
Parkinson's Disease: March 2018
Parkinson's Disease: March 2018
You might also like
- Yamaha Fazer-Fzh150 CatalogueDocument55 pagesYamaha Fazer-Fzh150 CatalogueAnonymous KoA00wXXD69% (13)
- ptj4008504 PDFDocument8 pagesptj4008504 PDFDiva VashtiNo ratings yet
- Phytotherapy in Treatment of Parkinson's Disease: A Review: Pharmaceutical BiologyDocument9 pagesPhytotherapy in Treatment of Parkinson's Disease: A Review: Pharmaceutical BiologyG. Araya MoraNo ratings yet
- Parkinson's DiseaseDocument14 pagesParkinson's DiseaseRohan MistryNo ratings yet
- Altered Oxidative Stress Levels in Indian Parkinson's Disease Patients With PARK2 MutationsDocument5 pagesAltered Oxidative Stress Levels in Indian Parkinson's Disease Patients With PARK2 MutationssandykumalaNo ratings yet
- Toneuj 10 42 PDFDocument17 pagesToneuj 10 42 PDFpratiwifatmasariNo ratings yet
- Latest Progresses and Methods Used To Treat Parkinson's DiseaseDocument9 pagesLatest Progresses and Methods Used To Treat Parkinson's DiseaseInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Parkinson's Disease: Mechanisms, Translational Models and Management StrategiesDocument14 pagesParkinson's Disease: Mechanisms, Translational Models and Management StrategiesGleyce CabralNo ratings yet
- Science:, 819 (2003) Ted M. Dawson and Valina L. DawsonDocument5 pagesScience:, 819 (2003) Ted M. Dawson and Valina L. DawsonSomanshu BanerjeeNo ratings yet
- TMP - 4306 300 596 1 SM (3) 1791561448Document5 pagesTMP - 4306 300 596 1 SM (3) 1791561448Lulu LuwiiNo ratings yet
- Effect of Walking Along Circle On Foot Prints in Parkinson's On FreezingDocument48 pagesEffect of Walking Along Circle On Foot Prints in Parkinson's On FreezingAnup ShankarwarNo ratings yet
- Parkinsonism A General Motor Disability PDFDocument9 pagesParkinsonism A General Motor Disability PDFRishabh SinghNo ratings yet
- Parkinson's: A Syndrome Rather Than A Disease?: BackgroundDocument8 pagesParkinson's: A Syndrome Rather Than A Disease?: BackgroundEduardo Santana SuárezNo ratings yet
- Review (1) - 2004 - Tabakmna Et AlDocument11 pagesReview (1) - 2004 - Tabakmna Et Alshimonl3892No ratings yet
- Stem Cell-Based Therapies For Parkinson DiseaseDocument17 pagesStem Cell-Based Therapies For Parkinson DiseaseYunita Christiani BiyangNo ratings yet
- PARKINSONISMDocument5 pagesPARKINSONISMPrashanth RajuNo ratings yet
- WJPR Shivaleela Rev ArticleDocument26 pagesWJPR Shivaleela Rev ArticlerajeshNo ratings yet
- Parkinson's Disease: From Bench To BedsideDocument17 pagesParkinson's Disease: From Bench To BedsideSoap 2221No ratings yet
- Involvement of Interferon-Dopaminergic Neurons: in Microglial-Mediated Loss ofDocument10 pagesInvolvement of Interferon-Dopaminergic Neurons: in Microglial-Mediated Loss ofshayley9No ratings yet
- Parkinson and Stem Cell TherapyDocument9 pagesParkinson and Stem Cell TherapyLefinia PutriNo ratings yet
- Evaluation of Anti-Parkinson'sDocument80 pagesEvaluation of Anti-Parkinson'sPanini PatankarNo ratings yet
- TMP FFC1Document28 pagesTMP FFC1FrontiersNo ratings yet
- Biology of Parkinson S Disease Pathogenesis and Pathophysiology of A Multisystem Neurodegenerative DisorderDocument23 pagesBiology of Parkinson S Disease Pathogenesis and Pathophysiology of A Multisystem Neurodegenerative DisorderNelly LeónNo ratings yet
- AANA Journal Course: Update For Nurse Anesthetists Parkinson DiseaseDocument6 pagesAANA Journal Course: Update For Nurse Anesthetists Parkinson DiseaseMarianne GarciaNo ratings yet
- Pharmaceutics 15 00770Document24 pagesPharmaceutics 15 00770Estefania AndreaNo ratings yet
- Parkinsons Disease Recent Advancement and Future AspectsDocument20 pagesParkinsons Disease Recent Advancement and Future AspectsIJRASETPublicationsNo ratings yet
- The Role of Insulin Igf-1Document8 pagesThe Role of Insulin Igf-1Arina Windri RivartiNo ratings yet
- Etiology and Pathophysiology of Parkinson S DiseaseDocument552 pagesEtiology and Pathophysiology of Parkinson S DiseaseAstrid Figueroa100% (2)
- CORTEX PDreviewDocument8 pagesCORTEX PDreviewNadineNo ratings yet
- Manuscript 3Document16 pagesManuscript 3Nana ShkodinaNo ratings yet
- PARKINSONDocument59 pagesPARKINSONvannyNo ratings yet
- BDDKPDocument21 pagesBDDKPChidube UkachukwuNo ratings yet
- Mitochondrial Dysfunction and Mitophagy in Parkinson's: From Familial To Sporadic DiseaseDocument11 pagesMitochondrial Dysfunction and Mitophagy in Parkinson's: From Familial To Sporadic DiseaseKaycsa AdrianaNo ratings yet
- Experimental Validation of Vitex Negundo Leaves Hydroalcoholic Extract For Neuroprotection in Haloperidol Induced Parkinson's Disease in RatDocument16 pagesExperimental Validation of Vitex Negundo Leaves Hydroalcoholic Extract For Neuroprotection in Haloperidol Induced Parkinson's Disease in Ratali abbas rizviNo ratings yet
- Herbal Treatment of Parkinsonism A ReviewDocument7 pagesHerbal Treatment of Parkinsonism A ReviewKartika BorraNo ratings yet
- Background Parkinson Disease Is Recognized As One of The Most Common Neurologic Disorders, AffectingDocument27 pagesBackground Parkinson Disease Is Recognized As One of The Most Common Neurologic Disorders, AffectingCharan Pal SinghNo ratings yet
- The Development of Treatment For Parkinson's Disease: Harishankar Prasad Yadav, Yun LiDocument20 pagesThe Development of Treatment For Parkinson's Disease: Harishankar Prasad Yadav, Yun LiTherezia Sonia Gabriella TanggulunganNo ratings yet
- Spektro Uv VisDocument7 pagesSpektro Uv VisNadaNo ratings yet
- Parkinson's DiseaseDocument9 pagesParkinson's Diseaselucia desantisNo ratings yet
- 1 s2.0 S016517811530559X MainDocument6 pages1 s2.0 S016517811530559X MainDiana DionisioNo ratings yet
- Neurochemistry International: Sunaina Sharma, Puneet Kumar, Rahul DeshmukhDocument8 pagesNeurochemistry International: Sunaina Sharma, Puneet Kumar, Rahul DeshmukhEla MishraNo ratings yet
- 2019 European Academy of Neurology Parkinson DiseaseDocument16 pages2019 European Academy of Neurology Parkinson DiseaseJuan Diego Gutierrez ZevallosNo ratings yet
- The Parkinson Disease Mitochondrial Hypothesis: Where Are We At?Document12 pagesThe Parkinson Disease Mitochondrial Hypothesis: Where Are We At?just for download matterNo ratings yet
- Parkinson's Disease: A Review: Neurology India March 2018Document11 pagesParkinson's Disease: A Review: Neurology India March 2018Alina Vitali TabarceaNo ratings yet
- Parkinson ThesisDocument4 pagesParkinson Thesisandreajimenezomaha100% (1)
- Ijn 5 3 95 1051Document12 pagesIjn 5 3 95 1051Riris AriskaNo ratings yet
- Role of Encapsulated Nano Curcumin in Induced Sh-Sy-5y Cell LineDocument8 pagesRole of Encapsulated Nano Curcumin in Induced Sh-Sy-5y Cell LineInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Jurnal NeuropsikiatriDocument10 pagesJurnal NeuropsikiatriPosterilmiah Majestynas2019No ratings yet
- Haloperidol Dose and Effect of ParkinsonDocument13 pagesHaloperidol Dose and Effect of Parkinsonali abbas rizviNo ratings yet
- Peerj 16762Document21 pagesPeerj 16762jamesraiaanNo ratings yet
- Mitochondrial Pyruvate Carrier Regulates Autophagy, in Ammation, and Neurodegeneration in Experimental Models of Parkinsons DiseaseDocument51 pagesMitochondrial Pyruvate Carrier Regulates Autophagy, in Ammation, and Neurodegeneration in Experimental Models of Parkinsons DiseaseEkeleme Nnamdi MartinsNo ratings yet
- Epidemiology PAthology Genetics and PathophysiologyDocument15 pagesEpidemiology PAthology Genetics and PathophysiologybbadoNo ratings yet
- Https Emedicine - Medscape.com Article 1831191-PrintDocument59 pagesHttps Emedicine - Medscape.com Article 1831191-PrintNoviatiPrayangsariNo ratings yet
- The Genes of Parkinson's DiseaseDocument6 pagesThe Genes of Parkinson's Diseaseapi-26116142No ratings yet
- Pharmacogenetics of Antipsychotic-Induced Movement Disorders As A Resource For Better Understanding Parkinson's Disease Modifier GenesDocument9 pagesPharmacogenetics of Antipsychotic-Induced Movement Disorders As A Resource For Better Understanding Parkinson's Disease Modifier Genesel egendNo ratings yet
- Artículo de GeriatríaDocument14 pagesArtículo de GeriatríaMaria Guadalupe Hernandez JimenezNo ratings yet
- Fifty Years of Clinical Holistic Treatment for Parkinson’s: A Unique ApproachFrom EverandFifty Years of Clinical Holistic Treatment for Parkinson’s: A Unique ApproachRating: 1 out of 5 stars1/5 (1)
- DJ1 PD Review 2021Document8 pagesDJ1 PD Review 2021Krisztina TothNo ratings yet
- Parkinson's Disease A Review 2014 PDFDocument19 pagesParkinson's Disease A Review 2014 PDFjeanNo ratings yet
- Human Caspases and Neuronal Apoptosis in Neurodegenerative DiseasesFrom EverandHuman Caspases and Neuronal Apoptosis in Neurodegenerative DiseasesNo ratings yet
- Sleep Disorders in Parkinson’s Disease: Management and Case StudyFrom EverandSleep Disorders in Parkinson’s Disease: Management and Case StudyChun-Feng LiuNo ratings yet
- Varicose VeinDocument22 pagesVaricose VeinArslan KhanNo ratings yet
- Disorders of The VeinsDocument5 pagesDisorders of The VeinsArslan KhanNo ratings yet
- Metabolic Syndrome:weight Gain, Arterial HypertensionDocument7 pagesMetabolic Syndrome:weight Gain, Arterial HypertensionArslan KhanNo ratings yet
- Ecg CmuDocument34 pagesEcg CmuArslan KhanNo ratings yet
- Basic Concepts of Clinical ECGDocument40 pagesBasic Concepts of Clinical ECGArslan KhanNo ratings yet
- Fumihiko Maki and His Theory of Collective Form - A Study On Its PDocument278 pagesFumihiko Maki and His Theory of Collective Form - A Study On Its PemiliosasofNo ratings yet
- Deviations and Non Conformances SOP PDFDocument1 pageDeviations and Non Conformances SOP PDFtesteNo ratings yet
- Manuel Resume 17Document2 pagesManuel Resume 17api-286125655No ratings yet
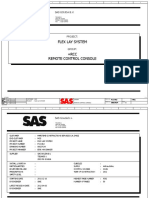
- 00027634-B RCC Wiring DiagramDocument50 pages00027634-B RCC Wiring DiagramKarikalan JayNo ratings yet
- MLOG GX CMXA75 v4 0 322985a0 UM-ENDocument311 pagesMLOG GX CMXA75 v4 0 322985a0 UM-ENjamiekuangNo ratings yet
- Siliporite Opx Pellets Revision 11 - 2017Document2 pagesSiliporite Opx Pellets Revision 11 - 2017Juan Victor Sulvaran Arellano100% (2)
- Parle GDocument26 pagesParle GNikhil Vithaldas Kadam100% (1)
- 13 565Document4 pages13 565Nabeel SheikhNo ratings yet
- I) H3C - MSR3600 - Datasheet PDFDocument15 pagesI) H3C - MSR3600 - Datasheet PDFSON DANG LAMNo ratings yet
- Laboratory Diagnosis of Cerebrospinal Fluid: MM Cajucom MicrobiologyDocument21 pagesLaboratory Diagnosis of Cerebrospinal Fluid: MM Cajucom Microbiologymarc cajucomNo ratings yet
- Form o - Quality AssuranceDocument93 pagesForm o - Quality AssuranceonutocsNo ratings yet
- Semi-Detailed Lesson Plan: Teacher: Blessie Jean A. YbañezDocument3 pagesSemi-Detailed Lesson Plan: Teacher: Blessie Jean A. YbañezJENNIFER YBAÑEZNo ratings yet
- SD Kelas 5Document2 pagesSD Kelas 5mts. miftahulhudaNo ratings yet
- Business Plan MNHS OlangoDocument7 pagesBusiness Plan MNHS OlangoJomar Romero BalmoresNo ratings yet
- Unipro UniGo Quick Guide 1 EN Run and Analyse Rev 1Document2 pagesUnipro UniGo Quick Guide 1 EN Run and Analyse Rev 1jpsdsdsdsdsddNo ratings yet
- QuadEquations PPT Alg2Document16 pagesQuadEquations PPT Alg2Kenny Ann Grace BatiancilaNo ratings yet
- He Va Grass Roller 63 82 Spare PartsDocument48 pagesHe Va Grass Roller 63 82 Spare PartstotcsabNo ratings yet
- Breach of ContractDocument26 pagesBreach of ContractSandeep100% (1)
- Bearing Inspection SOPDocument7 pagesBearing Inspection SOPRianAwangga100% (1)
- HashingDocument1,668 pagesHashingDinesh Reddy KommeraNo ratings yet
- International Journal of Pharmtech Research: Formulation of Aloe Juice (Aloe Vera (L) Burm.F.) Sheet Mask As Anti-AgingDocument10 pagesInternational Journal of Pharmtech Research: Formulation of Aloe Juice (Aloe Vera (L) Burm.F.) Sheet Mask As Anti-AgingAzri RahmadiNo ratings yet
- 35a Ratio and Proportion - H - Question PaperDocument25 pages35a Ratio and Proportion - H - Question Paperfahmid.kabir789No ratings yet
- WIX 51069 Engine Oil Filter Cross ReferenceDocument8 pagesWIX 51069 Engine Oil Filter Cross Referencekman548No ratings yet
- NCP HPNDocument5 pagesNCP HPNGwyneth SantiagoNo ratings yet
- Analgesics in ObstetricsDocument33 pagesAnalgesics in ObstetricsVeena KaNo ratings yet
- Allama Iqbal Open University, Islamabad (Department of Business Administration) WarningDocument5 pagesAllama Iqbal Open University, Islamabad (Department of Business Administration) WarningRana Tauqeer HaiderNo ratings yet
- History: The History of The Hospitality Industry Dates All The WayDocument10 pagesHistory: The History of The Hospitality Industry Dates All The WaySAKET TYAGINo ratings yet
- Portable Boring MachineDocument2 pagesPortable Boring Machinesexmanijak100% (1)
- L01 - Review of Z TransformDocument17 pagesL01 - Review of Z TransformRanjith KumarNo ratings yet





























































































Download as pdf or txt
You might also like
- Yamaha Fazer-Fzh150 CatalogueDocument55 pagesYamaha Fazer-Fzh150 CatalogueAnonymous KoA00wXXD69% (13)
- ptj4008504 PDFDocument8 pagesptj4008504 PDFDiva VashtiNo ratings yet
- Phytotherapy in Treatment of Parkinson's Disease: A Review: Pharmaceutical BiologyDocument9 pagesPhytotherapy in Treatment of Parkinson's Disease: A Review: Pharmaceutical BiologyG. Araya MoraNo ratings yet
- Parkinson's DiseaseDocument14 pagesParkinson's DiseaseRohan MistryNo ratings yet
- Altered Oxidative Stress Levels in Indian Parkinson's Disease Patients With PARK2 MutationsDocument5 pagesAltered Oxidative Stress Levels in Indian Parkinson's Disease Patients With PARK2 MutationssandykumalaNo ratings yet
- Toneuj 10 42 PDFDocument17 pagesToneuj 10 42 PDFpratiwifatmasariNo ratings yet
- Latest Progresses and Methods Used To Treat Parkinson's DiseaseDocument9 pagesLatest Progresses and Methods Used To Treat Parkinson's DiseaseInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Parkinson's Disease: Mechanisms, Translational Models and Management StrategiesDocument14 pagesParkinson's Disease: Mechanisms, Translational Models and Management StrategiesGleyce CabralNo ratings yet
- Science:, 819 (2003) Ted M. Dawson and Valina L. DawsonDocument5 pagesScience:, 819 (2003) Ted M. Dawson and Valina L. DawsonSomanshu BanerjeeNo ratings yet
- TMP - 4306 300 596 1 SM (3) 1791561448Document5 pagesTMP - 4306 300 596 1 SM (3) 1791561448Lulu LuwiiNo ratings yet
- Effect of Walking Along Circle On Foot Prints in Parkinson's On FreezingDocument48 pagesEffect of Walking Along Circle On Foot Prints in Parkinson's On FreezingAnup ShankarwarNo ratings yet
- Parkinsonism A General Motor Disability PDFDocument9 pagesParkinsonism A General Motor Disability PDFRishabh SinghNo ratings yet
- Parkinson's: A Syndrome Rather Than A Disease?: BackgroundDocument8 pagesParkinson's: A Syndrome Rather Than A Disease?: BackgroundEduardo Santana SuárezNo ratings yet
- Review (1) - 2004 - Tabakmna Et AlDocument11 pagesReview (1) - 2004 - Tabakmna Et Alshimonl3892No ratings yet
- Stem Cell-Based Therapies For Parkinson DiseaseDocument17 pagesStem Cell-Based Therapies For Parkinson DiseaseYunita Christiani BiyangNo ratings yet
- PARKINSONISMDocument5 pagesPARKINSONISMPrashanth RajuNo ratings yet
- WJPR Shivaleela Rev ArticleDocument26 pagesWJPR Shivaleela Rev ArticlerajeshNo ratings yet
- Parkinson's Disease: From Bench To BedsideDocument17 pagesParkinson's Disease: From Bench To BedsideSoap 2221No ratings yet
- Involvement of Interferon-Dopaminergic Neurons: in Microglial-Mediated Loss ofDocument10 pagesInvolvement of Interferon-Dopaminergic Neurons: in Microglial-Mediated Loss ofshayley9No ratings yet
- Parkinson and Stem Cell TherapyDocument9 pagesParkinson and Stem Cell TherapyLefinia PutriNo ratings yet
- Evaluation of Anti-Parkinson'sDocument80 pagesEvaluation of Anti-Parkinson'sPanini PatankarNo ratings yet
- TMP FFC1Document28 pagesTMP FFC1FrontiersNo ratings yet
- Biology of Parkinson S Disease Pathogenesis and Pathophysiology of A Multisystem Neurodegenerative DisorderDocument23 pagesBiology of Parkinson S Disease Pathogenesis and Pathophysiology of A Multisystem Neurodegenerative DisorderNelly LeónNo ratings yet
- AANA Journal Course: Update For Nurse Anesthetists Parkinson DiseaseDocument6 pagesAANA Journal Course: Update For Nurse Anesthetists Parkinson DiseaseMarianne GarciaNo ratings yet
- Pharmaceutics 15 00770Document24 pagesPharmaceutics 15 00770Estefania AndreaNo ratings yet
- Parkinsons Disease Recent Advancement and Future AspectsDocument20 pagesParkinsons Disease Recent Advancement and Future AspectsIJRASETPublicationsNo ratings yet
- The Role of Insulin Igf-1Document8 pagesThe Role of Insulin Igf-1Arina Windri RivartiNo ratings yet
- Etiology and Pathophysiology of Parkinson S DiseaseDocument552 pagesEtiology and Pathophysiology of Parkinson S DiseaseAstrid Figueroa100% (2)
- CORTEX PDreviewDocument8 pagesCORTEX PDreviewNadineNo ratings yet
- Manuscript 3Document16 pagesManuscript 3Nana ShkodinaNo ratings yet
- PARKINSONDocument59 pagesPARKINSONvannyNo ratings yet
- BDDKPDocument21 pagesBDDKPChidube UkachukwuNo ratings yet
- Mitochondrial Dysfunction and Mitophagy in Parkinson's: From Familial To Sporadic DiseaseDocument11 pagesMitochondrial Dysfunction and Mitophagy in Parkinson's: From Familial To Sporadic DiseaseKaycsa AdrianaNo ratings yet
- Experimental Validation of Vitex Negundo Leaves Hydroalcoholic Extract For Neuroprotection in Haloperidol Induced Parkinson's Disease in RatDocument16 pagesExperimental Validation of Vitex Negundo Leaves Hydroalcoholic Extract For Neuroprotection in Haloperidol Induced Parkinson's Disease in Ratali abbas rizviNo ratings yet
- Herbal Treatment of Parkinsonism A ReviewDocument7 pagesHerbal Treatment of Parkinsonism A ReviewKartika BorraNo ratings yet
- Background Parkinson Disease Is Recognized As One of The Most Common Neurologic Disorders, AffectingDocument27 pagesBackground Parkinson Disease Is Recognized As One of The Most Common Neurologic Disorders, AffectingCharan Pal SinghNo ratings yet
- The Development of Treatment For Parkinson's Disease: Harishankar Prasad Yadav, Yun LiDocument20 pagesThe Development of Treatment For Parkinson's Disease: Harishankar Prasad Yadav, Yun LiTherezia Sonia Gabriella TanggulunganNo ratings yet
- Spektro Uv VisDocument7 pagesSpektro Uv VisNadaNo ratings yet
- Parkinson's DiseaseDocument9 pagesParkinson's Diseaselucia desantisNo ratings yet
- 1 s2.0 S016517811530559X MainDocument6 pages1 s2.0 S016517811530559X MainDiana DionisioNo ratings yet
- Neurochemistry International: Sunaina Sharma, Puneet Kumar, Rahul DeshmukhDocument8 pagesNeurochemistry International: Sunaina Sharma, Puneet Kumar, Rahul DeshmukhEla MishraNo ratings yet
- 2019 European Academy of Neurology Parkinson DiseaseDocument16 pages2019 European Academy of Neurology Parkinson DiseaseJuan Diego Gutierrez ZevallosNo ratings yet
- The Parkinson Disease Mitochondrial Hypothesis: Where Are We At?Document12 pagesThe Parkinson Disease Mitochondrial Hypothesis: Where Are We At?just for download matterNo ratings yet
- Parkinson's Disease: A Review: Neurology India March 2018Document11 pagesParkinson's Disease: A Review: Neurology India March 2018Alina Vitali TabarceaNo ratings yet
- Parkinson ThesisDocument4 pagesParkinson Thesisandreajimenezomaha100% (1)
- Ijn 5 3 95 1051Document12 pagesIjn 5 3 95 1051Riris AriskaNo ratings yet
- Role of Encapsulated Nano Curcumin in Induced Sh-Sy-5y Cell LineDocument8 pagesRole of Encapsulated Nano Curcumin in Induced Sh-Sy-5y Cell LineInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Jurnal NeuropsikiatriDocument10 pagesJurnal NeuropsikiatriPosterilmiah Majestynas2019No ratings yet
- Haloperidol Dose and Effect of ParkinsonDocument13 pagesHaloperidol Dose and Effect of Parkinsonali abbas rizviNo ratings yet
- Peerj 16762Document21 pagesPeerj 16762jamesraiaanNo ratings yet
- Mitochondrial Pyruvate Carrier Regulates Autophagy, in Ammation, and Neurodegeneration in Experimental Models of Parkinsons DiseaseDocument51 pagesMitochondrial Pyruvate Carrier Regulates Autophagy, in Ammation, and Neurodegeneration in Experimental Models of Parkinsons DiseaseEkeleme Nnamdi MartinsNo ratings yet
- Epidemiology PAthology Genetics and PathophysiologyDocument15 pagesEpidemiology PAthology Genetics and PathophysiologybbadoNo ratings yet
- Https Emedicine - Medscape.com Article 1831191-PrintDocument59 pagesHttps Emedicine - Medscape.com Article 1831191-PrintNoviatiPrayangsariNo ratings yet
- The Genes of Parkinson's DiseaseDocument6 pagesThe Genes of Parkinson's Diseaseapi-26116142No ratings yet
- Pharmacogenetics of Antipsychotic-Induced Movement Disorders As A Resource For Better Understanding Parkinson's Disease Modifier GenesDocument9 pagesPharmacogenetics of Antipsychotic-Induced Movement Disorders As A Resource For Better Understanding Parkinson's Disease Modifier Genesel egendNo ratings yet
- Artículo de GeriatríaDocument14 pagesArtículo de GeriatríaMaria Guadalupe Hernandez JimenezNo ratings yet
- Fifty Years of Clinical Holistic Treatment for Parkinson’s: A Unique ApproachFrom EverandFifty Years of Clinical Holistic Treatment for Parkinson’s: A Unique ApproachRating: 1 out of 5 stars1/5 (1)
- DJ1 PD Review 2021Document8 pagesDJ1 PD Review 2021Krisztina TothNo ratings yet
- Parkinson's Disease A Review 2014 PDFDocument19 pagesParkinson's Disease A Review 2014 PDFjeanNo ratings yet
- Human Caspases and Neuronal Apoptosis in Neurodegenerative DiseasesFrom EverandHuman Caspases and Neuronal Apoptosis in Neurodegenerative DiseasesNo ratings yet
- Sleep Disorders in Parkinson’s Disease: Management and Case StudyFrom EverandSleep Disorders in Parkinson’s Disease: Management and Case StudyChun-Feng LiuNo ratings yet
- Varicose VeinDocument22 pagesVaricose VeinArslan KhanNo ratings yet
- Disorders of The VeinsDocument5 pagesDisorders of The VeinsArslan KhanNo ratings yet
- Metabolic Syndrome:weight Gain, Arterial HypertensionDocument7 pagesMetabolic Syndrome:weight Gain, Arterial HypertensionArslan KhanNo ratings yet
- Ecg CmuDocument34 pagesEcg CmuArslan KhanNo ratings yet
- Basic Concepts of Clinical ECGDocument40 pagesBasic Concepts of Clinical ECGArslan KhanNo ratings yet
- Fumihiko Maki and His Theory of Collective Form - A Study On Its PDocument278 pagesFumihiko Maki and His Theory of Collective Form - A Study On Its PemiliosasofNo ratings yet
- Deviations and Non Conformances SOP PDFDocument1 pageDeviations and Non Conformances SOP PDFtesteNo ratings yet
- Manuel Resume 17Document2 pagesManuel Resume 17api-286125655No ratings yet
- 00027634-B RCC Wiring DiagramDocument50 pages00027634-B RCC Wiring DiagramKarikalan JayNo ratings yet
- MLOG GX CMXA75 v4 0 322985a0 UM-ENDocument311 pagesMLOG GX CMXA75 v4 0 322985a0 UM-ENjamiekuangNo ratings yet
- Siliporite Opx Pellets Revision 11 - 2017Document2 pagesSiliporite Opx Pellets Revision 11 - 2017Juan Victor Sulvaran Arellano100% (2)
- Parle GDocument26 pagesParle GNikhil Vithaldas Kadam100% (1)
- 13 565Document4 pages13 565Nabeel SheikhNo ratings yet
- I) H3C - MSR3600 - Datasheet PDFDocument15 pagesI) H3C - MSR3600 - Datasheet PDFSON DANG LAMNo ratings yet
- Laboratory Diagnosis of Cerebrospinal Fluid: MM Cajucom MicrobiologyDocument21 pagesLaboratory Diagnosis of Cerebrospinal Fluid: MM Cajucom Microbiologymarc cajucomNo ratings yet
- Form o - Quality AssuranceDocument93 pagesForm o - Quality AssuranceonutocsNo ratings yet
- Semi-Detailed Lesson Plan: Teacher: Blessie Jean A. YbañezDocument3 pagesSemi-Detailed Lesson Plan: Teacher: Blessie Jean A. YbañezJENNIFER YBAÑEZNo ratings yet
- SD Kelas 5Document2 pagesSD Kelas 5mts. miftahulhudaNo ratings yet
- Business Plan MNHS OlangoDocument7 pagesBusiness Plan MNHS OlangoJomar Romero BalmoresNo ratings yet
- Unipro UniGo Quick Guide 1 EN Run and Analyse Rev 1Document2 pagesUnipro UniGo Quick Guide 1 EN Run and Analyse Rev 1jpsdsdsdsdsddNo ratings yet
- QuadEquations PPT Alg2Document16 pagesQuadEquations PPT Alg2Kenny Ann Grace BatiancilaNo ratings yet
- He Va Grass Roller 63 82 Spare PartsDocument48 pagesHe Va Grass Roller 63 82 Spare PartstotcsabNo ratings yet
- Breach of ContractDocument26 pagesBreach of ContractSandeep100% (1)
- Bearing Inspection SOPDocument7 pagesBearing Inspection SOPRianAwangga100% (1)
- HashingDocument1,668 pagesHashingDinesh Reddy KommeraNo ratings yet
- International Journal of Pharmtech Research: Formulation of Aloe Juice (Aloe Vera (L) Burm.F.) Sheet Mask As Anti-AgingDocument10 pagesInternational Journal of Pharmtech Research: Formulation of Aloe Juice (Aloe Vera (L) Burm.F.) Sheet Mask As Anti-AgingAzri RahmadiNo ratings yet
- 35a Ratio and Proportion - H - Question PaperDocument25 pages35a Ratio and Proportion - H - Question Paperfahmid.kabir789No ratings yet
- WIX 51069 Engine Oil Filter Cross ReferenceDocument8 pagesWIX 51069 Engine Oil Filter Cross Referencekman548No ratings yet
- NCP HPNDocument5 pagesNCP HPNGwyneth SantiagoNo ratings yet
- Analgesics in ObstetricsDocument33 pagesAnalgesics in ObstetricsVeena KaNo ratings yet
- Allama Iqbal Open University, Islamabad (Department of Business Administration) WarningDocument5 pagesAllama Iqbal Open University, Islamabad (Department of Business Administration) WarningRana Tauqeer HaiderNo ratings yet
- History: The History of The Hospitality Industry Dates All The WayDocument10 pagesHistory: The History of The Hospitality Industry Dates All The WaySAKET TYAGINo ratings yet
- Portable Boring MachineDocument2 pagesPortable Boring Machinesexmanijak100% (1)
- L01 - Review of Z TransformDocument17 pagesL01 - Review of Z TransformRanjith KumarNo ratings yet