawat Inap Maret 2021Document6 pagesRL 5.3 10 - Besar Penyakit Rawat Inap Maret 2021Fitri AnisaNo ratings yet
- Third Assignment (Forensic)Document2 pagesThird Assignment (Forensic)Dean Mark AnacioNo ratings yet
- AbortionDocument29 pagesAbortionMujeeb Choudhary100% (2)
- Capital Area Pregnancy Centers Media KitDocument16 pagesCapital Area Pregnancy Centers Media Kitapi-326916153No ratings yet
- Edukasi HIV/AIDS "Gerakan 1000 Remaja Millenial Peduli Odha" (Gerserha) Di MA Al-Mukhtariyah Kabupaten Bandung BaratDocument8 pagesEdukasi HIV/AIDS "Gerakan 1000 Remaja Millenial Peduli Odha" (Gerserha) Di MA Al-Mukhtariyah Kabupaten Bandung BaratFitri AnggrainiNo ratings yet
- 2021 - Unfpa Supplies Partnership Annual Report 2021 - Setting The Stage For SustainabilityDocument60 pages2021 - Unfpa Supplies Partnership Annual Report 2021 - Setting The Stage For SustainabilityMajor General Adekunle AdeyinkaNo ratings yet
- High-Risk Pregnancy Premature Rupture of Membranes (PROM)Document3 pagesHigh-Risk Pregnancy Premature Rupture of Membranes (PROM)elimcangcoNo ratings yet
- Ob Biophysical Profile Protocol r14 PDFDocument3 pagesOb Biophysical Profile Protocol r14 PDFapi-390240132No ratings yet
- EwdsdeklksdlkDocument2 pagesEwdsdeklksdlkAtanda UthmanNo ratings yet
- ARTICLE 165. Children Conceived and Born Outside A Valid Marriage Are IllegitimateDocument2 pagesARTICLE 165. Children Conceived and Born Outside A Valid Marriage Are IllegitimateJeric BonNo ratings yet