Download as docx, pdf, or txt
You might also like
- Wound Dressing ProcedureDocument2 pagesWound Dressing ProcedureCaptainMarksman100% (1)
- Level III Performance ChecklistDocument43 pagesLevel III Performance ChecklistMikhaela Andree MarianoNo ratings yet
- Nursing ProceduresDocument17 pagesNursing Proceduresjomlovekriz75% (4)
- External Douche and Open Gloving ProceduresDocument9 pagesExternal Douche and Open Gloving ProceduresBudoy WashupapiNo ratings yet
- Final Project ReportDocument61 pagesFinal Project ReportAakanksha BharatiNo ratings yet
- Wound CareDocument3 pagesWound Caregrangerhermionep100% (1)
- Home Visit Steps: Perform The Bag TechniqueDocument4 pagesHome Visit Steps: Perform The Bag TechniqueRasec Nayr CoseNo ratings yet
- Wound DressingDocument5 pagesWound Dressingsinuaish syaNo ratings yet
- Wound Care ChecklistDocument5 pagesWound Care Checklistacademic purposes100% (1)
- Caring For A Hemovac DrainDocument15 pagesCaring For A Hemovac DrainJaily Mariano0% (1)
- Cleaning A Sutured Wound & Changing A Dressing On A Wound With A Drain Procedure ChecklistDocument3 pagesCleaning A Sutured Wound & Changing A Dressing On A Wound With A Drain Procedure ChecklistMonicaElizadePazNo ratings yet
- Final - Perineal - Prep RatioDocument7 pagesFinal - Perineal - Prep RatioJanine BaringNo ratings yet
- Wound DressingDocument11 pagesWound DressingKRIZIA ANE A. SULONGNo ratings yet
- Checklist Wound CareDocument3 pagesChecklist Wound CareJenny Agustin FabrosNo ratings yet
- Surgical DressingDocument7 pagesSurgical DressingGabz GabbyNo ratings yet
- Colostomy Care DefinitionDocument3 pagesColostomy Care DefinitionAICEL A. ABILNo ratings yet
- Wound Care ChecklistDocument5 pagesWound Care ChecklistAngela Nicole MarcosNo ratings yet
- Applying Wound Barriers and DressingsDocument2 pagesApplying Wound Barriers and DressingsCarlyn AguasNo ratings yet
- Wound Care PefDocument3 pagesWound Care PefJenny Agustin FabrosNo ratings yet
- Wound Care - PefDocument3 pagesWound Care - PefJenny Agustin FabrosNo ratings yet
- Wound DressingsDocument7 pagesWound DressingsJaymi MacapagalNo ratings yet
- Surgical Hand Scrub 1Document4 pagesSurgical Hand Scrub 1Alfred Jayson RuizNo ratings yet
- Procedure Checklist Chapter 34: Applying A Hydrocolloid DressingDocument2 pagesProcedure Checklist Chapter 34: Applying A Hydrocolloid DressingjthsNo ratings yet
- Rationale (Enema)Document10 pagesRationale (Enema)Mina RacadioNo ratings yet
- Procedure Checklist Chapter 34: Removing and Applying Dry DressingsDocument2 pagesProcedure Checklist Chapter 34: Removing and Applying Dry DressingsjthsNo ratings yet
- Respiratory AssessmentDocument3 pagesRespiratory AssessmentSharina Marie CoderaNo ratings yet
- Wound Care Procedure StudentsDocument2 pagesWound Care Procedure StudentsJan Philippe BelandoNo ratings yet
- Wound Dressing ChecklistDocument3 pagesWound Dressing ChecklistBUAHIN JANNA100% (1)
- Level III Performance Checklist: Preparing A Sterile Field: Using A Commercially Prepared Sterile Kit/Tray PurposeDocument40 pagesLevel III Performance Checklist: Preparing A Sterile Field: Using A Commercially Prepared Sterile Kit/Tray PurposeRichmon SantosNo ratings yet
- Roleplay All ProceduresDocument10 pagesRoleplay All Proceduresmej popesNo ratings yet
- Aseptic Wound Dressing ProcedureDocument9 pagesAseptic Wound Dressing ProcedureConvalescent Nursing HomeNo ratings yet
- Colostomy Ileostomy CareDocument6 pagesColostomy Ileostomy Careأبوأحمد الحكيمNo ratings yet
- Wound CareDocument3 pagesWound CarehaneyumiiiNo ratings yet
- Kle U Institute of Nursing Sciences, BelgaumDocument8 pagesKle U Institute of Nursing Sciences, BelgaumShivraj DandgiNo ratings yet
- Wound Dressing Cesarean SectionDocument7 pagesWound Dressing Cesarean Sectionneo natalNo ratings yet
- University of The EastDocument33 pagesUniversity of The EastSEAN MELNOR LOSBAÑESNo ratings yet
- Clinical Teaching Plan FormatDocument12 pagesClinical Teaching Plan FormatEmerald ArcenaNo ratings yet
- Colostomy Ileostomy CareDocument6 pagesColostomy Ileostomy CareRosevick BadocoNo ratings yet
- Midterm Topics After Hygiene 1Document39 pagesMidterm Topics After Hygiene 1Budoy WashupapiNo ratings yet
- Finalrationale CAGABCABDocument9 pagesFinalrationale CAGABCABCagabcab Canibel MelanyNo ratings yet
- COLOSTOMYDocument4 pagesCOLOSTOMYbambam1aNo ratings yet
- Skin Sutures and StaplesDocument4 pagesSkin Sutures and StaplesDrmirfat AlkashifNo ratings yet
- Perilite Exposure JuecoDocument3 pagesPerilite Exposure JuecoTrishaNo ratings yet
- External DoucheDocument6 pagesExternal DoucheSha AbdulaNo ratings yet
- Manual of Procedures 2nd Year 1st SemDocument28 pagesManual of Procedures 2nd Year 1st SemJan Erika AlmeronNo ratings yet
- Nicole - DBE and Wound DressingDocument4 pagesNicole - DBE and Wound DressingnicolemellaNo ratings yet
- Wound Care RationaleDocument3 pagesWound Care RationaleKyleNo ratings yet
- NCMA113 FUNDA SKILL 3 Open Gloving Method Applying Removing Sterlile GlovesDocument2 pagesNCMA113 FUNDA SKILL 3 Open Gloving Method Applying Removing Sterlile Glovesbriana lopezNo ratings yet
- SATAIRAPAN Rationale Wound CareDocument2 pagesSATAIRAPAN Rationale Wound CareMichelle SatairapanNo ratings yet
- Perineal CareDocument3 pagesPerineal CareandreabreeNo ratings yet
- Applying A Wet-To-dry DressingDocument4 pagesApplying A Wet-To-dry DressingBianca Mikaela Dosdos0% (1)
- Donning and Removing Sterile Gloves (Open Method) Preparation RationaleDocument2 pagesDonning and Removing Sterile Gloves (Open Method) Preparation RationalecharmainchavezNo ratings yet
- 0nb (Tiz 0i9v-HpcsdDocument12 pages0nb (Tiz 0i9v-HpcsdKelvin TimssNo ratings yet
- Administering IntradermalDocument4 pagesAdministering IntradermalNezukoNo ratings yet
- Delivery Room ProceduresDocument25 pagesDelivery Room ProceduresTintin HonraNo ratings yet
- 2020 MSN Oropharyngeal and Nasopharyngeal Suctioning For The Students 1Document3 pages2020 MSN Oropharyngeal and Nasopharyngeal Suctioning For The Students 1John MalkovicNo ratings yet
- Procedure Checklist Chapter 34: Applying A Transparent Film DressingDocument1 pageProcedure Checklist Chapter 34: Applying A Transparent Film DressingjthsNo ratings yet
- Glucose TestingDocument5 pagesGlucose TestingMoira Julianne Serognas BrigoliNo ratings yet
- Survival Skills: How to Survive Anything and Anywhere in the World (A Comprehensive Guide to Preparing for and Overcoming Challenges of Earthquakes)From EverandSurvival Skills: How to Survive Anything and Anywhere in the World (A Comprehensive Guide to Preparing for and Overcoming Challenges of Earthquakes)No ratings yet
- Captivating and Simplistic No-Sew Protective Face Masks: A Quick and Easy DIY Face Mask with Step-by-Step Instructions plus IllustrationsFrom EverandCaptivating and Simplistic No-Sew Protective Face Masks: A Quick and Easy DIY Face Mask with Step-by-Step Instructions plus IllustrationsNo ratings yet
- UntitledDocument7 pagesUntitledcharmainchavezNo ratings yet
- Unit 1 The Key Concepts in EthicsDocument9 pagesUnit 1 The Key Concepts in EthicscharmainchavezNo ratings yet
- Rubrics For Rubrics Rating of Group 4Document4 pagesRubrics For Rubrics Rating of Group 4charmainchavezNo ratings yet
- UntitledDocument6 pagesUntitledcharmainchavezNo ratings yet
- TEM Quiz No. 4 BSNDocument2 pagesTEM Quiz No. 4 BSNcharmainchavezNo ratings yet
- Donning and Removing Sterile Gloves (Open Method) Preparation RationaleDocument2 pagesDonning and Removing Sterile Gloves (Open Method) Preparation RationalecharmainchavezNo ratings yet
- DSA Weekly PlanDocument3 pagesDSA Weekly PlanJatin0% (1)
- Letter of TransmittalDocument7 pagesLetter of TransmittalGolam Samdanee TaneemNo ratings yet
- ExerciseDocument3 pagesExerciseWiinarsihNo ratings yet
- sECOND pERIODICAL tEST in hEALTH 6Document4 pagessECOND pERIODICAL tEST in hEALTH 6Marivic Echaveria DepalaNo ratings yet
- Notes MT Module I - KTUDocument47 pagesNotes MT Module I - KTURagesh Dudu100% (1)
- J33Document6 pagesJ33Belkisa ŠaćiriNo ratings yet
- Rama 2Document3 pagesRama 2Ramasubba ReddyNo ratings yet
- Gerson Therapy HandbookDocument192 pagesGerson Therapy HandbookSérgio Luiz Carvalho Bernardes100% (1)
- Microsoft Vicual C++Document1 pageMicrosoft Vicual C++parlingultomNo ratings yet
- H CSRDocument2 pagesH CSRLuvkush RulesNo ratings yet
- 43 CA CPT Dec 2010 Question Paper With Answer Key 2Document6 pages43 CA CPT Dec 2010 Question Paper With Answer Key 2Vishal Gattani100% (1)
- Arslan 20 Bba 11Document11 pagesArslan 20 Bba 11Arslan Ahmed SoomroNo ratings yet
- Netflix Ing British English StudentDocument8 pagesNetflix Ing British English StudentДианка МотыкаNo ratings yet
- August 2013: Zion'S Lutheran ChurchDocument10 pagesAugust 2013: Zion'S Lutheran ChurchConnie AllgireNo ratings yet
- Garcillano V.: The House of RepresentativesDocument11 pagesGarcillano V.: The House of RepresentativesRoselle LagamayoNo ratings yet
- Current Issues, Status and Applications of GIS To Marine FisheriesDocument33 pagesCurrent Issues, Status and Applications of GIS To Marine FisheriesKyran Joeffer EsporlasNo ratings yet
- Architectural Design 9 Thesis Research Writing: 3 Proposal DraftDocument7 pagesArchitectural Design 9 Thesis Research Writing: 3 Proposal DraftVANESSA DELA TORRENo ratings yet
- B e BmeDocument42 pagesB e BmeRAMESHKUMAR.S MCE-LECT/MECHNo ratings yet
- Master Thesis Report Kunal Choudhary 2021-11-02Document75 pagesMaster Thesis Report Kunal Choudhary 2021-11-02margoumnarimene2001No ratings yet
- G.R. No. L-48176 PDFDocument7 pagesG.R. No. L-48176 PDFAj SobrevegaNo ratings yet
- Approach To Polyarthritis For The Primary Care Physician: Arielle Freilich, DO, PGY2 & Helaine Larsen, DODocument8 pagesApproach To Polyarthritis For The Primary Care Physician: Arielle Freilich, DO, PGY2 & Helaine Larsen, DOLydia IsaacNo ratings yet
- NSDL Conso File FVU Error Code ListDocument22 pagesNSDL Conso File FVU Error Code Listlekireddy33% (9)
- Revolusi Industri 4.0: Impak Terhadap Perkembangan Pendidikan Tinggi Di MalaysiaDocument13 pagesRevolusi Industri 4.0: Impak Terhadap Perkembangan Pendidikan Tinggi Di Malaysiaeiman medinaNo ratings yet
- Royal Prince Dasma Electrical Plan 1Document2 pagesRoyal Prince Dasma Electrical Plan 1Ryan Anthony UmaliNo ratings yet
- Motion To Reconsider-Vacate-Modify Order, C.a.11 No.13-11585-BDocument62 pagesMotion To Reconsider-Vacate-Modify Order, C.a.11 No.13-11585-BNeil GillespieNo ratings yet
- Report HR6102 RH EducationandLaborDocument161 pagesReport HR6102 RH EducationandLaborRyland BartonNo ratings yet
- AIDICO ECO-STONE Sustainable System Implementation For Natural Stone Production and Use PDFDocument81 pagesAIDICO ECO-STONE Sustainable System Implementation For Natural Stone Production and Use PDFDaniNo ratings yet
- Asme 2a - Sa-350 PDFDocument12 pagesAsme 2a - Sa-350 PDFEswaran100% (1)
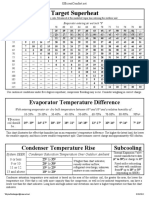
- Charging and TD Chart PlusDocument1 pageCharging and TD Chart PlusFaquruddin AliNo ratings yet