Download as pdf or txt
You might also like
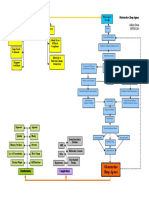
- Sleep Apnea Concept MapDocument1 pageSleep Apnea Concept Mapashleydean100% (2)
- Unit-5 Ventilation Breathing QuestionsDocument37 pagesUnit-5 Ventilation Breathing Questionsareyouthere92100% (1)
- NCP - Impaired Gas ExchangeDocument4 pagesNCP - Impaired Gas ExchangeRene John Francisco100% (1)
- Non Invasive Ventilation in PediatricsDocument192 pagesNon Invasive Ventilation in Pediatricstj1983tj0% (1)
- Anatomy and Physiology Test Final PDFDocument3 pagesAnatomy and Physiology Test Final PDFLALRINTLUANGI CHHAKCHHUAKNo ratings yet
- Mecánica en SdraDocument11 pagesMecánica en Sdracarlos ruiz perezNo ratings yet
- ARDS Vs CARDSDocument7 pagesARDS Vs CARDSسلطان الحنبصيNo ratings yet
- Lung Function Assessment by ImpulseDocument12 pagesLung Function Assessment by Impulsethiago gibsonNo ratings yet
- 931 2169 1 PBDocument9 pages931 2169 1 PBThithiraNo ratings yet
- Applsci 09 02842 PDFDocument13 pagesApplsci 09 02842 PDFFelicia SutarliNo ratings yet
- Ding 2022 Small Airway Dysfunction in ChronicDocument7 pagesDing 2022 Small Airway Dysfunction in ChronicDylanNo ratings yet
- Hudson Et Al 2016 Electroencephalographic Detection of Respiratory Related Cortical Activity in Humans From EventDocument10 pagesHudson Et Al 2016 Electroencephalographic Detection of Respiratory Related Cortical Activity in Humans From EventSIVAMATHIVANAN P 22MTL129No ratings yet
- Respiratory Physiology & NeurobiologyDocument5 pagesRespiratory Physiology & Neurobiologyrafi surya ghaniNo ratings yet
- Role of The Cholinergic Pathway Airway Response To Emotional Stimuli in Asthma: TheDocument9 pagesRole of The Cholinergic Pathway Airway Response To Emotional Stimuli in Asthma: TheLuis RicardoNo ratings yet
- Lung Protective Ventilatory (Estrategias Ventilatorias de Protección Pulmonar)Document24 pagesLung Protective Ventilatory (Estrategias Ventilatorias de Protección Pulmonar)Jesus FrancoNo ratings yet
- Costa Et Al 2021 Ventilatory Variables and Mechanical Power in Patients With Acute Respiratory Distress SyndromeDocument9 pagesCosta Et Al 2021 Ventilatory Variables and Mechanical Power in Patients With Acute Respiratory Distress SyndromePepeee:DNo ratings yet
- The Relationship Between Duration of Asthma and Pulmonary Function Test Parameters in Patients With Mild To Moderate AsthmaDocument5 pagesThe Relationship Between Duration of Asthma and Pulmonary Function Test Parameters in Patients With Mild To Moderate AsthmaInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Hfo 2Document9 pagesHfo 2markus_danusantosoNo ratings yet
- Lung Tissue Resistance in Diffuse Interstitial Pulmonary FibrosisDocument9 pagesLung Tissue Resistance in Diffuse Interstitial Pulmonary FibrosisEndhy KurniawanNo ratings yet
- BD in VM EditorialDocument2 pagesBD in VM EditorialTavo Aravena TorresNo ratings yet
- CF Ventilation ManagementDocument10 pagesCF Ventilation ManagementSherry SaidNo ratings yet
- Aerosol Delivery Via Invasive Ventilation - A Narrative Review 2021Document17 pagesAerosol Delivery Via Invasive Ventilation - A Narrative Review 2021claudiocraisseNo ratings yet
- Methods To Evaluate Airway Resistance and Lung Compliance During Mechanical Ventilation A Comparative StudyDocument5 pagesMethods To Evaluate Airway Resistance and Lung Compliance During Mechanical Ventilation A Comparative StudyInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Airway Pressure Release VentilatiDocument9 pagesAirway Pressure Release VentilatiDavid ParraNo ratings yet
- Ali PathopysDocument6 pagesAli PathopysYudo PrabowoNo ratings yet
- Ug201210041electrical Model of LungsDocument2 pagesUg201210041electrical Model of LungsAyush BhadauriaNo ratings yet
- Ards PronoDocument10 pagesArds PronoARELHI ROSARIO GARCIA MONROYNo ratings yet
- Driving Pressure PDFDocument4 pagesDriving Pressure PDFDorian CiobanuNo ratings yet
- Acute Medicine Surgery - 2024 - Hoshino - Future Directions of Lung Protective Ventilation Strategies in AcuteDocument8 pagesAcute Medicine Surgery - 2024 - Hoshino - Future Directions of Lung Protective Ventilation Strategies in AcuteDiego AzevedoNo ratings yet
- Relation Between Respiratory Rate and HeDocument4 pagesRelation Between Respiratory Rate and HeMuhammad Naufal NoorrachmanNo ratings yet
- Vol Pulmon Art AcDocument7 pagesVol Pulmon Art AcdanielNo ratings yet
- Effect of Lowering VT On Mortality in Acute Respiratory DistressDocument8 pagesEffect of Lowering VT On Mortality in Acute Respiratory DistressFabio RepettoNo ratings yet
- PRVC in COPDDocument8 pagesPRVC in COPDwandapandabebeNo ratings yet
- Fphys 09 00621Document9 pagesFphys 09 00621SIVAMATHIVANAN P 22MTL129No ratings yet
- Coppola 2021 - Radiological Pattern in ARDS Patients - Partitioned Respiratory Mechanics, Gas Exchange and Lung RecruitabilityDocument10 pagesCoppola 2021 - Radiological Pattern in ARDS Patients - Partitioned Respiratory Mechanics, Gas Exchange and Lung RecruitabilitygiadungdanamallNo ratings yet
- SDRA Ventilacion Alta FrecuenciaDocument8 pagesSDRA Ventilacion Alta FrecuenciaDavid Davoas A. SolizNo ratings yet
- Impulsna Koruga42 75Document5 pagesImpulsna Koruga42 75sstefan888No ratings yet
- Lessons Learned in Acute Respiratory Distress Syndrome From The Animal LaboratoryDocument11 pagesLessons Learned in Acute Respiratory Distress Syndrome From The Animal LaboratoryLaode Muh. Agus SapdimanNo ratings yet
- Reviews: Lung Function Testing Assessment by Impulse Oscillometry in Chronic Lung DiseaseDocument7 pagesReviews: Lung Function Testing Assessment by Impulse Oscillometry in Chronic Lung DiseaseCristiana LibuNo ratings yet
- Jurnal Farmakologi 3Document12 pagesJurnal Farmakologi 3Laode Muh. Agus SapdimanNo ratings yet
- Pronation Reveals A Heterogeneous Response of GlobDocument10 pagesPronation Reveals A Heterogeneous Response of GlobJhoselyn De La Torre OnofreNo ratings yet
- Lung Opening and Closing During Ventilation of Acute Respiratory Distress SyndromeDocument9 pagesLung Opening and Closing During Ventilation of Acute Respiratory Distress Syndromerxh30No ratings yet
- P V Courve in ArdsDocument5 pagesP V Courve in ArdsAdrian BălanNo ratings yet
- Ajustesiniciales VNIDocument3 pagesAjustesiniciales VNIDamian Torres SperanzaNo ratings yet
- CcventilacioninicialbuenoDocument3 pagesCcventilacioninicialbuenoARELHI ROSARIO GARCIA MONROYNo ratings yet
- Invasive Mechanical Ventilation PDFDocument4 pagesInvasive Mechanical Ventilation PDFRaquel AguilarNo ratings yet
- Wang 2022Document11 pagesWang 2022Carlos Daniel AliagaNo ratings yet
- CrirmiDocument6 pagesCrirmistanleyNo ratings yet
- Annalsats 201704-345otDocument10 pagesAnnalsats 201704-345otAmjad SaudNo ratings yet
- AMJ-Volume 50-Issue 2 - Page 1489-1496Document8 pagesAMJ-Volume 50-Issue 2 - Page 1489-1496Pandu Putra Wijaya RestaNo ratings yet
- RCCM 201902-0334ocDocument10 pagesRCCM 201902-0334ocrodolfo riosNo ratings yet
- Borges 2006 Plateau 60Document11 pagesBorges 2006 Plateau 60pablopg_5No ratings yet
- High-Frequency Oscillation For Acute Respiratory Distress SyndromeDocument8 pagesHigh-Frequency Oscillation For Acute Respiratory Distress SyndromeLintang SuroyaNo ratings yet
- Brock 2017Document10 pagesBrock 2017Carlos Daniel AliagaNo ratings yet
- Paper 8, Raymandos 2012Document10 pagesPaper 8, Raymandos 2012NITIN SENTHILKUMARNo ratings yet
- Classification of Sleep-Disordered Breathing: American Journal of Respiratory and Critical Care Medicine March 2001Document9 pagesClassification of Sleep-Disordered Breathing: American Journal of Respiratory and Critical Care Medicine March 2001Stefanus SiswoyoNo ratings yet
- Oscilometrie RespiratorieDocument9 pagesOscilometrie RespiratorieDan PopaNo ratings yet
- 2015 Article 91Document7 pages2015 Article 91Karel ZertucheNo ratings yet
- The Effect of Physiotherapy-Based Breathing Retraining On Asthma ControlDocument10 pagesThe Effect of Physiotherapy-Based Breathing Retraining On Asthma Controlselamat parminNo ratings yet
- A Study of Efficiency of Breathing Exercises To Improve Pulmonary FX in SCi PtsDocument6 pagesA Study of Efficiency of Breathing Exercises To Improve Pulmonary FX in SCi PtsMarion AtienzaNo ratings yet
- Ngo 2016Document11 pagesNgo 2016Carlos Daniel AliagaNo ratings yet
- Zampieri 2019Document8 pagesZampieri 2019Peter AgabaNo ratings yet
- LohiaDocument11 pagesLohiastanleyNo ratings yet
- Evidence-Based Management of Acute Lung Injury and Acute Respiratory Distress SyndromeDocument17 pagesEvidence-Based Management of Acute Lung Injury and Acute Respiratory Distress SyndromeretNo ratings yet
- Monitoring Mechanical Ventilation Using Ventilator WaveformsFrom EverandMonitoring Mechanical Ventilation Using Ventilator WaveformsNo ratings yet
- Updated Hesi Ap V1V2 Study GuideDocument10 pagesUpdated Hesi Ap V1V2 Study GuideichelNo ratings yet
- DR PadmeshDocument25 pagesDR PadmeshNisar ShaikNo ratings yet
- Ineffective AIRWAY CLEARANCE RT Retained Mucus Secretions AEB The (+) Crackles On Both Lower Lung Field.Document2 pagesIneffective AIRWAY CLEARANCE RT Retained Mucus Secretions AEB The (+) Crackles On Both Lower Lung Field.Senyorita KHaye0% (1)
- DR - Wahid Helmi Ped Rev PDFDocument2,088 pagesDR - Wahid Helmi Ped Rev PDFNatalia NatNo ratings yet
- Pengaturan Sistem RespirasiDocument18 pagesPengaturan Sistem RespirasiMaulidya MagfirahNo ratings yet
- Respiratory System Science Revision WorksheetDocument7 pagesRespiratory System Science Revision WorksheetTravel UnlimitedNo ratings yet
- Instructional PlanDocument17 pagesInstructional PlanJamal P. AlawiyaNo ratings yet
- Congenital Lung MalformationsDocument115 pagesCongenital Lung MalformationsAhmad Abu KushNo ratings yet
- Advanced Neonatal Procedure1Document14 pagesAdvanced Neonatal Procedure1Santhosh.S.U100% (1)
- Zdorovye - The Means To PrepareDocument4 pagesZdorovye - The Means To PrepareBrett DrinkwaterNo ratings yet
- ARDS PresentationDocument89 pagesARDS Presentationalexandriaputera30No ratings yet
- 5% HCLDocument7 pages5% HCLJoeco Abay-abayNo ratings yet
- Group 1 (Science-9)Document3 pagesGroup 1 (Science-9)Joslyn Ditona DialNo ratings yet
- Asv Fact SheetDocument2 pagesAsv Fact SheetThanigaiarsu ThiyagarajanNo ratings yet
- NCP & Prio!!!Document45 pagesNCP & Prio!!!Sj 斗力上100% (1)
- Steel Mill Electric Arc Furnace Dust MSDS (NA) 12-8-08Document15 pagesSteel Mill Electric Arc Furnace Dust MSDS (NA) 12-8-08Agustine SetiawanNo ratings yet
- DESIGN OF A BREATHING SIMULATOR GENERATING ADULT AND PEDIATRIC PATTERNS MSC Thesis PDFDocument81 pagesDESIGN OF A BREATHING SIMULATOR GENERATING ADULT AND PEDIATRIC PATTERNS MSC Thesis PDFyekta8No ratings yet
- English For Medicine Part 2 PDFDocument161 pagesEnglish For Medicine Part 2 PDFVictoria VintuNo ratings yet
- HRCT ProtocolsDocument17 pagesHRCT ProtocolsZezo KaraNo ratings yet
- 1.airway, Airflow, Ventilation and DiffusionDocument64 pages1.airway, Airflow, Ventilation and DiffusionEbin EbenezerNo ratings yet
- TB Dots Ri Dan RJ Jan - Juli 2020Document6 pagesTB Dots Ri Dan RJ Jan - Juli 2020Dina MariyanaNo ratings yet
- Human Respiratory System Based On Law of ThermodynamicsDocument9 pagesHuman Respiratory System Based On Law of ThermodynamicsfatimahNo ratings yet
- Reanimation of Rats From Body Temperatures Between 0 and 1°c by Microwave DiathermyDocument6 pagesReanimation of Rats From Body Temperatures Between 0 and 1°c by Microwave DiathermyLJNo ratings yet
- Msds HClO4Document6 pagesMsds HClO4Nur Af-idah Bekti Ardiasih100% (1)
- Chest Injury and Its TypesDocument14 pagesChest Injury and Its TypesKoochi PoojithaNo ratings yet