Download as pdf or txt
You might also like
- Claims Management Policy TemplateDocument2 pagesClaims Management Policy TemplateSharif Fayiz AbushaikhaNo ratings yet
- Adrenergic AntagonistsDocument29 pagesAdrenergic AntagonistsBenedict Brashi100% (1)
- PDFDocument577 pagesPDFOmaff Hurtadi100% (1)
- Group 10 PHARMACOLOGYDocument50 pagesGroup 10 PHARMACOLOGYm.yasir.geoNo ratings yet
- Beta Adrenergic Blockers: SympatholyticDocument12 pagesBeta Adrenergic Blockers: SympatholyticAbdullah asadNo ratings yet
- 3-11-2018 Beta Blocking DrugsDocument65 pages3-11-2018 Beta Blocking DrugsDharmendra GohilNo ratings yet
- Adrenoceptor Antagonist Drugs-IIDocument14 pagesAdrenoceptor Antagonist Drugs-IIcelecosibNo ratings yet
- Beta-Blockers For Cardiovascular Conditions:: One Size Does Not Fit All PatientsDocument7 pagesBeta-Blockers For Cardiovascular Conditions:: One Size Does Not Fit All PatientsspalemaxNo ratings yet
- Beta Adrenergic Blockers ArvindDocument12 pagesBeta Adrenergic Blockers ArvindA2Z GyanNo ratings yet
- Adrenergic AntagonistDocument29 pagesAdrenergic AntagonistAreesha ArifNo ratings yet
- What Is AtenololDocument9 pagesWhat Is AtenololAbdelrhman AboodaNo ratings yet
- Sympa T Holy TicsDocument47 pagesSympa T Holy Ticsahmad tariqNo ratings yet
- YogeshDocument49 pagesYogeshapi-3741769No ratings yet
- Antiadrenergic DrugsDocument44 pagesAntiadrenergic DrugsHUZAIFA YAMAANNo ratings yet
- Propranolol Introduced in 1963 Was A Therapeutic BreakthroughDocument5 pagesPropranolol Introduced in 1963 Was A Therapeutic BreakthroughOmkar Singh100% (1)
- Bisoprolol: A New Beta-Adrenoceptor Blocking Drug: B. N. C. PrichardDocument9 pagesBisoprolol: A New Beta-Adrenoceptor Blocking Drug: B. N. C. PrichardspalemaxNo ratings yet
- Obat Antihypertensi: DR Med DR - Widharto PH, SPFK Farmakologi Dan Terapi Fak - Kedokteran UgmDocument38 pagesObat Antihypertensi: DR Med DR - Widharto PH, SPFK Farmakologi Dan Terapi Fak - Kedokteran UgmNi Made Dwiki AndriyaniNo ratings yet
- Beta-Blockers: Beta-Blocker Options Following Funding Changes To Betaloc CRDocument12 pagesBeta-Blockers: Beta-Blocker Options Following Funding Changes To Betaloc CRDewi Nurul SakinahNo ratings yet
- Beta BlockersDocument3 pagesBeta BlockersWil LesterNo ratings yet
- 6 SymaptholyticDocument48 pages6 SymaptholyticYoueel IbrahemNo ratings yet
- Auspar Labetalol Hydrochloride 210319 Pi RMB 02Document12 pagesAuspar Labetalol Hydrochloride 210319 Pi RMB 02Adel SalehNo ratings yet
- BenzodiazepinesDocument6 pagesBenzodiazepinesRoman MamunNo ratings yet
- Alpha Blockers PharmacologyDocument23 pagesAlpha Blockers PharmacologyHesbon MomanyiNo ratings yet
- Atenolol: Atenolol Is A Beta Blocker MedicationDocument6 pagesAtenolol: Atenolol Is A Beta Blocker MedicationAbdelrhman AboodaNo ratings yet
- Beta Blockers-Wps OfficeDocument6 pagesBeta Blockers-Wps OfficeCamelle DiniayNo ratings yet
- Pharmacology Cardiovascular DrugsDocument120 pagesPharmacology Cardiovascular DrugsDareRaymond100% (1)
- Antiadrenergic Drugs - II 24.07.018 PDFDocument25 pagesAntiadrenergic Drugs - II 24.07.018 PDFHitesh karnNo ratings yet
- Hypertension: Increase in Blood PressureDocument29 pagesHypertension: Increase in Blood PressureKeesha Mae AnteNo ratings yet
- Adrenergic Blockers by Ms. MaidaDocument23 pagesAdrenergic Blockers by Ms. MaidaShimmering MoonNo ratings yet
- BETA BlockerDocument4 pagesBETA BlockerHasrul MuslihNo ratings yet
- A Review On Atenolol: Volume 9, Issue 3, 902-914 Review Article ISSN 2278 - 4357Document13 pagesA Review On Atenolol: Volume 9, Issue 3, 902-914 Review Article ISSN 2278 - 4357SitiHawa SomadayoNo ratings yet
- Major Side Effects of Beta Blockers - UpToDateDocument22 pagesMajor Side Effects of Beta Blockers - UpToDateJoão VictorNo ratings yet
- Pha051 Las#8 RationaleDocument25 pagesPha051 Las#8 RationaleMonique EamiguelNo ratings yet
- Sympa T Holy TicsDocument30 pagesSympa T Holy TicsAhaisibwe GordonNo ratings yet
- 6 Beta Adrenergic BlockersDocument19 pages6 Beta Adrenergic Blockersmatchees-gone rogue100% (1)
- Butisol Sodium: (Butabarbital Sodium Tablets, USP and Butabarbital Sodium Oral Solution, USP) Tablets & Oral SolutionDocument5 pagesButisol Sodium: (Butabarbital Sodium Tablets, USP and Butabarbital Sodium Oral Solution, USP) Tablets & Oral SolutionBrian HarrisNo ratings yet
- LI Case 2 (Pharmacological Properties of Propanolol)Document2 pagesLI Case 2 (Pharmacological Properties of Propanolol)adtyadaviaNo ratings yet
- Beta Blocker Poisoning - UpToDateDocument16 pagesBeta Blocker Poisoning - UpToDatehatsuneNo ratings yet
- BISOPROLOLDocument4 pagesBISOPROLOLHY Hong YiNo ratings yet
- TriptololDocument5 pagesTriptololMohan PrasadNo ratings yet
- Adrenoceptor BlockersDocument53 pagesAdrenoceptor Blockersesra1altahirNo ratings yet
- Drugs Acting On Respiratory System of AnimalsDocument8 pagesDrugs Acting On Respiratory System of AnimalsSunil100% (4)
- AuditDocument10 pagesAuditrheyasrNo ratings yet
- Adrenergic Antagonists Adrenoreceptor Blockers 2: September 2019Document30 pagesAdrenergic Antagonists Adrenoreceptor Blockers 2: September 2019Rohullah QasimiNo ratings yet
- Adrenergic AntagonistsDocument23 pagesAdrenergic AntagonistsMirza Shaharyar BaigNo ratings yet
- SY - Medichem I - Adrenergic BlockersDocument38 pagesSY - Medichem I - Adrenergic BlockersKevalNo ratings yet
- 5 Adrenoceptor BlockersDocument52 pages5 Adrenoceptor BlockersHamid Hussain HamidNo ratings yet
- CH 19Document15 pagesCH 19Emmanuel GaliciaNo ratings yet
- β - BlockersDocument12 pagesβ - Blockersmohavi8169No ratings yet
- Labetalol: Review of Pharmacology, Pharmacokinetics, Clinical Uses and Adverse EffectsDocument25 pagesLabetalol: Review of Pharmacology, Pharmacokinetics, Clinical Uses and Adverse EffectsPham TrucNo ratings yet
- Pharma Midterm Review 1Document49 pagesPharma Midterm Review 1aujrcbanayadshiela11stem1aNo ratings yet
- methotrexate-Anti-Asthmatic Drugs Toxicity-1Document9 pagesmethotrexate-Anti-Asthmatic Drugs Toxicity-1joonabil29No ratings yet
- Clinical Cardiology - September 1996 - Stewart - Systemic Side Effects of Topical Beta Adrenergic BlockersDocument7 pagesClinical Cardiology - September 1996 - Stewart - Systemic Side Effects of Topical Beta Adrenergic BlockersamanabduwahabNo ratings yet
- Salbu IpaDocument2 pagesSalbu IpaGwyn RosalesNo ratings yet
- Adrenoreceptor Antagonist DrugsDocument19 pagesAdrenoreceptor Antagonist DrugsAassh DcmbrNo ratings yet
- PropranololDocument6 pagesPropranololanon_678895677No ratings yet
- Stoeltings Pharmacology TextbookDocument10 pagesStoeltings Pharmacology Textbookkarenmr013No ratings yet
- Anoro Ellipta Pi MGDocument35 pagesAnoro Ellipta Pi MGAgusJiethoSfarmAptNo ratings yet
- Antinauseants and AntiemeticsDocument8 pagesAntinauseants and AntiemeticsHamad AlshabiNo ratings yet
- Beta Blockers in HTNDocument69 pagesBeta Blockers in HTNMohammad Sadiq AzamNo ratings yet
- Curs 8 - Antagonisti Selectivi Beta 1 AdrenergiciDocument1 pageCurs 8 - Antagonisti Selectivi Beta 1 AdrenergiciAnamaria RusuNo ratings yet
- Diagnosing Wound Infection The Use of C Reactive Protein 1Document9 pagesDiagnosing Wound Infection The Use of C Reactive Protein 1Raj BalasubramaniamNo ratings yet
- Product: A Product Is Anything That Can Be Offered To A Market To Satisfy A Want or NeedDocument12 pagesProduct: A Product Is Anything That Can Be Offered To A Market To Satisfy A Want or NeedSumon Das DasNo ratings yet
- 6 - Breath SoundsDocument31 pages6 - Breath SoundsggNo ratings yet
- Effective Rejuvenation With Hyaluronic Acid Fillers: Current Advanced ConceptsDocument13 pagesEffective Rejuvenation With Hyaluronic Acid Fillers: Current Advanced ConceptsCamila De Lizier MesquitaNo ratings yet
- MindfulnessDocument30 pagesMindfulnessYetro ValentinoNo ratings yet
- CAPE Communication Studies 2009 P3BDocument4 pagesCAPE Communication Studies 2009 P3BRiaz JokanNo ratings yet
- Benefits of Living DonationDocument1 pageBenefits of Living DonationRanga RajanNo ratings yet
- Body Systems Lecture NotesDocument10 pagesBody Systems Lecture Notesapi-377297552No ratings yet
- Cannabis Legal Regulatory Update April June 2019Document19 pagesCannabis Legal Regulatory Update April June 2019stonerhinoNo ratings yet
- Ordinance #1. BESUDocument4 pagesOrdinance #1. BESUHana Navalta Soberano100% (3)
- Alamillo Vs Cleene Maritime PPDocument27 pagesAlamillo Vs Cleene Maritime PPHeart LeroNo ratings yet
- SHS Hope IvDocument4 pagesSHS Hope IvMacapagal Andrea Nicole DayritNo ratings yet
- The Evolution of A Different Voice in Family Therapy: Conversation Between Lynn Hoffman and Darryl WheatDocument12 pagesThe Evolution of A Different Voice in Family Therapy: Conversation Between Lynn Hoffman and Darryl WheatMaNo ratings yet
- Disability and Life Writing: Reports From The Nineteenth-Century AsylumDocument19 pagesDisability and Life Writing: Reports From The Nineteenth-Century AsylumHS22D001 MalavikaNo ratings yet
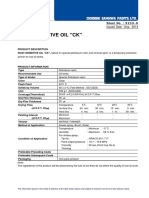
- 8250 RUST INHIBITIVE OIL CK Rev (1409) PDFDocument2 pages8250 RUST INHIBITIVE OIL CK Rev (1409) PDFTrịnh Minh KhoaNo ratings yet
- Hse Training MatrixDocument3 pagesHse Training Matrixjoenediath9345No ratings yet
- Prevalence of Undernutrition and Effectiveness of A Community Based Nutritional Support Programme To Reverse Stunting Among Children Under Five YearsDocument8 pagesPrevalence of Undernutrition and Effectiveness of A Community Based Nutritional Support Programme To Reverse Stunting Among Children Under Five YearsEusabia LiansianiNo ratings yet
- Jennifer CarrollCV09 21Document22 pagesJennifer CarrollCV09 21Jen CarrollNo ratings yet
- Neuroscience and Biobehavioral Reviews: Janne C. Visser, Nanda N.J. Rommelse, Corina U. Greven, Jan K. BuitelaarDocument35 pagesNeuroscience and Biobehavioral Reviews: Janne C. Visser, Nanda N.J. Rommelse, Corina U. Greven, Jan K. BuitelaarCristinaNo ratings yet
- Articulo en Ingles CARILLAS EN DISILICATODocument14 pagesArticulo en Ingles CARILLAS EN DISILICATOISABELANo ratings yet
- Journal Sit and Reach MeasurementDocument3 pagesJournal Sit and Reach MeasurementfricaNo ratings yet
- UG - Workshop Manufacturing Practices - EnglishDocument23 pagesUG - Workshop Manufacturing Practices - EnglishKhalidNo ratings yet
- Class 12 Physical Education Half-Yearly Paper 2021-22Document15 pagesClass 12 Physical Education Half-Yearly Paper 2021-22Gamer ZoneNo ratings yet
- Chapter 1 The Human OrganismDocument18 pagesChapter 1 The Human OrganismEuniece AnicocheNo ratings yet
- CPR Salbutamol+Ipratropium Neb (BRODIX PLUS) 35'sDocument2 pagesCPR Salbutamol+Ipratropium Neb (BRODIX PLUS) 35'sRacquel SolivenNo ratings yet
- PB Nuflow REV03Document2 pagesPB Nuflow REV03metech8xNo ratings yet
- Management Is Nothing More Than Motivating Other People GHEORGHE MDocument6 pagesManagement Is Nothing More Than Motivating Other People GHEORGHE MCristina PaliuNo ratings yet
- Curing of MeatDocument32 pagesCuring of MeatRai Sajid LatifNo ratings yet