Download as docx, pdf, or txt
You might also like
- Method Statement - Relocation of Water MeterDocument5 pagesMethod Statement - Relocation of Water MeterMG50% (2)
- Old Yang Tai Chi Edition OfferDocument23 pagesOld Yang Tai Chi Edition Offerdimmo100% (1)
- Patient Encounter FormDocument2 pagesPatient Encounter FormSpectator Medic0% (1)
- Med Cert DepedDocument1 pageMed Cert DepedMark Cañete PunongbayanNo ratings yet
- Discharge Plan FormatDocument2 pagesDischarge Plan FormatChristian67% (6)
- FatigueDocument3 pagesFatigueIande CornerNo ratings yet
- Endorsement SheetDocument1 pageEndorsement SheetMon DoceNo ratings yet
- Clinical Pathway For Hypertensive Urgency (Revised)Document6 pagesClinical Pathway For Hypertensive Urgency (Revised)Heide Danica A. BaltazarNo ratings yet
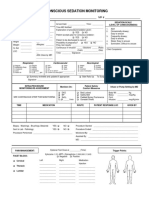
- 34 An Consious Sedation MonitoringDocument2 pages34 An Consious Sedation Monitoringabu alauon abed almohsenNo ratings yet
- Procedural Sedation RecordDocument2 pagesProcedural Sedation RecordRosanne AguilarNo ratings yet
- Anadjah Ebrahim MCDocument1 pageAnadjah Ebrahim MCMusaiden EbrahimNo ratings yet
- Rle WorksheetDocument8 pagesRle WorksheetLiza AingelicaNo ratings yet
- Rle WorksheetDocument9 pagesRle WorksheetLiza AingelicaNo ratings yet
- Report Sheet - NursingDocument1 pageReport Sheet - NursingMario LemirNo ratings yet
- Patient Chart TemplateDocument3 pagesPatient Chart TemplateV NNo ratings yet
- Dokumentasi Pada Tatanan KhususDocument7 pagesDokumentasi Pada Tatanan KhususyohannaNo ratings yet
- Medical ClinicDocument1 pageMedical ClinicAngelica Branzuela Pagal AninipotNo ratings yet
- Aor Reporting FormDocument2 pagesAor Reporting FormPaidiHasanNo ratings yet
- Hso G Medical Examination FormDocument1 pageHso G Medical Examination FormorionsrulerNo ratings yet
- Drug Study 3Document1 pageDrug Study 3Coleen Angelique MontenegroNo ratings yet
- AUC Health ClearanceDocument2 pagesAUC Health ClearanceNatasha ReddyNo ratings yet
- Obstetric Assessment ToolDocument5 pagesObstetric Assessment ToolDudil GoatNo ratings yet
- NCM 107 Rle: Indication of Use) : Name, Dose, Timing, Route Indication ObjectiveDocument5 pagesNCM 107 Rle: Indication of Use) : Name, Dose, Timing, Route Indication ObjectiveDud AccNo ratings yet
- (HSO) Medical Examination FormDocument1 page(HSO) Medical Examination FormKrizel LagundiNo ratings yet
- Circulating Case Slip: Name of Student Student NumberDocument12 pagesCirculating Case Slip: Name of Student Student NumberEugenio Roque Casaclang De Leon IiiNo ratings yet
- REFERRALDocument1 pageREFERRALNether MonsterNo ratings yet
- Annual Medical ReportDocument6 pagesAnnual Medical ReportMarc SilvestreNo ratings yet
- Cuidados Posoperatorio CirugiaDocument1 pageCuidados Posoperatorio CirugiaAna CristernaNo ratings yet
- Sedation Record: Patient Selection Criteria DateDocument2 pagesSedation Record: Patient Selection Criteria Datenona aryanNo ratings yet
- OSHS Annual Medical ReportDocument6 pagesOSHS Annual Medical ReportRandy PedrozaNo ratings yet
- Annual Medical Report - 2022Document8 pagesAnnual Medical Report - 2022KokieNo ratings yet
- Clinic 5Document1 pageClinic 5nandyanuaNo ratings yet
- Organizational WorksheetDocument4 pagesOrganizational WorksheetJennifer AprilNo ratings yet
- Mini TicklerDocument1 pageMini TicklerTrisha Mae MacatangayNo ratings yet
- Circumcision 2-4-09Document2 pagesCircumcision 2-4-09twells417No ratings yet
- 2018 WSRDocument1 page2018 WSR2ncnz6999mNo ratings yet
- Annual Medical Report Form PDFDocument8 pagesAnnual Medical Report Form PDFDaniel ReyesNo ratings yet
- CaseloadDocument3 pagesCaseloadJayson Mherl GonzalesNo ratings yet
- New Referral Form Sheet1Document2 pagesNew Referral Form Sheet1rebklineNo ratings yet
- Billing Account FormDocument1 pageBilling Account FormGubat District HospitalNo ratings yet
- Companion Animal FormDocument2 pagesCompanion Animal FormGabriela GuerraNo ratings yet
- RRT FormDocument1 pageRRT Formjepa kripaNo ratings yet
- NURS 4045 Adult Health Competencies II Texas Woman's University Patient Data SheetDocument12 pagesNURS 4045 Adult Health Competencies II Texas Woman's University Patient Data SheetUyen DoNo ratings yet
- ISO 05 Student Health Record 1 RevDocument2 pagesISO 05 Student Health Record 1 RevHahaha HihihooNo ratings yet
- Pediatric History OutlineDocument12 pagesPediatric History OutlineDawn MarcoNo ratings yet
- 4.operating Room RecordDocument1 page4.operating Room RecordDienizs LabiniNo ratings yet
- Bedside Shift ReportDocument3 pagesBedside Shift ReportRumkee chyNo ratings yet
- History Guide Ob GyneDocument5 pagesHistory Guide Ob Gyned99452727No ratings yet
- AmrDocument5 pagesAmrGemarie Adarlo CastilloNo ratings yet
- Template For Clinical Progress Note June 2009Document3 pagesTemplate For Clinical Progress Note June 2009Buthaina AltenaijiNo ratings yet
- Pedi Admission OrdersDocument1 pagePedi Admission OrdersRyan Bianet CosicolNo ratings yet
- Night BeforeDocument3 pagesNight BeforeChris MoffettNo ratings yet
- MED-F-009 Discharge Planning FormDocument1 pageMED-F-009 Discharge Planning Formdrakmalik71No ratings yet
- Geriatric Case KitDocument6 pagesGeriatric Case KitMay Chelle ErazoNo ratings yet
- CONSENT PROCEDURE - English - Oct2016Document2 pagesCONSENT PROCEDURE - English - Oct2016malaysiamadani01No ratings yet
- Headaches Residual Functional Capacity QuestionnaireDocument3 pagesHeadaches Residual Functional Capacity QuestionnaireDellComputer99No ratings yet
- FAB - Annual Medical Report FormDocument8 pagesFAB - Annual Medical Report FormOsfmc LogisticsNo ratings yet
- WM 03092011Document15 pagesWM 03092011Sbc GradNo ratings yet
- B0146 CashlessDocument1 pageB0146 CashlessSubhajit BhoiNo ratings yet
- Governmental Traumatizing Investigations: An Application to Get a New Toilet, Part IFrom EverandGovernmental Traumatizing Investigations: An Application to Get a New Toilet, Part INo ratings yet
- CDI3 Module 12Document8 pagesCDI3 Module 12Ysabela Kim Raz CarboNo ratings yet
- ArrestDocument40 pagesArrestYsabela Kim Raz CarboNo ratings yet
- Crs4 - Professional Conduct and Ethical IssuesDocument31 pagesCrs4 - Professional Conduct and Ethical IssuesYsabela Kim Raz CarboNo ratings yet
- Lesson 1 Legal Bases of Industrial Security ManagementDocument15 pagesLesson 1 Legal Bases of Industrial Security ManagementYsabela Kim Raz CarboNo ratings yet
- Accounting Cycle of A Merchandising BusinessDocument32 pagesAccounting Cycle of A Merchandising BusinessYsabela Kim Raz CarboNo ratings yet
- Depression: by Aroosha Abdul RasheedDocument9 pagesDepression: by Aroosha Abdul RasheedArushar 24No ratings yet
- Case Study StabDocument7 pagesCase Study StabMari Jasmeen Estrada Noveda100% (1)
- Illness PerceptionDocument13 pagesIllness PerceptionhakrajputNo ratings yet
- My Philosophy of Nursing OutlineDocument8 pagesMy Philosophy of Nursing Outlineapi-340667135No ratings yet
- Safety Training FormatsDocument11 pagesSafety Training FormatsAsan IbrahimNo ratings yet
- Concept PaperDocument2 pagesConcept PaperDavid Lee100% (13)
- 38 Feam Ejb EngDocument4 pages38 Feam Ejb EngSaufi YatimNo ratings yet
- Stock 01 Des 22Document70 pagesStock 01 Des 22kaprodiS1 stikesalfatahNo ratings yet
- Educating The Nurses of 2025 Technology Trends of 2017 Nurse Education in PDocument4 pagesEducating The Nurses of 2025 Technology Trends of 2017 Nurse Education in Pfriska anjaNo ratings yet
- Pleural Fluid Analysis, Thoracentesis, Biopsy, and Chest TubeDocument6 pagesPleural Fluid Analysis, Thoracentesis, Biopsy, and Chest TubeRicky SpideyNo ratings yet
- Guidelines CANALL5SASDocument29 pagesGuidelines CANALL5SASNil PaksnavinNo ratings yet
- Practice Guidelines For Tumor Marker Use in The Clinic: Catharine SturgeonDocument9 pagesPractice Guidelines For Tumor Marker Use in The Clinic: Catharine SturgeonYder AtrupNo ratings yet
- Ear Surgery: Tympanoplasty, Mastoidectomy: Patient Postoperative Instructions and InformationDocument4 pagesEar Surgery: Tympanoplasty, Mastoidectomy: Patient Postoperative Instructions and InformationPaul Jordan SandaloNo ratings yet
- Chapter 038Document51 pagesChapter 038Ako To100% (1)
- Tiong Bi v. PhilhealthDocument7 pagesTiong Bi v. PhilhealthRodney AtibulaNo ratings yet
- Transforming Research Into ActionDocument48 pagesTransforming Research Into ActionGustavo FonsecaNo ratings yet
- Workload Indicators (Staffing Norms)Document131 pagesWorkload Indicators (Staffing Norms)asimsiNo ratings yet
- A Comprehensive: Health Analysis ReportDocument20 pagesA Comprehensive: Health Analysis ReportAbhilash MishraNo ratings yet
- THE INDEPENDENT Issue 542 PDFDocument44 pagesTHE INDEPENDENT Issue 542 PDFThe Independent MagazineNo ratings yet
- MCQ Construction SafetyDocument18 pagesMCQ Construction SafetyGautam PrajapatiNo ratings yet
- Chapter 3Document2 pagesChapter 3Laramy Lacy MontgomeryNo ratings yet
- 2019 CPC Chapter 16 PA Tips FAQs - CyDocument4 pages2019 CPC Chapter 16 PA Tips FAQs - CyAnthony El HageNo ratings yet
- Financial GuaranteeDocument2 pagesFinancial Guaranteeapi-19509948No ratings yet
- Hindustan Times Delhi 21 - 6Document44 pagesHindustan Times Delhi 21 - 6Hmbe hmbeNo ratings yet
- Attunement and Involvement (PDFDrive)Document27 pagesAttunement and Involvement (PDFDrive)Dangsinen SarangheyoNo ratings yet
- National Privacy Commission: Republic Act 10173 - Data Privacy Act of 2012Document21 pagesNational Privacy Commission: Republic Act 10173 - Data Privacy Act of 2012enber.franciscoNo ratings yet
- Final FS Balachan DipDocument121 pagesFinal FS Balachan DipRosemarie VeluzNo ratings yet