
Tunneled Catheters
Tunneled Catheters
You might also like
- Andre Tan's Surgical NotesDocument163 pagesAndre Tan's Surgical NotesHani Nadiah75% (4)
- Fundamentals NotesDocument23 pagesFundamentals NotesElle R Naceno100% (5)
- 2019 Book VesselHealthAndPreservationTheDocument303 pages2019 Book VesselHealthAndPreservationTheOigres OdaravalNo ratings yet
- Osce - D&CDocument2 pagesOsce - D&Cmkct111No ratings yet
- Obs Gynae Full Summary NotesDocument41 pagesObs Gynae Full Summary NotesJana Aldour100% (1)
- Medication Calculation Practice Problems: Level Ii, Iii and IvDocument6 pagesMedication Calculation Practice Problems: Level Ii, Iii and IvQueennita100% (7)
- Operating Manual Infusomat Space PDFDocument82 pagesOperating Manual Infusomat Space PDFamirali.bme4527No ratings yet
- Pediatric Nursing An Introductory Text 11th Edition Price Test BankDocument11 pagesPediatric Nursing An Introductory Text 11th Edition Price Test BankDarius67% (3)
- Percutaneous Non-TunneledDocument12 pagesPercutaneous Non-TunneledJunkNo ratings yet
- Implanted Venous Access Device (IVAD) - "Dome" or "Port"Document12 pagesImplanted Venous Access Device (IVAD) - "Dome" or "Port"JunkNo ratings yet
- Percutaneous Non-Tunneled Open-Ended CatheterDocument13 pagesPercutaneous Non-Tunneled Open-Ended CatheterJunkNo ratings yet
- Central VC ModuleDocument11 pagesCentral VC ModuleJunkNo ratings yet
- 20 Trauma Resuscitation Part 2 InterventionsDocument3 pages20 Trauma Resuscitation Part 2 InterventionssueNo ratings yet
- S T A R T: Imple Riage ND Apid ReatmentDocument17 pagesS T A R T: Imple Riage ND Apid ReatmentNavine NavNo ratings yet
- Anaesthesia SummaryDocument36 pagesAnaesthesia SummaryRazan QassemNo ratings yet
- Advanced Life Support: Siska Christianingsih, S.Kep.,Ns.M.KepDocument31 pagesAdvanced Life Support: Siska Christianingsih, S.Kep.,Ns.M.KepFlorenciaNo ratings yet
- Advanced Trauma Life Support RevisedDocument7 pagesAdvanced Trauma Life Support RevisedpaveethrahNo ratings yet
- DR - Noer Rachmat Early Management Pelvic FractureDocument72 pagesDR - Noer Rachmat Early Management Pelvic FractureRsud Malinau Ppk BludNo ratings yet
- Diagnostic Procedures For Respiratory Conditions Non-Invasive & Invasive ProceduresDocument4 pagesDiagnostic Procedures For Respiratory Conditions Non-Invasive & Invasive ProceduresIrish Eunice FelixNo ratings yet
- Cme Trauma Management ZakwanDocument44 pagesCme Trauma Management ZakwansyasyaNo ratings yet
- Airway ManagementDocument4 pagesAirway ManagementEllamae DerupeNo ratings yet
- Primary and Secondary Survey MiraDocument50 pagesPrimary and Secondary Survey MiraAfifah SelamatNo ratings yet
- Emergency Medicine: by DR Maimun ShikderDocument22 pagesEmergency Medicine: by DR Maimun ShikderFarwa RazaNo ratings yet
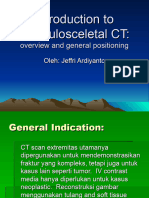
- TM 5-6 - Musculosceletal CT - P. JeffryDocument50 pagesTM 5-6 - Musculosceletal CT - P. Jeffryradiologi.rsgmNo ratings yet
- Tugas Anestesi Rani RevisiDocument27 pagesTugas Anestesi Rani RevisiFahrizalNo ratings yet
- Basic Chest UltrasoundDocument60 pagesBasic Chest UltrasoundAdriana Villarreal100% (2)
- Review NotesDocument5 pagesReview NotesIrish May BalanzaNo ratings yet
- Advanced Trauma Life SupportDocument8 pagesAdvanced Trauma Life SupportAbouzr Mohammed ElsaidNo ratings yet
- General Management of Trauma: The Atls ConceptDocument30 pagesGeneral Management of Trauma: The Atls ConceptWasim R. IssaNo ratings yet
- Airway Control Management, RSPMDocument59 pagesAirway Control Management, RSPMzakia4nisakNo ratings yet
- Airway Control Management, RSPMDocument59 pagesAirway Control Management, RSPMEryanda DinataNo ratings yet
- Approach To TraumaDocument43 pagesApproach To TraumaAlmonz AndoriasNo ratings yet
- 2.1. Trauma and Critical Care (Jerome Villacorta's Conflicted Copy 2013-08-24)Document12 pages2.1. Trauma and Critical Care (Jerome Villacorta's Conflicted Copy 2013-08-24)Miguel C. DolotNo ratings yet
- Trauma Resuscitation Acute Care Emerg MedDocument67 pagesTrauma Resuscitation Acute Care Emerg MedsyasyaNo ratings yet
- Perioperative NursingDocument5 pagesPerioperative NursingMikhaela Andree MarianoNo ratings yet
- Laminectomy: By: RN Nurul Syazwani RosliDocument26 pagesLaminectomy: By: RN Nurul Syazwani RosliMuhammad Nizam AmmNo ratings yet
- 3 Ways To Examine The Larynx: PiriformDocument10 pages3 Ways To Examine The Larynx: PiriformbeautyNo ratings yet
- Pulse OximetryDocument7 pagesPulse OximetryEmerson De SilvaNo ratings yet
- CVS Phsicl ExaminationDocument34 pagesCVS Phsicl ExaminationHassan HarirNo ratings yet
- 2.1. Trauma and Critical CareDocument13 pages2.1. Trauma and Critical CareMiguel C. DolotNo ratings yet
- Radiology Lecture 4th Year 2022 Part 2Document44 pagesRadiology Lecture 4th Year 2022 Part 2Abubakar JallohNo ratings yet
- DR Sujata: Professor Dept - of Anaesthesiology &critical Care Ucms & GTB HospitalDocument53 pagesDR Sujata: Professor Dept - of Anaesthesiology &critical Care Ucms & GTB HospitalMiniNo ratings yet
- SpineDocument83 pagesSpineMohamed Ragab 3mmarNo ratings yet
- Common Musculoskeletal ProblemsDocument17 pagesCommon Musculoskeletal Problemsapi-3822433No ratings yet
- Prevention of Postoperative Complications of CDocument1 pagePrevention of Postoperative Complications of CChinedu H. DuruNo ratings yet
- Gallery Walk PosterDocument1 pageGallery Walk PosterBern NerquitNo ratings yet
- Anesthesia PositionsDocument19 pagesAnesthesia Positionsnicolinna2000yahoo.comNo ratings yet
- Nursing Intervention Respiratory Status: Ventilation Respiratory Status: Airway Patency Vital Sign StatusDocument12 pagesNursing Intervention Respiratory Status: Ventilation Respiratory Status: Airway Patency Vital Sign StatusSepti MemorisaNo ratings yet
- EM - SGD 1 (Airway and Breathing)Document5 pagesEM - SGD 1 (Airway and Breathing)R RNo ratings yet
- General Anesthesia Notes - JalaDocument6 pagesGeneral Anesthesia Notes - JalaJulie Anne AciertoNo ratings yet
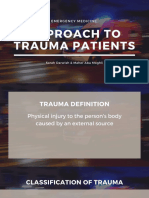
- Approach To Trauma PatientsDocument45 pagesApproach To Trauma PatientsSarahNo ratings yet
- Positioning Patients in BedDocument27 pagesPositioning Patients in BedAldo BGamanNo ratings yet
- Respiratory Paediatrics ExaminationDocument1 pageRespiratory Paediatrics ExaminationRatnahKumar28No ratings yet
- RSI Assessment HODocument4 pagesRSI Assessment HOlalalalalalalalalala happinessNo ratings yet
- Surgery Emergencies: Multiple Trauma: Yonathan Adi PurnomoDocument66 pagesSurgery Emergencies: Multiple Trauma: Yonathan Adi Purnomowaraney palitNo ratings yet
- Airway ManagementDocument129 pagesAirway ManagementSyabie YassinNo ratings yet
- (Mantap) Slide Materi Anestesi Batch 3 2018Document74 pages(Mantap) Slide Materi Anestesi Batch 3 2018Aditya PratamaNo ratings yet
- Respiratory Syatem: January 2009Document19 pagesRespiratory Syatem: January 2009aarti devNo ratings yet
- Airway Managmenat Normal and DifficultDocument49 pagesAirway Managmenat Normal and DifficultHari Om ChaurasiyaNo ratings yet
- WSDDocument50 pagesWSDgraceriaaNo ratings yet
- Eyes To KnowDocument3 pagesEyes To KnowTrisNo ratings yet
- Chest Radiography For InternsDocument42 pagesChest Radiography For InternsRose ValeNo ratings yet
- Cvs ExaminationDocument2 pagesCvs Examinationjenny grovesNo ratings yet
- Implanted Venous Access Device (IVAD) - "Dome" or "Port"Document12 pagesImplanted Venous Access Device (IVAD) - "Dome" or "Port"JunkNo ratings yet
- Percutaneous Non-TunneledDocument12 pagesPercutaneous Non-TunneledJunkNo ratings yet
- Percutaneous Non-Tunneled Open-Ended CatheterDocument13 pagesPercutaneous Non-Tunneled Open-Ended CatheterJunkNo ratings yet
- Central VC ModuleDocument11 pagesCentral VC ModuleJunkNo ratings yet
- MU Manual 2 PDFDocument35 pagesMU Manual 2 PDFBasma AzazNo ratings yet
- Adverse Effects Of: Blood TransfusionDocument44 pagesAdverse Effects Of: Blood TransfusionNadir A IbrahimNo ratings yet
- Cystoclysis / Continuous Bladder Irrigation (Cbi) : Skills Laboratory Module No. 25Document4 pagesCystoclysis / Continuous Bladder Irrigation (Cbi) : Skills Laboratory Module No. 25astraeax pandaNo ratings yet
- RFDS Western Operations HEA16 - V3.0 Clinical ManualDocument28 pagesRFDS Western Operations HEA16 - V3.0 Clinical ManualJoed BiasonNo ratings yet
- 2016 NUR1021 Calculation of Basic IV Drip Rates - InstructorDocument39 pages2016 NUR1021 Calculation of Basic IV Drip Rates - InstructorMikhaelEarlSantosTacorda100% (1)
- PPH SetDocument1 pagePPH Setgeorgeloto12100% (1)
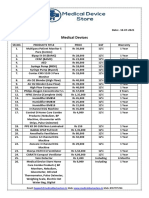
- Medical Device Store Products CatalogueDocument3 pagesMedical Device Store Products CatalogueWasim KhatibNo ratings yet
- Atosiban-5ml InfusionDocument5 pagesAtosiban-5ml InfusionMd. Abdur RahmanNo ratings yet
- Practice Drug CalculationsDocument11 pagesPractice Drug Calculationskijeramustapha23No ratings yet
- BD Alaris Plus Transfer Tool DFU BDDF00494 enDocument18 pagesBD Alaris Plus Transfer Tool DFU BDDF00494 enWaleed Ah-DhaifiNo ratings yet
- Liste Des Prix Consommables Médicaux 02 2019Document18 pagesListe Des Prix Consommables Médicaux 02 2019Racem LoukilNo ratings yet
- FINAL - Changes - NURS 401 Medication Safety and Calculation Quiz Information - 2Document12 pagesFINAL - Changes - NURS 401 Medication Safety and Calculation Quiz Information - 2guneet cheema0% (1)
- Podesta Military Tribunal Day Two - 4 May 2021Document3 pagesPodesta Military Tribunal Day Two - 4 May 2021Ronald Wederfoort100% (5)
- CL Midterm Oxytocin AdminDocument2 pagesCL Midterm Oxytocin AdminkristiannedenNo ratings yet
- Avoid Confusion On Infusions! Infusion and Injection Coding Tips and TricksDocument19 pagesAvoid Confusion On Infusions! Infusion and Injection Coding Tips and TrickssupercoderNo ratings yet
- Equator MANTA TERMICA PDFDocument68 pagesEquator MANTA TERMICA PDFAnonymous MnaMZQWwCNo ratings yet
- Nursing Foundation Harinderjeet GoyalDocument31 pagesNursing Foundation Harinderjeet Goyalmanrajghumman5550% (1)
- Transportation of The Critically Ill Patient 1Document17 pagesTransportation of The Critically Ill Patient 1Foo Wing JianNo ratings yet
- лекция 8 Phlegmon of the floor of the mouth. Topographic anatomy of the floor of the mouth, sources of infection, possible ways of spreading the infection. Clinic, differential diagnostics. Surgery. PDocument41 pagesлекция 8 Phlegmon of the floor of the mouth. Topographic anatomy of the floor of the mouth, sources of infection, possible ways of spreading the infection. Clinic, differential diagnostics. Surgery. Ptalalelsherif92No ratings yet
- Pembimbing: Dr. Emon Winardi, Sp. PDDocument37 pagesPembimbing: Dr. Emon Winardi, Sp. PDJericoKelvinNo ratings yet
- Potassium Chloride in Sodium ChlorideDocument3 pagesPotassium Chloride in Sodium Chlorideirma_rahayu_2No ratings yet
- Fluid Balance in Bowel ObstructionDocument7 pagesFluid Balance in Bowel Obstructiongodeberta18No ratings yet
- Medical Devices PDFDocument38 pagesMedical Devices PDFDr D Alwin , VetNo ratings yet
- What Is Obstructive JaundiceDocument1 pageWhat Is Obstructive JaundiceNicole PramonoNo ratings yet
- ERAS Ward Protocol in EnglishDocument4 pagesERAS Ward Protocol in EnglishfithriNo ratings yet























































































Download as docx, pdf, or txt
You might also like
- Andre Tan's Surgical NotesDocument163 pagesAndre Tan's Surgical NotesHani Nadiah75% (4)
- Fundamentals NotesDocument23 pagesFundamentals NotesElle R Naceno100% (5)
- 2019 Book VesselHealthAndPreservationTheDocument303 pages2019 Book VesselHealthAndPreservationTheOigres OdaravalNo ratings yet
- Osce - D&CDocument2 pagesOsce - D&Cmkct111No ratings yet
- Obs Gynae Full Summary NotesDocument41 pagesObs Gynae Full Summary NotesJana Aldour100% (1)
- Medication Calculation Practice Problems: Level Ii, Iii and IvDocument6 pagesMedication Calculation Practice Problems: Level Ii, Iii and IvQueennita100% (7)
- Operating Manual Infusomat Space PDFDocument82 pagesOperating Manual Infusomat Space PDFamirali.bme4527No ratings yet
- Pediatric Nursing An Introductory Text 11th Edition Price Test BankDocument11 pagesPediatric Nursing An Introductory Text 11th Edition Price Test BankDarius67% (3)
- Percutaneous Non-TunneledDocument12 pagesPercutaneous Non-TunneledJunkNo ratings yet
- Implanted Venous Access Device (IVAD) - "Dome" or "Port"Document12 pagesImplanted Venous Access Device (IVAD) - "Dome" or "Port"JunkNo ratings yet
- Percutaneous Non-Tunneled Open-Ended CatheterDocument13 pagesPercutaneous Non-Tunneled Open-Ended CatheterJunkNo ratings yet
- Central VC ModuleDocument11 pagesCentral VC ModuleJunkNo ratings yet
- 20 Trauma Resuscitation Part 2 InterventionsDocument3 pages20 Trauma Resuscitation Part 2 InterventionssueNo ratings yet
- S T A R T: Imple Riage ND Apid ReatmentDocument17 pagesS T A R T: Imple Riage ND Apid ReatmentNavine NavNo ratings yet
- Anaesthesia SummaryDocument36 pagesAnaesthesia SummaryRazan QassemNo ratings yet
- Advanced Life Support: Siska Christianingsih, S.Kep.,Ns.M.KepDocument31 pagesAdvanced Life Support: Siska Christianingsih, S.Kep.,Ns.M.KepFlorenciaNo ratings yet
- Advanced Trauma Life Support RevisedDocument7 pagesAdvanced Trauma Life Support RevisedpaveethrahNo ratings yet
- DR - Noer Rachmat Early Management Pelvic FractureDocument72 pagesDR - Noer Rachmat Early Management Pelvic FractureRsud Malinau Ppk BludNo ratings yet
- Diagnostic Procedures For Respiratory Conditions Non-Invasive & Invasive ProceduresDocument4 pagesDiagnostic Procedures For Respiratory Conditions Non-Invasive & Invasive ProceduresIrish Eunice FelixNo ratings yet
- Cme Trauma Management ZakwanDocument44 pagesCme Trauma Management ZakwansyasyaNo ratings yet
- Airway ManagementDocument4 pagesAirway ManagementEllamae DerupeNo ratings yet
- Primary and Secondary Survey MiraDocument50 pagesPrimary and Secondary Survey MiraAfifah SelamatNo ratings yet
- Emergency Medicine: by DR Maimun ShikderDocument22 pagesEmergency Medicine: by DR Maimun ShikderFarwa RazaNo ratings yet
- TM 5-6 - Musculosceletal CT - P. JeffryDocument50 pagesTM 5-6 - Musculosceletal CT - P. Jeffryradiologi.rsgmNo ratings yet
- Tugas Anestesi Rani RevisiDocument27 pagesTugas Anestesi Rani RevisiFahrizalNo ratings yet
- Basic Chest UltrasoundDocument60 pagesBasic Chest UltrasoundAdriana Villarreal100% (2)
- Review NotesDocument5 pagesReview NotesIrish May BalanzaNo ratings yet
- Advanced Trauma Life SupportDocument8 pagesAdvanced Trauma Life SupportAbouzr Mohammed ElsaidNo ratings yet
- General Management of Trauma: The Atls ConceptDocument30 pagesGeneral Management of Trauma: The Atls ConceptWasim R. IssaNo ratings yet
- Airway Control Management, RSPMDocument59 pagesAirway Control Management, RSPMzakia4nisakNo ratings yet
- Airway Control Management, RSPMDocument59 pagesAirway Control Management, RSPMEryanda DinataNo ratings yet
- Approach To TraumaDocument43 pagesApproach To TraumaAlmonz AndoriasNo ratings yet
- 2.1. Trauma and Critical Care (Jerome Villacorta's Conflicted Copy 2013-08-24)Document12 pages2.1. Trauma and Critical Care (Jerome Villacorta's Conflicted Copy 2013-08-24)Miguel C. DolotNo ratings yet
- Trauma Resuscitation Acute Care Emerg MedDocument67 pagesTrauma Resuscitation Acute Care Emerg MedsyasyaNo ratings yet
- Perioperative NursingDocument5 pagesPerioperative NursingMikhaela Andree MarianoNo ratings yet
- Laminectomy: By: RN Nurul Syazwani RosliDocument26 pagesLaminectomy: By: RN Nurul Syazwani RosliMuhammad Nizam AmmNo ratings yet
- 3 Ways To Examine The Larynx: PiriformDocument10 pages3 Ways To Examine The Larynx: PiriformbeautyNo ratings yet
- Pulse OximetryDocument7 pagesPulse OximetryEmerson De SilvaNo ratings yet
- CVS Phsicl ExaminationDocument34 pagesCVS Phsicl ExaminationHassan HarirNo ratings yet
- 2.1. Trauma and Critical CareDocument13 pages2.1. Trauma and Critical CareMiguel C. DolotNo ratings yet
- Radiology Lecture 4th Year 2022 Part 2Document44 pagesRadiology Lecture 4th Year 2022 Part 2Abubakar JallohNo ratings yet
- DR Sujata: Professor Dept - of Anaesthesiology &critical Care Ucms & GTB HospitalDocument53 pagesDR Sujata: Professor Dept - of Anaesthesiology &critical Care Ucms & GTB HospitalMiniNo ratings yet
- SpineDocument83 pagesSpineMohamed Ragab 3mmarNo ratings yet
- Common Musculoskeletal ProblemsDocument17 pagesCommon Musculoskeletal Problemsapi-3822433No ratings yet
- Prevention of Postoperative Complications of CDocument1 pagePrevention of Postoperative Complications of CChinedu H. DuruNo ratings yet
- Gallery Walk PosterDocument1 pageGallery Walk PosterBern NerquitNo ratings yet
- Anesthesia PositionsDocument19 pagesAnesthesia Positionsnicolinna2000yahoo.comNo ratings yet
- Nursing Intervention Respiratory Status: Ventilation Respiratory Status: Airway Patency Vital Sign StatusDocument12 pagesNursing Intervention Respiratory Status: Ventilation Respiratory Status: Airway Patency Vital Sign StatusSepti MemorisaNo ratings yet
- EM - SGD 1 (Airway and Breathing)Document5 pagesEM - SGD 1 (Airway and Breathing)R RNo ratings yet
- General Anesthesia Notes - JalaDocument6 pagesGeneral Anesthesia Notes - JalaJulie Anne AciertoNo ratings yet
- Approach To Trauma PatientsDocument45 pagesApproach To Trauma PatientsSarahNo ratings yet
- Positioning Patients in BedDocument27 pagesPositioning Patients in BedAldo BGamanNo ratings yet
- Respiratory Paediatrics ExaminationDocument1 pageRespiratory Paediatrics ExaminationRatnahKumar28No ratings yet
- RSI Assessment HODocument4 pagesRSI Assessment HOlalalalalalalalalala happinessNo ratings yet
- Surgery Emergencies: Multiple Trauma: Yonathan Adi PurnomoDocument66 pagesSurgery Emergencies: Multiple Trauma: Yonathan Adi Purnomowaraney palitNo ratings yet
- Airway ManagementDocument129 pagesAirway ManagementSyabie YassinNo ratings yet
- (Mantap) Slide Materi Anestesi Batch 3 2018Document74 pages(Mantap) Slide Materi Anestesi Batch 3 2018Aditya PratamaNo ratings yet
- Respiratory Syatem: January 2009Document19 pagesRespiratory Syatem: January 2009aarti devNo ratings yet
- Airway Managmenat Normal and DifficultDocument49 pagesAirway Managmenat Normal and DifficultHari Om ChaurasiyaNo ratings yet
- WSDDocument50 pagesWSDgraceriaaNo ratings yet
- Eyes To KnowDocument3 pagesEyes To KnowTrisNo ratings yet
- Chest Radiography For InternsDocument42 pagesChest Radiography For InternsRose ValeNo ratings yet
- Cvs ExaminationDocument2 pagesCvs Examinationjenny grovesNo ratings yet
- Implanted Venous Access Device (IVAD) - "Dome" or "Port"Document12 pagesImplanted Venous Access Device (IVAD) - "Dome" or "Port"JunkNo ratings yet
- Percutaneous Non-TunneledDocument12 pagesPercutaneous Non-TunneledJunkNo ratings yet
- Percutaneous Non-Tunneled Open-Ended CatheterDocument13 pagesPercutaneous Non-Tunneled Open-Ended CatheterJunkNo ratings yet
- Central VC ModuleDocument11 pagesCentral VC ModuleJunkNo ratings yet
- MU Manual 2 PDFDocument35 pagesMU Manual 2 PDFBasma AzazNo ratings yet
- Adverse Effects Of: Blood TransfusionDocument44 pagesAdverse Effects Of: Blood TransfusionNadir A IbrahimNo ratings yet
- Cystoclysis / Continuous Bladder Irrigation (Cbi) : Skills Laboratory Module No. 25Document4 pagesCystoclysis / Continuous Bladder Irrigation (Cbi) : Skills Laboratory Module No. 25astraeax pandaNo ratings yet
- RFDS Western Operations HEA16 - V3.0 Clinical ManualDocument28 pagesRFDS Western Operations HEA16 - V3.0 Clinical ManualJoed BiasonNo ratings yet
- 2016 NUR1021 Calculation of Basic IV Drip Rates - InstructorDocument39 pages2016 NUR1021 Calculation of Basic IV Drip Rates - InstructorMikhaelEarlSantosTacorda100% (1)
- PPH SetDocument1 pagePPH Setgeorgeloto12100% (1)
- Medical Device Store Products CatalogueDocument3 pagesMedical Device Store Products CatalogueWasim KhatibNo ratings yet
- Atosiban-5ml InfusionDocument5 pagesAtosiban-5ml InfusionMd. Abdur RahmanNo ratings yet
- Practice Drug CalculationsDocument11 pagesPractice Drug Calculationskijeramustapha23No ratings yet
- BD Alaris Plus Transfer Tool DFU BDDF00494 enDocument18 pagesBD Alaris Plus Transfer Tool DFU BDDF00494 enWaleed Ah-DhaifiNo ratings yet
- Liste Des Prix Consommables Médicaux 02 2019Document18 pagesListe Des Prix Consommables Médicaux 02 2019Racem LoukilNo ratings yet
- FINAL - Changes - NURS 401 Medication Safety and Calculation Quiz Information - 2Document12 pagesFINAL - Changes - NURS 401 Medication Safety and Calculation Quiz Information - 2guneet cheema0% (1)
- Podesta Military Tribunal Day Two - 4 May 2021Document3 pagesPodesta Military Tribunal Day Two - 4 May 2021Ronald Wederfoort100% (5)
- CL Midterm Oxytocin AdminDocument2 pagesCL Midterm Oxytocin AdminkristiannedenNo ratings yet
- Avoid Confusion On Infusions! Infusion and Injection Coding Tips and TricksDocument19 pagesAvoid Confusion On Infusions! Infusion and Injection Coding Tips and TrickssupercoderNo ratings yet
- Equator MANTA TERMICA PDFDocument68 pagesEquator MANTA TERMICA PDFAnonymous MnaMZQWwCNo ratings yet
- Nursing Foundation Harinderjeet GoyalDocument31 pagesNursing Foundation Harinderjeet Goyalmanrajghumman5550% (1)
- Transportation of The Critically Ill Patient 1Document17 pagesTransportation of The Critically Ill Patient 1Foo Wing JianNo ratings yet
- лекция 8 Phlegmon of the floor of the mouth. Topographic anatomy of the floor of the mouth, sources of infection, possible ways of spreading the infection. Clinic, differential diagnostics. Surgery. PDocument41 pagesлекция 8 Phlegmon of the floor of the mouth. Topographic anatomy of the floor of the mouth, sources of infection, possible ways of spreading the infection. Clinic, differential diagnostics. Surgery. Ptalalelsherif92No ratings yet
- Pembimbing: Dr. Emon Winardi, Sp. PDDocument37 pagesPembimbing: Dr. Emon Winardi, Sp. PDJericoKelvinNo ratings yet
- Potassium Chloride in Sodium ChlorideDocument3 pagesPotassium Chloride in Sodium Chlorideirma_rahayu_2No ratings yet
- Fluid Balance in Bowel ObstructionDocument7 pagesFluid Balance in Bowel Obstructiongodeberta18No ratings yet
- Medical Devices PDFDocument38 pagesMedical Devices PDFDr D Alwin , VetNo ratings yet
- What Is Obstructive JaundiceDocument1 pageWhat Is Obstructive JaundiceNicole PramonoNo ratings yet
- ERAS Ward Protocol in EnglishDocument4 pagesERAS Ward Protocol in EnglishfithriNo ratings yet