Download as pdf or txt
You might also like
- Formwork and ScaffoldingDocument43 pagesFormwork and ScaffoldingAarti Vij50% (2)
- 16-Port Antenna Frequency Range Dual Polarization HPBW Gain Adjust. Electr. DTDocument7 pages16-Port Antenna Frequency Range Dual Polarization HPBW Gain Adjust. Electr. DTestebanarcaNo ratings yet
- TEM Slot Booking Form-ExternalDocument1 pageTEM Slot Booking Form-ExternalMadan Mohan ReddyNo ratings yet
- Week16 N9Document3 pagesWeek16 N920131A05N9 SRUTHIK THOKALANo ratings yet
- Java MCQDocument10 pagesJava MCQsatyam sharmaNo ratings yet
- Objective Type Questions: (1 Mark Each)Document5 pagesObjective Type Questions: (1 Mark Each)SIRSHA PATTANAYAKNo ratings yet
- CleaningDocument555 pagesCleaningifan1984No ratings yet
- Detailed Estimation Roof PDFDocument7 pagesDetailed Estimation Roof PDFFranzer BalbinNo ratings yet
- SEEPDocument10 pagesSEEPJose Miguel Valencia BallesterosNo ratings yet
- Itb 2018-05 Itb For Bac Copy - RevisedDocument1 pageItb 2018-05 Itb For Bac Copy - RevisedDASURECOWebTeamNo ratings yet
- Sta104 2 July202 Set2Document6 pagesSta104 2 July202 Set2Mi MiNo ratings yet
- Assignment 1 BDocument5 pagesAssignment 1 BAbhishek SinghNo ratings yet
- Cse3090y 2020 2Document9 pagesCse3090y 2020 2Khritish BhoodhooNo ratings yet
- IP Exercise To Students 2020 PDFDocument5 pagesIP Exercise To Students 2020 PDFherrajohnNo ratings yet
- Python LabDocument79 pagesPython LabnaveenNo ratings yet
- MS-Computer Science-12-Common ExamDocument9 pagesMS-Computer Science-12-Common ExamDeivanai K CSNo ratings yet
- CorrectionW01 Problem Exam - Process Strategy-EstherKisekkaDocument7 pagesCorrectionW01 Problem Exam - Process Strategy-EstherKisekkapauljesse2023No ratings yet
- Theory of Constraints Lab Experiments (Report)Document10 pagesTheory of Constraints Lab Experiments (Report)Mahmoud KassabNo ratings yet
- OPM I-Solution Sheet Chap 2 Problems: SolutionsDocument22 pagesOPM I-Solution Sheet Chap 2 Problems: SolutionsKaushal BakhaiNo ratings yet
- Pet. ATOS 41693. SE - IBE - BDS - Cyber - STM - McAfee ProfileDocument3 pagesPet. ATOS 41693. SE - IBE - BDS - Cyber - STM - McAfee ProfileSalatiel NavaNo ratings yet
- Value Chain FormatDocument17 pagesValue Chain FormatMk Seifu EthioNo ratings yet
- XSX Xs XDocument8 pagesXSX Xs XValentin CastroNo ratings yet
- Project CrashingDocument24 pagesProject CrashingVINITHA100% (1)
- Oepe 14602Document2 pagesOepe 14602Apeksha SinghNo ratings yet
- ReportDocument13 pagesReportSaugat ThapaNo ratings yet
- Nikumbuke Computer ExamDocument4 pagesNikumbuke Computer Examwycliffekinyili7No ratings yet
- Overtime Claim Form: Date: Location: Work ScopeDocument2 pagesOvertime Claim Form: Date: Location: Work ScopeMatthew Ho Choon LimNo ratings yet
- Sta104 Try 2 - 230615 - 235749Document5 pagesSta104 Try 2 - 230615 - 235749Siti Hajar Khalidah100% (1)
- Perfect CompetitionDocument26 pagesPerfect CompetitionNaman AroraNo ratings yet
- Vietnam DX SaaS Landscape 2022 enDocument32 pagesVietnam DX SaaS Landscape 2022 enLinh Nguyễn VănNo ratings yet
- Hard Activity On JavaDocument5 pagesHard Activity On JavaMilbertNo ratings yet
- Forecast Demand by Quarter (1,000 Case Units)Document3 pagesForecast Demand by Quarter (1,000 Case Units)KaMan CHAUNo ratings yet
- Legend: Problem Solving Information Literacy Critical ThinkingDocument2 pagesLegend: Problem Solving Information Literacy Critical ThinkingShien Zan SouNo ratings yet
- Woodward Training Schedule 2018Document1 pageWoodward Training Schedule 2018JUAN PEREZNo ratings yet
- ABSEN KKN AzizahDocument2 pagesABSEN KKN AzizahazizahNo ratings yet
- 21PGDM152 - RACHIT MRINAL - Don't Bother Me, Can't Cope AssignmentDocument6 pages21PGDM152 - RACHIT MRINAL - Don't Bother Me, Can't Cope AssignmentRachit Mrinal100% (3)
- NumAT Task 4 and 5Document2 pagesNumAT Task 4 and 5SQAGDZRFWSRFXBC ERDFNo ratings yet
- Project: System. A Database Is A Collection of Structured Information Like The 200 Order Forms, All WithDocument3 pagesProject: System. A Database Is A Collection of Structured Information Like The 200 Order Forms, All WithLuckmore MapongaNo ratings yet
- PT. Archetype Engineering and Industry Consultants: 1.0 Scope of WorkDocument3 pagesPT. Archetype Engineering and Industry Consultants: 1.0 Scope of WorkcitramuaraNo ratings yet
- Adding/Subtracting Decimals (A)Document30 pagesAdding/Subtracting Decimals (A)Ron Man BautistaNo ratings yet
- Technosafe: Test Report of Ambient NoiseDocument2 pagesTechnosafe: Test Report of Ambient NoiseAshish TiwariNo ratings yet
- Simulation Exercise 2Document2 pagesSimulation Exercise 2LouieNo ratings yet
- Firewall Change Request Form 1.0 2 (1)Document16 pagesFirewall Change Request Form 1.0 2 (1)udugadesupriya146No ratings yet
- Assignment 2Document4 pagesAssignment 2Laith AboshamatNo ratings yet
- Nanisivik Awos, Nu, Canada: 2013 ASHRAE Handbook - Fundamentals (SI) © 2013 ASHRAE, IncDocument1 pageNanisivik Awos, Nu, Canada: 2013 ASHRAE Handbook - Fundamentals (SI) © 2013 ASHRAE, Inccbdk71No ratings yet
- JC Maclean International Fzco Reem Mall, Abu Dhabi, Uae - Weekly DashboardDocument25 pagesJC Maclean International Fzco Reem Mall, Abu Dhabi, Uae - Weekly DashboardsarahNo ratings yet
- Crashing Progarm: EstimationDocument6 pagesCrashing Progarm: EstimationKadhim FalahNo ratings yet
- Staad - Pro Connect Edition Fundamentals Beginner'S Training: Xstructures Engineering ConsultantsDocument2 pagesStaad - Pro Connect Edition Fundamentals Beginner'S Training: Xstructures Engineering ConsultantsChristian Angelo BermudezNo ratings yet
- Estabilidad de Presa Millo Sin SisDocument6 pagesEstabilidad de Presa Millo Sin SisJose Miguel Valencia BallesterosNo ratings yet
- Bradford Manufacturing Group-6Document3 pagesBradford Manufacturing Group-6DizziNo ratings yet
- Mes Stadium Design: BeamsDocument2 pagesMes Stadium Design: BeamsANKESH SHRIVASTAVANo ratings yet
- Operational Research: Group-6 Case StudyDocument70 pagesOperational Research: Group-6 Case Studymasrawy2010No ratings yet
- Panel InfoDocument4 pagesPanel InfoMohh KeNo ratings yet
- Name of Department/Agency: DENR (2) Name of Service: Document AuthenticationDocument11 pagesName of Department/Agency: DENR (2) Name of Service: Document Authenticationcenro staritaNo ratings yet
- Quality Monthly Report "Name of The Project": Logo EeccDocument1 pageQuality Monthly Report "Name of The Project": Logo EeccGisselle Morales TorresNo ratings yet
- March - Test - Computing (Pre IG - Night - 0.4)Document3 pagesMarch - Test - Computing (Pre IG - Night - 0.4)Eaint Sann YayNo ratings yet
- Oct 2Document1 pageOct 2camangidawage143No ratings yet
- Pow 17J00009Document3 pagesPow 17J00009amroussyNo ratings yet
- 2009 DetailsDocument19 pages2009 DetailshrrcrgkNo ratings yet
- UBS-Corporate Certificate Document in WordDocument2 pagesUBS-Corporate Certificate Document in WordPuvanesh 2501No ratings yet
- Joshua EssayDocument3 pagesJoshua EssayPuvanesh 2501No ratings yet
- Nursery 2 Newsletter 15-19 Nov 2021Document2 pagesNursery 2 Newsletter 15-19 Nov 2021Puvanesh 2501No ratings yet
- Nursery 2 Newsletter 24 - 4 Feb 2022Document2 pagesNursery 2 Newsletter 24 - 4 Feb 2022Puvanesh 2501No ratings yet
- Documents To Be Kept at The Registered OfficeDocument2 pagesDocuments To Be Kept at The Registered OfficePuvanesh 2501No ratings yet
- Jaypirakas EssayDocument2 pagesJaypirakas EssayPuvanesh 2501No ratings yet
- 26th - 29th May Langkawi Trip 2022Document3 pages26th - 29th May Langkawi Trip 2022Puvanesh 2501No ratings yet
- UntitledDocument1 pageUntitledPuvanesh 2501No ratings yet
- Run BW Setup TableDocument10 pagesRun BW Setup Tableko68565No ratings yet
- Extruder SEIDocument6 pagesExtruder SEIMohd Ikram SolehuddinNo ratings yet
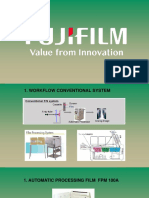
- FPM100A Baisc TrainingDocument43 pagesFPM100A Baisc TrainingErwin TeknisiNo ratings yet
- Bolomoters Running Backward 2006Document12 pagesBolomoters Running Backward 2006sapa3No ratings yet
- Think Smarter TogetherDocument1 pageThink Smarter TogetherKi KiNo ratings yet
- General MIDI Drum Kit MapDocument4 pagesGeneral MIDI Drum Kit Mapmartzo-50% (2)
- Project Report On Kajaria Ceramic LTD For BBADocument52 pagesProject Report On Kajaria Ceramic LTD For BBAPari Savla100% (2)
- William McElcheran Paper To Bronze 2013 Digital Exhibition CatalogueDocument19 pagesWilliam McElcheran Paper To Bronze 2013 Digital Exhibition CatalogueJohn MacGregor NewmanNo ratings yet
- Tvlineup EutelsatDocument109 pagesTvlineup Eutelsatoluomo1No ratings yet
- Aplication Form PDLDocument4 pagesAplication Form PDLTarun GoelNo ratings yet
- RD 700gx RD 300gx BrochureDocument2 pagesRD 700gx RD 300gx BrochureYonathan Mikhael Susanto RambaNo ratings yet
- Digital Libraries (Chap 1 & 2)Document23 pagesDigital Libraries (Chap 1 & 2)bobot91100% (2)
- 2.37 Rso Training Standard Syllabi For Training Courses On Radiological SafetyDocument96 pages2.37 Rso Training Standard Syllabi For Training Courses On Radiological SafetyashwiniNo ratings yet
- Benning Products BrochureDocument14 pagesBenning Products BrochureGlen FordNo ratings yet
- Introduction To Research MethodsDocument12 pagesIntroduction To Research Methodsapi-3825778100% (1)
- 0 Faade 219904@20194917571Document4 pages0 Faade 219904@20194917571Mikayrie D. DulayNo ratings yet
- What's Next "Cold Fusion"?.. Super Low Cost Power Generators Vying For Mainstream Spot LightDocument387 pagesWhat's Next "Cold Fusion"?.. Super Low Cost Power Generators Vying For Mainstream Spot LightBen Rusuisiak50% (2)
- 5.energy Saving Tips - Home AppliancesDocument16 pages5.energy Saving Tips - Home Appliancessrinivas_k4555100% (1)
- ANNEX 10 - Aeronautical Telecomunications (Volume V)Document48 pagesANNEX 10 - Aeronautical Telecomunications (Volume V)Syahid MachedaNo ratings yet
- 1840-E-Uster Sentinel Final Web LowresDocument7 pages1840-E-Uster Sentinel Final Web LowresJuan Francisco Rubio JovelNo ratings yet
- Bulletin 4900 PDFDocument44 pagesBulletin 4900 PDFdjole112No ratings yet
- Airlift BioreactorDocument18 pagesAirlift BioreactorDark_Kiro100% (1)
- Powador 39.0 - 72.0 TL3: Transformerless, Three-Phase String InvertersDocument4 pagesPowador 39.0 - 72.0 TL3: Transformerless, Three-Phase String InvertersHayat DamouniNo ratings yet
- Mechanical Design Engineer Resume Sample - LiveCareerDocument4 pagesMechanical Design Engineer Resume Sample - LiveCareerचन्दनप्रसादNo ratings yet
- Gales RobotSimulation AToolforProjectSuccessDocument52 pagesGales RobotSimulation AToolforProjectSuccessMarcelo NogueiraNo ratings yet
- Research PaperDocument3 pagesResearch PaperEisen LadotNo ratings yet
- DC220 ErrorDocument4 pagesDC220 ErrorTonyandAnthonyNo ratings yet
- 188 - Downs, ChrisDocument10 pages188 - Downs, ChrisrockmanqhNo ratings yet