Download as pdf or txt
You might also like
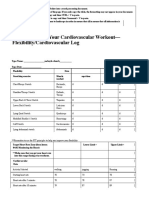
- 4.06 Recording Your Cardiovascular Workout - SchoologyDocument3 pages4.06 Recording Your Cardiovascular Workout - SchoologyMcKayla ChurchNo ratings yet
- Planetary Apothecary - An Astrological Approach To Health and WellnessDocument217 pagesPlanetary Apothecary - An Astrological Approach To Health and Wellnessankita goswami100% (6)
- Vol9No1 USABP Journal 2010Document73 pagesVol9No1 USABP Journal 2010Rucsandra MurzeaNo ratings yet
- Radix Entomolaris in Mandibular First Molars: A Case ReportDocument3 pagesRadix Entomolaris in Mandibular First Molars: A Case ReportAdvanced Research Publications100% (1)
- NURSING-CARE-PLAN-Lung-Cancerxxx 1Document3 pagesNURSING-CARE-PLAN-Lung-Cancerxxx 1Caroline Cha100% (1)
- JBR Journal of Interdisciplinary Medicine and Dental ScienceDocument5 pagesJBR Journal of Interdisciplinary Medicine and Dental ScienceAsmita SonawneNo ratings yet
- Radix Entomolaris: Case Report With Clinical Implication: 10.5005/jp-Journals-10005-1572Document3 pagesRadix Entomolaris: Case Report With Clinical Implication: 10.5005/jp-Journals-10005-1572ratacha chingsuwanrojNo ratings yet
- Prevalence of Radix Entamolaris in Kashmiri PopulationDocument7 pagesPrevalence of Radix Entamolaris in Kashmiri Populationarshad khandayNo ratings yet
- Jurnal Ilmu Konservasi Gigi: PSA Pada Supernumery RootDocument6 pagesJurnal Ilmu Konservasi Gigi: PSA Pada Supernumery RootAchmad Zam Zam AghazyNo ratings yet
- 4.aberrant Root Canal Anatomy in Max 2nd MolarDocument11 pages4.aberrant Root Canal Anatomy in Max 2nd MolarSoham DattaNo ratings yet
- Endodontic Treatment of A Mandibular Second Premolar With Three Roots and Three CanalsDocument3 pagesEndodontic Treatment of A Mandibular Second Premolar With Three Roots and Three CanalsLeticia RiveraNo ratings yet
- 31 Ijss Nov cr02 - 2018Document4 pages31 Ijss Nov cr02 - 2018RAfii KerenNo ratings yet
- Do Not Miss It"radix Entamolaris in Pediatric Patients An Endodontic Challenge: A Case Series and Review of Literature."Document5 pagesDo Not Miss It"radix Entamolaris in Pediatric Patients An Endodontic Challenge: A Case Series and Review of Literature."arshad khandayNo ratings yet
- My 3rd Article PublishedDocument8 pagesMy 3rd Article Publishedcharukapur27No ratings yet
- JjkkkopDocument3 pagesJjkkkopNurul HidayatiNo ratings yet
- Type III Radix Entomolaris in Permanent Mandibular Second MolarDocument3 pagesType III Radix Entomolaris in Permanent Mandibular Second MolarGJR PUBLICATIONNo ratings yet
- Endodontic Management of Mandibular Third Molar With Radix EntomolarisDocument6 pagesEndodontic Management of Mandibular Third Molar With Radix EntomolarisismetNo ratings yet
- "Nonsurgical Endodontic Management of Mandibular First Premolar With 2 Roots: A Rare Case Report" PubDocument2 pages"Nonsurgical Endodontic Management of Mandibular First Premolar With 2 Roots: A Rare Case Report" PubSHILPI TIWARINo ratings yet
- Jurnal 2Document8 pagesJurnal 2NissaNo ratings yet
- Maxillary Second Molar With Four Roots and Five Canals: SciencedirectDocument5 pagesMaxillary Second Molar With Four Roots and Five Canals: SciencedirectKanish AggarwalNo ratings yet
- Of Dental Sciences: Case ReportDocument3 pagesOf Dental Sciences: Case Reportadministraciòn Clinica dentalNo ratings yet
- "Taurodontism" An Endodontic Challenge A Case ReportDocument4 pages"Taurodontism" An Endodontic Challenge A Case ReportDr.O.R.GANESAMURTHINo ratings yet
- Endodontic Management of Radix Entomolaris - A Case ReportDocument4 pagesEndodontic Management of Radix Entomolaris - A Case ReportIJAR JOURNALNo ratings yet
- Four Rooted Maxillary Third Molar A Case Report ofDocument3 pagesFour Rooted Maxillary Third Molar A Case Report ofghinaNo ratings yet
- EndoDocument3 pagesEndoJessicaLisaNugrohoNo ratings yet
- External Root Resorption Associated With Impacted Third Molars: A CaseDocument6 pagesExternal Root Resorption Associated With Impacted Third Molars: A CaseMuskab JonasNo ratings yet
- F Shailendra GuptaDocument7 pagesF Shailendra GuptaRavi KanthNo ratings yet
- The Radix Entomolaris and Paramolaris: Clinical Approach in EndodonticsDocument6 pagesThe Radix Entomolaris and Paramolaris: Clinical Approach in EndodonticsPankajkumar GuptaNo ratings yet
- Three Rooted Mandibular Molar Radix Entomolaris and ParamolarisDocument3 pagesThree Rooted Mandibular Molar Radix Entomolaris and ParamolarisFathul RahmanNo ratings yet
- Dentistry CaseDocument3 pagesDentistry CaseA ANo ratings yet
- Contemporary Approach in Successful Endodontic Intervention in Radix Entomolaris'Document7 pagesContemporary Approach in Successful Endodontic Intervention in Radix Entomolaris'Miranda VicmontNo ratings yet
- ASE Eport: International Journal of Research in Health and Allied SciencesDocument5 pagesASE Eport: International Journal of Research in Health and Allied SciencesRaghav PratapNo ratings yet
- ArtogojoeoctDocument4 pagesArtogojoeoctDewa Ayu Kumara DewiNo ratings yet
- Jomfp 14 80Document3 pagesJomfp 14 80muhammad nauvalNo ratings yet
- EndoDocument3 pagesEndoshobhana20No ratings yet
- The Radix Entomolaris: Management of The Distolingual Root CanalDocument4 pagesThe Radix Entomolaris: Management of The Distolingual Root CanalAlyaNo ratings yet
- 51 667 1 PBDocument2 pages51 667 1 PBMax FaxNo ratings yet
- The Radix Entomolaris in Mandibular First Molars: An Endodontic ChallengeDocument12 pagesThe Radix Entomolaris in Mandibular First Molars: An Endodontic Challengeratacha chingsuwanrojNo ratings yet
- Internal ResorptionDocument4 pagesInternal ResorptionmaharaniNo ratings yet
- Bilateral Maxillary Canines Agenesis: A Case Report and A Literature ReviewDocument4 pagesBilateral Maxillary Canines Agenesis: A Case Report and A Literature ReviewLiga Odontopediatria Rondoniense100% (1)
- Radix EntomolarisDocument12 pagesRadix Entomolarisshatakshi rastogiNo ratings yet
- Cephalometric 3Document7 pagesCephalometric 3Abiyyu WidyaNo ratings yet
- Itsmo en Conducto Mesiobucal en Primera MolarDocument7 pagesItsmo en Conducto Mesiobucal en Primera MolarSaray ValerioNo ratings yet
- Ijoprd 2016 06 102Document5 pagesIjoprd 2016 06 102Unlikely QuestionsNo ratings yet
- EA DS: European Annals of Dental SciencesDocument5 pagesEA DS: European Annals of Dental SciencesEstefania Alvarado ZambranoNo ratings yet
- Endodontic Treatment of Bilateral Maxillary FirstDocument4 pagesEndodontic Treatment of Bilateral Maxillary FirstkhurshidNo ratings yet
- Taurodoncia PDFDocument4 pagesTaurodoncia PDFMarriano DarinoNo ratings yet
- An Unusual Presentation of All The Mandibular AnteDocument3 pagesAn Unusual Presentation of All The Mandibular AnteNadya Raudillah PNo ratings yet
- Pulp Treatment of Triple Tooth in Primary Dentition: Two Case ReportsDocument8 pagesPulp Treatment of Triple Tooth in Primary Dentition: Two Case ReportsDelia Guadalupe Gardea ContrerasNo ratings yet
- Lateral Periodontal CystDocument8 pagesLateral Periodontal CystTejas KulkarniNo ratings yet
- A Rare Case of Twinning Involving Primary Maxillary Lateral Incisor With Review of LiteratureDocument3 pagesA Rare Case of Twinning Involving Primary Maxillary Lateral Incisor With Review of LiteratureSalma FaNo ratings yet
- Endodontc Surgical Management of Mucosal FenistrationDocument3 pagesEndodontc Surgical Management of Mucosal Fenistrationfun timesNo ratings yet
- Zachrisson2004 Management of Missing Maxillary Anterior Teeth With Emphasis On AutotransplantationDocument5 pagesZachrisson2004 Management of Missing Maxillary Anterior Teeth With Emphasis On AutotransplantationplsssssNo ratings yet
- PIIS0889540604009242 EnigmaofClassIImolarfinishingDocument3 pagesPIIS0889540604009242 EnigmaofClassIImolarfinishingMirza GlusacNo ratings yet
- Page 1 PDFDocument1 pagePage 1 PDFMAYRA LORENA ROMERO DIAZNo ratings yet
- 4pulp Space MorphologyDocument68 pages4pulp Space Morphologyraghh roooNo ratings yet
- Original Article Assessment of Different Patterns of Impacted Mandibular Third Molars and Their Associated PathologiesDocument9 pagesOriginal Article Assessment of Different Patterns of Impacted Mandibular Third Molars and Their Associated PathologiesMaulidahNo ratings yet
- 23 Case Rep1 Palatogingival GrooveDocument7 pages23 Case Rep1 Palatogingival GrooveDr.O.R.GANESAMURTHINo ratings yet
- Two Rooted Mandibular Canine With Severe Dilacerations: April 2012Document6 pagesTwo Rooted Mandibular Canine With Severe Dilacerations: April 2012Ashis BiswasNo ratings yet
- Internal Root Resorption Case SeriesDocument5 pagesInternal Root Resorption Case SeriesDana StanciuNo ratings yet
- Amhsr 3 285Document3 pagesAmhsr 3 285Dwi Dayanti AgustinaNo ratings yet
- SJMCR - 411879-882Document4 pagesSJMCR - 411879-882Mukarram FaridiNo ratings yet
- Dentinogenesis Imperfecta A Case ReportDocument3 pagesDentinogenesis Imperfecta A Case ReporthadriaanaNo ratings yet
- Radix Entomolaris: Literature Review and Case Report: SADJ April 2017, Vol 72 No 3 p113 - p117Document5 pagesRadix Entomolaris: Literature Review and Case Report: SADJ April 2017, Vol 72 No 3 p113 - p117ratacha chingsuwanrojNo ratings yet
- Managing Curved Canals: Keywords: Balance Forced Technique, Dilacerations, Precurved Files, ProtaperDocument5 pagesManaging Curved Canals: Keywords: Balance Forced Technique, Dilacerations, Precurved Files, Protaperratacha chingsuwanrojNo ratings yet
- The Radix Entomolaris in Mandibular First Molars: An Endodontic ChallengeDocument12 pagesThe Radix Entomolaris in Mandibular First Molars: An Endodontic Challengeratacha chingsuwanrojNo ratings yet
- Radix Entomolaris: Case Report With Clinical Implication: 10.5005/jp-Journals-10005-1572Document3 pagesRadix Entomolaris: Case Report With Clinical Implication: 10.5005/jp-Journals-10005-1572ratacha chingsuwanrojNo ratings yet
- NSTPDocument1 pageNSTPKimberly RojasNo ratings yet
- HRM20016 Unit Outline - S12024 DR Vinesh-2Document12 pagesHRM20016 Unit Outline - S12024 DR Vinesh-2Roxy OngNo ratings yet
- Quiz Places Around TownDocument2 pagesQuiz Places Around TownROUZBEH BANIHASHEMINo ratings yet
- Annotated BibliographyDocument5 pagesAnnotated Bibliographyapi-259924791No ratings yet
- Table1: Option1 Option2 Option3 Option4 CorrectanswerDocument24 pagesTable1: Option1 Option2 Option3 Option4 CorrectanswerSoom RamadanNo ratings yet
- VUCADocument3 pagesVUCAuzmi06physioNo ratings yet
- AirTrackUS General Product GuideDocument27 pagesAirTrackUS General Product GuideJoe GramNo ratings yet
- Euthanasia in CanadaDocument5 pagesEuthanasia in CanadaMariusz WesolowskiNo ratings yet
- Comprehensive Safety and Health Policies: Policies, Rules, Procedures, Programs, HandbooksDocument13 pagesComprehensive Safety and Health Policies: Policies, Rules, Procedures, Programs, HandbooksMart oro alNo ratings yet
- Elc590 Persuasive Speech Draft and PPT SDocument10 pagesElc590 Persuasive Speech Draft and PPT S2023262198No ratings yet
- Quality and Safety Management in ConstruDocument42 pagesQuality and Safety Management in Construadriansyah maNo ratings yet
- KleinmanDocument66 pagesKleinmanKhirod Chandra MoharanaNo ratings yet
- Control and Resilience The Importance of An Internal Focus To Maintain Resilience in Academically Able StudentsDocument17 pagesControl and Resilience The Importance of An Internal Focus To Maintain Resilience in Academically Able StudentsCarla Si MarianNo ratings yet
- Austin v. Board of Education of Community Unit School District 300, 2022 IL App (4th) 220090-UDocument24 pagesAustin v. Board of Education of Community Unit School District 300, 2022 IL App (4th) 220090-UKHQA NewsNo ratings yet
- Pornography On Today's YouthDocument2 pagesPornography On Today's YouthJaaaNo ratings yet
- Axillary Temperature MeasurementDocument3 pagesAxillary Temperature MeasurementReemix KhalidNo ratings yet
- Lumbar Assessment Form FILLABLE Jun 2020Document2 pagesLumbar Assessment Form FILLABLE Jun 2020FejesNo ratings yet
- HIS1249 - BSBRSK501 - Assessment 2 Case Study - v1.9 - Feb 2020Document12 pagesHIS1249 - BSBRSK501 - Assessment 2 Case Study - v1.9 - Feb 2020Ivan LisdiyanaNo ratings yet
- 4 Unit-Vi-Diet-TherapyDocument13 pages4 Unit-Vi-Diet-TherapyTrinidad SherwinNo ratings yet
- Personnel Management in SalesDocument9 pagesPersonnel Management in SalesraveendramanipalNo ratings yet
- Diet and Exercise EffectDocument5 pagesDiet and Exercise Effectsafar akramNo ratings yet
- Legal Basis Basic Background Purpose/ Goal Significance: Activity 2Document1 pageLegal Basis Basic Background Purpose/ Goal Significance: Activity 2RodrinerBillonesNo ratings yet
- Pain Management in ChildrenDocument8 pagesPain Management in ChildrenKrizle AdazaNo ratings yet
- Cause EffectDocument2 pagesCause EffectcocoNo ratings yet
- HSM 2 Project Management Presentation#2-2Document61 pagesHSM 2 Project Management Presentation#2-2Waltas Kariuki100% (1)
- New Grad Amanda Truong Resume RevisedDocument4 pagesNew Grad Amanda Truong Resume Revisedapi-621660715No ratings yet