Download as docx, pdf, or txt
You might also like
- Audit's Use of Data Analytics ACL PDFDocument30 pagesAudit's Use of Data Analytics ACL PDFjmonsa11No ratings yet
- Onboarding Checklist Form - DO NOT OVERWRITE PDFDocument2 pagesOnboarding Checklist Form - DO NOT OVERWRITE PDFRezzaNo ratings yet
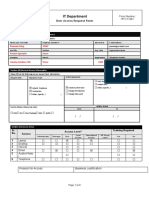
- IT Access Request FormDocument4 pagesIT Access Request FormCSKNo ratings yet
- FM OO3 01.18 Kabuhayan Beneficiary Profile Form 022023Document1 pageFM OO3 01.18 Kabuhayan Beneficiary Profile Form 022023Mary Chris Celoso MedinaNo ratings yet
- Exit Clearance Form (2020)Document1 pageExit Clearance Form (2020)Juvilyn ValeraNo ratings yet
- Support FormDocument2 pagesSupport FormAnik GhoshNo ratings yet
- Exit Clearance FormDocument1 pageExit Clearance FormHannah Krisha AmorNo ratings yet
- Application Form For Global Ambassadors: Personal DetailsDocument2 pagesApplication Form For Global Ambassadors: Personal DetailsGilson JúniorNo ratings yet
- Resigned ChecklistDocument2 pagesResigned ChecklistMaria DanialNo ratings yet
- DCF - Several Forms - Batch 1 March 12, 2021Document2 pagesDCF - Several Forms - Batch 1 March 12, 2021Jofit DayocNo ratings yet
- Neptune Application Package - 2019 DecemberDocument19 pagesNeptune Application Package - 2019 Decemberjay gandhiNo ratings yet
- First National Commercial New Business Application (Updated)Document9 pagesFirst National Commercial New Business Application (Updated)marNo ratings yet
- BCI TWI Enrolment FormDocument4 pagesBCI TWI Enrolment FormJustin DiraviarajNo ratings yet
- POE AlterraDSDocument2 pagesPOE AlterraDSmariobros24No ratings yet
- Mobile Phone Requisition Form - Updated Dec 2022Document1 pageMobile Phone Requisition Form - Updated Dec 2022Samir AkramNo ratings yet
- UBP Corp Credit Card Application Form - New FillableDocument7 pagesUBP Corp Credit Card Application Form - New FillableAdam Albert DomendenNo ratings yet
- SAI - TWI India Enrolment Form From As Per Rev25 IndiaDocument4 pagesSAI - TWI India Enrolment Form From As Per Rev25 Indiavarunchopra0501No ratings yet
- Bio Data: Place 1 (Colored) Passport Size Photo Here & Attach Another Duly AttestedDocument3 pagesBio Data: Place 1 (Colored) Passport Size Photo Here & Attach Another Duly AttestedJeraldNo ratings yet
- Pelkon III Application Form v4Document1 pagePelkon III Application Form v4freddieckngNo ratings yet
- Membership Form: Upes Spe Student ChapterDocument1 pageMembership Form: Upes Spe Student Chapterkayastha shriNo ratings yet
- 5 2551442 Prospective Employee Declaration 7-19-2022 9 16 28 PMDocument2 pages5 2551442 Prospective Employee Declaration 7-19-2022 9 16 28 PMShauryaNo ratings yet
- CCA Membership Application: International Federation of Professional ManagersDocument1 pageCCA Membership Application: International Federation of Professional ManagersMarielle AngelesNo ratings yet
- Training Program: 1. Personal InformationDocument3 pagesTraining Program: 1. Personal Information03151206639No ratings yet
- Biodata SampleAAAADocument3 pagesBiodata SampleAAAAMarilou DivinagraciaNo ratings yet
- HR Bio Data Sample: Place 1 (Colored) Passport Size Photo Here & Attach Another Duly AttestedDocument3 pagesHR Bio Data Sample: Place 1 (Colored) Passport Size Photo Here & Attach Another Duly AttestedMatagal NaNo ratings yet
- Letter of Request Application Form Updated2020Document1 pageLetter of Request Application Form Updated2020Jhasmin GierranNo ratings yet
- Agency Funds Expenditure DetailsDocument1 pageAgency Funds Expenditure Detailsindo jinNo ratings yet
- TER Number: Title: Activity: Type:: District Staff MeetingDocument7 pagesTER Number: Title: Activity: Type:: District Staff MeetingOblino NicaNo ratings yet
- TWI Enrolment Form: TWI Training & Examination ServicesDocument4 pagesTWI Enrolment Form: TWI Training & Examination ServicesSamsuNo ratings yet
- Request SlipDocument1 pageRequest SlipMark TepaceNo ratings yet
- Sponsored DefenceDocument3 pagesSponsored DefencempbnqNo ratings yet
- BIO DATA Employee FormDocument3 pagesBIO DATA Employee FormSen RafaelNo ratings yet
- Langganan Dnet 2021Document2 pagesLangganan Dnet 2021nando745No ratings yet
- Petty Cash NewDocument2 pagesPetty Cash NewAli ShiblianNo ratings yet
- POE E ServicesDocument2 pagesPOE E Servicesmariobros24No ratings yet
- System Administrator Designation FormDocument2 pagesSystem Administrator Designation FormKyssel SeyerNo ratings yet
- 6 3081979 Prospective Employee Declaration 7-3-2023 4 14 12 PMDocument2 pages6 3081979 Prospective Employee Declaration 7-3-2023 4 14 12 PMMeenakshi VermaNo ratings yet
- Event ManagementDocument56 pagesEvent ManagementgowriNo ratings yet
- Online Recruitment System: For Discussion Only (Sample Site Design and Information Flow)Document13 pagesOnline Recruitment System: For Discussion Only (Sample Site Design and Information Flow)humayunsagguNo ratings yet
- Vendor Bank Information Request v2.4Document1 pageVendor Bank Information Request v2.4TengkuFarisTengkuKhalidNo ratings yet
- Evsjv 'K KW Úduvimwgwz Company/Organization Information: Bangladesh Computer SamityDocument1 pageEvsjv 'K KW Úduvimwgwz Company/Organization Information: Bangladesh Computer SamityKalPurushNo ratings yet
- Web Site/Application Hosting Registration Form: Contact PersonDocument4 pagesWeb Site/Application Hosting Registration Form: Contact PersonrohitnukalaNo ratings yet
- 21-02-2020 - Upgrade MemoriDocument1 page21-02-2020 - Upgrade MemoriAde SuharyadiNo ratings yet
- Shyam KVAP235716-11848293KU1VBTQNMWDocument1 pageShyam KVAP235716-11848293KU1VBTQNMWMasood RabbaniNo ratings yet
- CLIENT APPLICATION FORM PayDocument2 pagesCLIENT APPLICATION FORM PayKarla Jeanne CoNo ratings yet
- Gateway - Career Support Registration & Interview FormDocument2 pagesGateway - Career Support Registration & Interview FormHealep De LucisNo ratings yet
- Mis SRF2022Document1 pageMis SRF2022R. REYESNo ratings yet
- Procurement Request Form - Blanl - Final Version 5 17 2 23Document2 pagesProcurement Request Form - Blanl - Final Version 5 17 2 23Nigel PhippsNo ratings yet
- 6 3445522 Prospective Employee Declaration 11-21-2023 1 04 10 AMDocument2 pages6 3445522 Prospective Employee Declaration 11-21-2023 1 04 10 AMadithyakadammhadhiNo ratings yet
- 5 - 1409281 - Prospective - Employee - Declaration - 8 - 13 - 2020 5 - 29 - 03 PMDocument2 pages5 - 1409281 - Prospective - Employee - Declaration - 8 - 13 - 2020 5 - 29 - 03 PMSaquib ShaikhNo ratings yet
- IT Tools and Access Request FormDocument4 pagesIT Tools and Access Request FormAllison CasiquinNo ratings yet
- DPISG Requirements Assessment Form - Ericsson - PA1Document1 pageDPISG Requirements Assessment Form - Ericsson - PA1Sukanta MandalNo ratings yet
- National Information Technology CenterDocument2 pagesNational Information Technology CenterAman SharmaNo ratings yet
- GOC GoBusiness LicensingDocument2 pagesGOC GoBusiness Licensingwim006No ratings yet
- ERP (SAP) Acess Request FormDocument2 pagesERP (SAP) Acess Request FormGaurav RoyNo ratings yet
- 32 - KO - RDD - STR 2020 - Kick Off DocumentsDocument2 pages32 - KO - RDD - STR 2020 - Kick Off DocumentsKasunTilinaChathurangaNo ratings yet
- VACATION LEAVE July 2024Document1 pageVACATION LEAVE July 2024Sikandar KhanNo ratings yet
- Company: APJ Software Private Limited Job Position: IT Software - Engineer Interview DetailsDocument1 pageCompany: APJ Software Private Limited Job Position: IT Software - Engineer Interview Detailssushmit raj badolaNo ratings yet
- Event Success: Maximizing the Business Impact of In-person, Virtual, and Hybrid ExperiencesFrom EverandEvent Success: Maximizing the Business Impact of In-person, Virtual, and Hybrid ExperiencesNo ratings yet
- App Market Research TemplateDocument5 pagesApp Market Research TemplateSwapneel GhadageNo ratings yet
- Mobile App Development Proposal Form Client Information Project DetailsDocument11 pagesMobile App Development Proposal Form Client Information Project Detailsjoy ramiloNo ratings yet
- Multi-Dimensional Reporting With PivottablesDocument4 pagesMulti-Dimensional Reporting With PivottablesVarenya KumarNo ratings yet
- Template GANT Project in ExcelDocument5 pagesTemplate GANT Project in ExceledisontoNo ratings yet
- VNX Events and Retention Suite FundamentalsDocument23 pagesVNX Events and Retention Suite Fundamentalsabctester2552No ratings yet
- VM RecommendationsDocument2 pagesVM RecommendationsAntonio MouraNo ratings yet
- Ddoocp Ms March2012 FinalDocument11 pagesDdoocp Ms March2012 FinalSarge ChisangaNo ratings yet
- Ieav2r4 SDSFDocument94 pagesIeav2r4 SDSFBurhan MalikNo ratings yet
- 06 Practice 6 Getting Familiar With Oracle EM Database ExpressDocument12 pages06 Practice 6 Getting Familiar With Oracle EM Database ExpressAbdo MohamedNo ratings yet
- Oracle Autovue 20.2.1: Quick Install GuideDocument16 pagesOracle Autovue 20.2.1: Quick Install GuideM Mirac CicekNo ratings yet
- TSM HSMDocument188 pagesTSM HSMChitranjan KumarNo ratings yet
- Chapter One Office Automation SystemsDocument3 pagesChapter One Office Automation SystemssalehNo ratings yet
- Rupali Shukla Latest Resume - Rupali ShuklaDocument1 pageRupali Shukla Latest Resume - Rupali ShuklaMohit KokilNo ratings yet
- Creating 3d BuildingsDocument6 pagesCreating 3d Buildingsjulioea6354No ratings yet
- BI-Integrated Planning Using BEx Query + Analysis For Office - Visual BI SolutionsDocument6 pagesBI-Integrated Planning Using BEx Query + Analysis For Office - Visual BI SolutionsDanial SabirNo ratings yet
- Chap 2 - Installing UltraPIPEDocument10 pagesChap 2 - Installing UltraPIPEbismarckandresNo ratings yet
- EW Harp ManualDocument14 pagesEW Harp ManualMatheus FrancoNo ratings yet
- Using Office Backstage: Lesson Skill MatrixDocument13 pagesUsing Office Backstage: Lesson Skill MatrixMary Jane PagayNo ratings yet
- Project InformationDocument3 pagesProject InformationhakiNo ratings yet
- Modifying and Using Engineering Library Data: ProblemDocument5 pagesModifying and Using Engineering Library Data: Problemselamawit workinehNo ratings yet
- Chapter 8: Main Memory: Silberschatz, Galvin and Gagne ©2013 Operating System Concepts - 9 EditionDocument19 pagesChapter 8: Main Memory: Silberschatz, Galvin and Gagne ©2013 Operating System Concepts - 9 EditionJari AbbasNo ratings yet
- Cadence Platform Support PlanDocument9 pagesCadence Platform Support PlanshilpajosephNo ratings yet
- Hareesh Kumar Mullaguru: EducationDocument2 pagesHareesh Kumar Mullaguru: EducationShareena FernandesNo ratings yet
- Inf1505 May June 2018 MemoDocument20 pagesInf1505 May June 2018 MemoKishan GunasseNo ratings yet
- Icloud Seminar ReportDocument17 pagesIcloud Seminar ReportJamesCarter100% (1)
- Xii Ip Practical Answers File 10Document24 pagesXii Ip Practical Answers File 10saket01nema50% (2)
- Bronze Edition V 6 ManualDocument262 pagesBronze Edition V 6 ManualmahyarbNo ratings yet
- 11 Adobe - Creative - Suite - 5 - 5 - Design - Premium - DatasheetDocument2 pages11 Adobe - Creative - Suite - 5 - 5 - Design - Premium - DatasheetPatrick BukamNo ratings yet
- Oracle Reports TutorialDocument38 pagesOracle Reports TutorialTomas Mendoza LoeraNo ratings yet