Download as pdf or txt
You might also like
- Anesthesiology Resident Manual of Procedures: A Step-by-Step GuideFrom EverandAnesthesiology Resident Manual of Procedures: A Step-by-Step GuideNo ratings yet
- Serology Report: Test Units Normal RangeDocument1 pageSerology Report: Test Units Normal RangeKrishna Shrestha100% (2)
- Oro & Naso Gastric CompetencyDocument2 pagesOro & Naso Gastric CompetencyANNETTE GUEVARRANo ratings yet
- Allegation: United Auburn Indian CommunityDocument16 pagesAllegation: United Auburn Indian CommunityABC10No ratings yet
- Curriculam Vitae: DHA LICENSE: DHA/LS/1872018/830493Document4 pagesCurriculam Vitae: DHA LICENSE: DHA/LS/1872018/830493Gloria JaisonNo ratings yet
- Nasogastric Tubes in Critical Care 2019Document16 pagesNasogastric Tubes in Critical Care 2019Zulkifli JibrilNo ratings yet
- Invasive Procedure Safety Checklist: TRACHEOSTOMYDocument2 pagesInvasive Procedure Safety Checklist: TRACHEOSTOMYMira ManoharanNo ratings yet
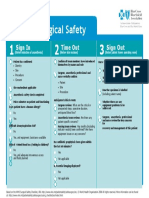
- Modified Surgical Safety Checklist During Covid 19 Pandemic - Addendum - FinalDocument1 pageModified Surgical Safety Checklist During Covid 19 Pandemic - Addendum - FinalLovie Japhet LopezNo ratings yet
- Coronary AngiographyDocument2 pagesCoronary AngiographyKena BenNo ratings yet
- Nasogastric NG Tube Insertion OSCE GuideDocument7 pagesNasogastric NG Tube Insertion OSCE Guidepunam todkarNo ratings yet
- Nursing CS How To Insert A NasogastricNG Tube For Gastric Decompression 03Document1 pageNursing CS How To Insert A NasogastricNG Tube For Gastric Decompression 03solisetherealNo ratings yet
- Surgical Safety ChecklistDocument2 pagesSurgical Safety ChecklistLian CatindigNo ratings yet
- Worksheet #3Document43 pagesWorksheet #3Jo Marchianne PigarNo ratings yet
- WHO Surgical Safety Checklist: InstructionsDocument3 pagesWHO Surgical Safety Checklist: InstructionsireneNo ratings yet
- NG Tube Placement - 13.05Document3 pagesNG Tube Placement - 13.05Rose OcampoNo ratings yet
- Vets Now Surgical Safety ChecklistDocument1 pageVets Now Surgical Safety ChecklistVeterinarios de ArgentinaNo ratings yet
- Sop and Competencies For NG InsertionDocument4 pagesSop and Competencies For NG InsertionReza ShinodaNo ratings yet
- Lampiran 1 Prosedur Tindakan Operasi Hernioraphy Set BasicDocument8 pagesLampiran 1 Prosedur Tindakan Operasi Hernioraphy Set Basiccandra oktaviaNo ratings yet
- NURSING PROCEDURES RT GI SYSTEMDocument226 pagesNURSING PROCEDURES RT GI SYSTEMMika SaldanaNo ratings yet
- Preprocedure Check-In Sign-In Time-Out Sign-Out: Teal Joint Commission and WHODocument2 pagesPreprocedure Check-In Sign-In Time-Out Sign-Out: Teal Joint Commission and WHOYL LYNo ratings yet
- 300-02 # ST 1220, Four Leg Wire Rope SlingDocument3 pages300-02 # ST 1220, Four Leg Wire Rope SlingAgeng LaksitoNo ratings yet
- Size: 137 X 218 MM: Rapid Test For The Detection of Dengue NS 1 Antigen in Human Serum/plasma DeviceDocument4 pagesSize: 137 X 218 MM: Rapid Test For The Detection of Dengue NS 1 Antigen in Human Serum/plasma DeviceMatibar RahmanNo ratings yet
- Combo Dengue KitDocument24 pagesCombo Dengue KitQlife KlinikNo ratings yet
- Competency Statement NEO PUFF - ANSWERS-1Document2 pagesCompetency Statement NEO PUFF - ANSWERS-1madimadi11No ratings yet
- Care of Mother and Child at Risk or With Problems (Acute & Chronic)Document6 pagesCare of Mother and Child at Risk or With Problems (Acute & Chronic)Angela Mae Letaban RegisNo ratings yet
- D20rha25 2013-1Document2 pagesD20rha25 2013-1Icmi KadarsihNo ratings yet
- Guidelines For The Insertion and Management of Enteral TubesDocument19 pagesGuidelines For The Insertion and Management of Enteral TubesAjeng SuparwiNo ratings yet
- SARS COC.2 Ag RDT POST TESTDocument3 pagesSARS COC.2 Ag RDT POST TESTEdyegu EnwakuNo ratings yet
- COVID-19 Advisory - 04072021Document9 pagesCOVID-19 Advisory - 04072021Ryan S. AngelesNo ratings yet
- WHOSurgical Safety Checklist TemplateDocument2 pagesWHOSurgical Safety Checklist Templateraj1969No ratings yet
- Workflow 2020 2021Document36 pagesWorkflow 2020 2021haffizmoradNo ratings yet
- Wa0001.Document2 pagesWa0001.akashcool470No ratings yet
- Covid 19 Rapid Antigen Self Tests Are Approved Australia Ifu 395590Document2 pagesCovid 19 Rapid Antigen Self Tests Are Approved Australia Ifu 395590thecloneofclone69No ratings yet
- AORN Comprehensive Surgical Checklist 2016Document1 pageAORN Comprehensive Surgical Checklist 2016Firma WahyuNo ratings yet
- JT-RT-43 Reading Text: Snakebite Including Sea SnakeDocument14 pagesJT-RT-43 Reading Text: Snakebite Including Sea SnakeJosey K ThomasNo ratings yet
- PGY 1 Survival Guide MICU 1Document3 pagesPGY 1 Survival Guide MICU 1Abdulelah MurshidNo ratings yet
- Interdisciplinary Plan of Care and Patient EducationDocument26 pagesInterdisciplinary Plan of Care and Patient Educationhuggr84629No ratings yet
- Laporan Penghitungan Instrumen & Laporan Operasi SirkumsisiDocument5 pagesLaporan Penghitungan Instrumen & Laporan Operasi SirkumsisiAtmo AtunNo ratings yet
- Best 2016Document6 pagesBest 2016MarlaNo ratings yet
- Surgical Safety: Sign in Time Out Sign OutDocument1 pageSurgical Safety: Sign in Time Out Sign OutNathanNo ratings yet
- NIV ProformaDocument10 pagesNIV ProformaWael N Sh GadallaNo ratings yet
- PPE - Kit TypesDocument1 pagePPE - Kit TypesjaionlyNo ratings yet
- Rsud DR Abdul Aziz Singkawang Intra OperatifDocument4 pagesRsud DR Abdul Aziz Singkawang Intra OperatifTitoNo ratings yet
- Rsud DR Abdul Aziz Singkawang Intra OperatifDocument4 pagesRsud DR Abdul Aziz Singkawang Intra OperatifTitoNo ratings yet
- كتاب التمريض الجديد2022Document206 pagesكتاب التمريض الجديد2022mohamed mohamedNo ratings yet
- ASSESSMENT SUBJECTIVE: "Ang Sakit NG Tagiliran Ko!", As Verbalized byDocument13 pagesASSESSMENT SUBJECTIVE: "Ang Sakit NG Tagiliran Ko!", As Verbalized bychenita ayaNo ratings yet
- Form 10 Nurse's NotesDocument5 pagesForm 10 Nurse's NotesJanelle Cabida SupnadNo ratings yet
- Covid-19 Inpatient Guide 092020.1Document1 pageCovid-19 Inpatient Guide 092020.1Anna JuniedNo ratings yet
- AGS Telehealth-Quickguide FINALDocument1 pageAGS Telehealth-Quickguide FINALSarinahNo ratings yet
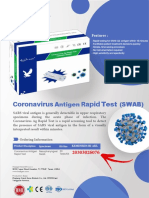
- Coronavirus Rapid Test: Antigen (SWAB)Document6 pagesCoronavirus Rapid Test: Antigen (SWAB)Medika AntapaniNo ratings yet
- LF G3920SA 0010 Clinical ReportDocument16 pagesLF G3920SA 0010 Clinical ReportRoxana HermosoNo ratings yet
- Learning Activity N3A & N3BDocument3 pagesLearning Activity N3A & N3BMikaela JosonNo ratings yet
- Undescended TestisDocument2 pagesUndescended TestisAjo VargheseNo ratings yet
- AORN Comprehensive Surgical Checklist 2016Document2 pagesAORN Comprehensive Surgical Checklist 2016Mevelle Laranjo AsuncionNo ratings yet
- Checklist IOT UTIA HIBA Feb2020Document2 pagesChecklist IOT UTIA HIBA Feb2020Juan FiigueerooaNo ratings yet
- Fast Results 15 Minutes Assay Time Easy Visuallly Interpretation Simple Operation, No Equipment Required High AccuracyDocument1 pageFast Results 15 Minutes Assay Time Easy Visuallly Interpretation Simple Operation, No Equipment Required High AccuracyIbnu Abdul AzizNo ratings yet
- Preprocedure Check-In Sign-In Time-Out Sign-OutDocument2 pagesPreprocedure Check-In Sign-In Time-Out Sign-OutSyahri DzikriNo ratings yet
- FullDocument4 pagesFullchristina malNo ratings yet
- Procedural Skill by NPDocument92 pagesProcedural Skill by NPsankethg93No ratings yet
- Iso 13485 Iso 9001Document56 pagesIso 13485 Iso 9001Juliamm MartNo ratings yet
- Biliopancreatic Endoscopy: Practical ApplicationFrom EverandBiliopancreatic Endoscopy: Practical ApplicationKwok-Hung LaiNo ratings yet
- Can I Cut It? Medical Students' Perceptions of Surgeons and Surgical CareersDocument8 pagesCan I Cut It? Medical Students' Perceptions of Surgeons and Surgical Careersakmal shahzadNo ratings yet
- Peri-Operative Management of Neuromuscular Blockade EJA 2023Document13 pagesPeri-Operative Management of Neuromuscular Blockade EJA 2023lim sjNo ratings yet
- Practical Ortho BROCHURE 2019Document2 pagesPractical Ortho BROCHURE 2019syafiqjaizNo ratings yet
- Care of Clients With Gastrointestinal Disorders Copy 1Document7 pagesCare of Clients With Gastrointestinal Disorders Copy 1Mr. whiteNo ratings yet
- Unhappy Triad of O'DonahueDocument14 pagesUnhappy Triad of O'DonahueGuadalupe GuzmánNo ratings yet
- Asa Physical Status Classification System PDFDocument2 pagesAsa Physical Status Classification System PDFAnonymous 6iLtIrNo ratings yet
- Teleflex Interventional Ordering Catalog: Corporate OfficeDocument50 pagesTeleflex Interventional Ordering Catalog: Corporate OfficeMuhammad Mahbøøb SadiqNo ratings yet
- CPC - Mock 9 Q - New-1Document39 pagesCPC - Mock 9 Q - New-1musayyab muz100% (1)
- Serology and Ultrasound For Diagnosis of Choledocolitiasis 2014Document5 pagesSerology and Ultrasound For Diagnosis of Choledocolitiasis 2014DannyNo ratings yet
- Surgery - 2020 With CorrectionDocument74 pagesSurgery - 2020 With CorrectionUmar JameelNo ratings yet
- Therapeutically Aspects in Esophageal Atresia: RI Spataru, Niculina Bratu, A NicaDocument4 pagesTherapeutically Aspects in Esophageal Atresia: RI Spataru, Niculina Bratu, A Nicanatacha479No ratings yet
- Feeding-Guide-for-Hospitalized-Dogs-and-Cats - PDF Version 1Document2 pagesFeeding-Guide-for-Hospitalized-Dogs-and-Cats - PDF Version 1Damian ChicaizaNo ratings yet
- Facial Nerve Trauma Clinical Evaluation And.41Document15 pagesFacial Nerve Trauma Clinical Evaluation And.41Razaria DailyneNo ratings yet
- Doctor ResumeDocument1 pageDoctor ResumeZeeshan SiddiquiNo ratings yet
- Intimacy and Sexuality After Treatment For Gynecologic CancerDocument37 pagesIntimacy and Sexuality After Treatment For Gynecologic CancerCarleone PrimaNo ratings yet
- Orthopedic Doctor Near MeDocument4 pagesOrthopedic Doctor Near MeDr. Yuvraj KumarNo ratings yet
- Haylen Et Al-2016-Neurourology and UrodynamicsDocument33 pagesHaylen Et Al-2016-Neurourology and UrodynamicsanyNo ratings yet
- OS 2 Module 5 ReportDocument151 pagesOS 2 Module 5 ReportChristineMartinNo ratings yet
- Critical Care Set UpDocument33 pagesCritical Care Set UpSam TullyNo ratings yet
- Ctvs MCQs Delhi 2014Document31 pagesCtvs MCQs Delhi 2014abhaymalur50% (2)
- Poliomyelitis of Foot and Ankle: by DR - Tejaswi Dussa Post Graduate in Ms Ortho Gandhi Hospital, SecunderabadDocument44 pagesPoliomyelitis of Foot and Ankle: by DR - Tejaswi Dussa Post Graduate in Ms Ortho Gandhi Hospital, SecunderabadAneesh JaganathNo ratings yet
- Allen Medical 2019Document144 pagesAllen Medical 2019Ricardo SalazarNo ratings yet
- Exercise # 3: How To Use CalculatorDocument5 pagesExercise # 3: How To Use CalculatorAbdullah SajidNo ratings yet
- Rehabilitation of A Post-Surgical Patella Fracture: Case ReportDocument4 pagesRehabilitation of A Post-Surgical Patella Fracture: Case ReportasmaNo ratings yet
- Week 2 Portfolio QuestionsDocument12 pagesWeek 2 Portfolio Questionsapi-479716004No ratings yet
- Karadenta Turun HargaDocument11 pagesKaradenta Turun HargaAndreas PeniNo ratings yet
- Laparoscopic Hernia Repair: Eva Deerenberg, Irene Mulder and Johan LangeDocument25 pagesLaparoscopic Hernia Repair: Eva Deerenberg, Irene Mulder and Johan LangeKamran AfzalNo ratings yet
- SterileProcessing SkillschecklistDocument2 pagesSterileProcessing SkillschecklistJose TiradoNo ratings yet
- Bilioenteric Bypass Stricture Type II With Hepatolithiasis A Case ReportDocument6 pagesBilioenteric Bypass Stricture Type II With Hepatolithiasis A Case ReportResiden BedahNo ratings yet