
Quick Reference Guide Endocrine Hypertension 2 2016 Version
Quick Reference Guide Endocrine Hypertension 2 2016 Version
You might also like
- Pa 1 Persuasive EssayDocument4 pagesPa 1 Persuasive Essayapi-458023500No ratings yet
- E773 FullDocument6 pagesE773 FullanhiramdhaniNo ratings yet
- Aldosteronismo PrimarioDocument23 pagesAldosteronismo PrimarioLuisNo ratings yet
- Joim 12831 PDFDocument23 pagesJoim 12831 PDFnurhidayahNo ratings yet
- Hypertensive EmergencyDocument4 pagesHypertensive EmergencyRara MuuztmuuztmuccuNo ratings yet
- Astra End HipDocument47 pagesAstra End HipIlze KonrādeNo ratings yet
- Evaluationandmanagement Ofprimary Hyperaldosteronism: Frances T. Lee,, Dina ElarajDocument15 pagesEvaluationandmanagement Ofprimary Hyperaldosteronism: Frances T. Lee,, Dina ElarajDiego BallesterosNo ratings yet
- Ardhanari 2015Document11 pagesArdhanari 2015Vivi DeviyanaNo ratings yet
- Primary Hyperaldosteronism - StatPearls - NCBI BookshelfDocument7 pagesPrimary Hyperaldosteronism - StatPearls - NCBI BookshelfCecil-An DalanonNo ratings yet
- Manchester Presentation Final 2Document21 pagesManchester Presentation Final 2api-610233914No ratings yet
- Stopp Start ToolkitDocument22 pagesStopp Start ToolkitRifky IlhamiNo ratings yet
- Crisis HipertensivasDocument17 pagesCrisis HipertensivasJuan C. Moreno BarraganNo ratings yet
- Antihypertensive DrugsDocument52 pagesAntihypertensive Drugsapi-224264169No ratings yet
- 1 Dental Management of Patients With Cardiovascular DiseasesDocument14 pages1 Dental Management of Patients With Cardiovascular Diseasesاحمد سلامNo ratings yet
- HypertensionDocument10 pagesHypertensionaa zzNo ratings yet
- HypertensionDocument5 pagesHypertensiongoinggreen91No ratings yet
- Jama Hta ResistenteDocument9 pagesJama Hta ResistenteMayra Alejandra Prada SerranoNo ratings yet
- Diagnosis and Treatment of Primary AldosteronismDocument17 pagesDiagnosis and Treatment of Primary AldosteronismcastillojessNo ratings yet
- Articles: Spironolactone Management of Resistant HypertensionDocument8 pagesArticles: Spironolactone Management of Resistant HypertensionKatherine America Camac DelgadoNo ratings yet
- HTN EmergenciesDocument7 pagesHTN EmergenciesBarry Tumpal Wouter NapitupuluNo ratings yet
- سريرية نظري٢Document12 pagesسريرية نظري٢مصطفى ابراهيم سعيدNo ratings yet
- 5 HypertensionDocument8 pages5 Hypertensioniraqeana100100No ratings yet
- Managing Hyperkalemia Caused by Inhibitors of The Renin-Angiotensin-Aldosterone SystemDocument8 pagesManaging Hyperkalemia Caused by Inhibitors of The Renin-Angiotensin-Aldosterone SystemMedranoReyesLuisinNo ratings yet
- Ferne HTN Emerg Feldstein 2007 PDFDocument5 pagesFerne HTN Emerg Feldstein 2007 PDFridwan020392No ratings yet
- Case StudiesDocument5 pagesCase Studiespragna novaNo ratings yet
- Hypertension Definition:: Nitric OxideDocument5 pagesHypertension Definition:: Nitric OxideAnonymous bbeAZHxZNo ratings yet
- Drug Treatment For Hypertensive Emergencies: New Concepts and Emerging Technologies For Emergency PhysiciansDocument0 pagesDrug Treatment For Hypertensive Emergencies: New Concepts and Emerging Technologies For Emergency PhysiciansRajihah JihahNo ratings yet
- Flashcards - QuizletDocument7 pagesFlashcards - QuizletNEsreNo ratings yet
- DBP: Diastolic Blood Pressure SBP: Systolic Blood PressureDocument7 pagesDBP: Diastolic Blood Pressure SBP: Systolic Blood PressureM. JoyceNo ratings yet
- Essential Hypertension Review - USMLE Step 2Document26 pagesEssential Hypertension Review - USMLE Step 2Marc Imhotep Cray, M.D.No ratings yet
- Why Hard To Control Blood Pressure ?: Atma GunawanDocument35 pagesWhy Hard To Control Blood Pressure ?: Atma GunawanLies Pramana SariNo ratings yet
- Anesthetic Management in Conn's Syndrome and PheochromocytomaDocument35 pagesAnesthetic Management in Conn's Syndrome and PheochromocytomaShashikant RamNo ratings yet
- Acquired TTP - Clinical Manifestations and Diagnosis - UpToDateDocument16 pagesAcquired TTP - Clinical Manifestations and Diagnosis - UpToDatepradeep danielNo ratings yet
- Hyperkalemia in Heart Failure: The Present and FutureDocument15 pagesHyperkalemia in Heart Failure: The Present and FutureLizette Galvan GalvanNo ratings yet
- High Yield Board ReviewDocument5 pagesHigh Yield Board ReviewMarcoNo ratings yet
- Lec 3Document13 pagesLec 3fbbqbcht6yNo ratings yet
- HypertensionDocument55 pagesHypertensionSr.Jyothy SABSNo ratings yet
- Sodium Disorders AAFP PDFDocument12 pagesSodium Disorders AAFP PDFIvan Tintaya UrureNo ratings yet
- Hypertensiveemergencies PDFDocument7 pagesHypertensiveemergencies PDFGede AdiNo ratings yet
- Drug Induced Hyperuricemia GoutDocument3 pagesDrug Induced Hyperuricemia GoutAnggun Cahya MertyanaNo ratings yet
- Acute Heart FailureDocument24 pagesAcute Heart FailureTeddy MauriceNo ratings yet
- Diagnostic Tests and ProceduresDocument49 pagesDiagnostic Tests and Procedurespmahi8854No ratings yet
- WJH 5 14Document15 pagesWJH 5 14Elena Borş MorariNo ratings yet
- Art 40Document4 pagesArt 40Francesca BertaccaNo ratings yet
- Farmacos de Hta en EmbarazoDocument5 pagesFarmacos de Hta en EmbarazoДжек ХавокNo ratings yet
- Cardiac Medication LectureDocument23 pagesCardiac Medication LectureilikeedsheeranNo ratings yet
- CVS (HF, HTN) PharmacologyDocument99 pagesCVS (HF, HTN) PharmacologyCherenet TomaNo ratings yet
- Hypertension: 1-Hypertension Is Defined As (BP)Document37 pagesHypertension: 1-Hypertension Is Defined As (BP)hussein alnasryNo ratings yet
- Crisis Hipertensiva CHEST 2007 PDFDocument16 pagesCrisis Hipertensiva CHEST 2007 PDFJenny AlexandraNo ratings yet
- Hypertensive CrisisDocument60 pagesHypertensive CrisisDzikrul Haq KarimullahNo ratings yet
- OmapatrilatDocument3 pagesOmapatrilataislineazpeitia23No ratings yet
- Reviews: Novel Therapeutic Targets For HypertensionDocument11 pagesReviews: Novel Therapeutic Targets For HypertensiongpatwallahNo ratings yet
- LAS 4 Drugs For HypertensionDocument28 pagesLAS 4 Drugs For HypertensionMuhammad Haroon RazaNo ratings yet
- Contraindications To Vasoconstrictors in Dentistry: Part IIDocument5 pagesContraindications To Vasoconstrictors in Dentistry: Part IIBunga Erlita RosaliaNo ratings yet
- Hiperkalemia en ERDocument8 pagesHiperkalemia en ERmjbb1310No ratings yet
- Hyperkalemia Management in The Emergency Department: An Expert Panel ConsensusDocument8 pagesHyperkalemia Management in The Emergency Department: An Expert Panel ConsensusDaniel HeSaNo ratings yet
- Critical Care Medications: Vasopressors, Inotropes and Anti-Hypertensives Study Guide: Critical Care EssentialsFrom EverandCritical Care Medications: Vasopressors, Inotropes and Anti-Hypertensives Study Guide: Critical Care EssentialsNo ratings yet
- Hypotensive Syndromes in Geriatric PatientsFrom EverandHypotensive Syndromes in Geriatric PatientsKannayiram AlagiakrishnanNo ratings yet
- Secondary Hypertension: Clinical Presentation, Diagnosis, and TreatmentFrom EverandSecondary Hypertension: Clinical Presentation, Diagnosis, and TreatmentGeorge A. MansoorNo ratings yet
- Conn Syndrome, (Hyper-Aldosteronism) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandConn Syndrome, (Hyper-Aldosteronism) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- 976c5091-5277-4d13-8655-371a2eb3d13fDocument2 pages976c5091-5277-4d13-8655-371a2eb3d13fParishan SaeedNo ratings yet
- Bone Age For Chronological Age Determination - November2018Document4 pagesBone Age For Chronological Age Determination - November2018Parishan SaeedNo ratings yet
- 1 s2.0 S0009912017307178 MainDocument23 pages1 s2.0 S0009912017307178 MainParishan SaeedNo ratings yet
- Decreased Ligand Affinity Rather Than Glucocorticoid Receptor Down-Regulation in Patients With Endogenous Cushing's SyndromeDocument5 pagesDecreased Ligand Affinity Rather Than Glucocorticoid Receptor Down-Regulation in Patients With Endogenous Cushing's SyndromeParishan SaeedNo ratings yet
- Effect of Knowledge of Chronologic Age On The Variability of Pediatric Bone Age Determined Using The Greulich and Pyle StandardsDocument7 pagesEffect of Knowledge of Chronologic Age On The Variability of Pediatric Bone Age Determined Using The Greulich and Pyle StandardsParishan SaeedNo ratings yet
- Cortisol II 2020-03 v6Document5 pagesCortisol II 2020-03 v6Parishan SaeedNo ratings yet
- Guidance Statement: Hormone Supplementation For Pubertal Induction in GirlsDocument21 pagesGuidance Statement: Hormone Supplementation For Pubertal Induction in GirlsParishan SaeedNo ratings yet
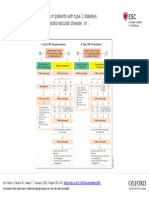
- Guideline Treatment of T2DM 2020 ESCDocument1 pageGuideline Treatment of T2DM 2020 ESCParishan SaeedNo ratings yet
- Ece Home 2023 Paag DDocument1 pageEce Home 2023 Paag DParishan SaeedNo ratings yet
- See Full Prescribing Information For Complete Boxed WarningDocument43 pagesSee Full Prescribing Information For Complete Boxed WarningParishan SaeedNo ratings yet
- Glp-1 Receptor Agonists (GLP-1 RA) : Presented By: Nermeen S. Esa (Clinical Pharmacist)Document10 pagesGlp-1 Receptor Agonists (GLP-1 RA) : Presented By: Nermeen S. Esa (Clinical Pharmacist)Parishan SaeedNo ratings yet
- COVID-19 Disease SeverityDocument7 pagesCOVID-19 Disease SeverityParishan SaeedNo ratings yet
- Junior Grade 9 Junior Grade 9Document2 pagesJunior Grade 9 Junior Grade 9Mark Joseph Nepomuceno CometaNo ratings yet
- Neonatal Meningitis: Designed By: Dr. Esraa AlnabilsyDocument19 pagesNeonatal Meningitis: Designed By: Dr. Esraa AlnabilsyAli FalihNo ratings yet
- List of Basic Essential Medicines Ministry of Health Seychelles 2010Document14 pagesList of Basic Essential Medicines Ministry of Health Seychelles 2010portosinNo ratings yet
- Neurology Clerkship UWORLD: Brain TumoursDocument13 pagesNeurology Clerkship UWORLD: Brain TumoursHaadi AliNo ratings yet
- Drugs Influencing Internal Organs Part2Document92 pagesDrugs Influencing Internal Organs Part2Jemi LoriNo ratings yet
- 4 Sitagliptin (Raysiglip)Document200 pages4 Sitagliptin (Raysiglip)Thet Su LwinNo ratings yet
- Polycythemia VeraDocument33 pagesPolycythemia VeramesseeeNo ratings yet
- Loresca - Ratio Mtle - HistopathDocument10 pagesLoresca - Ratio Mtle - HistopathKaycee Gretz LorescaNo ratings yet
- Kawasaki Disease-NcpDocument5 pagesKawasaki Disease-NcpBelen SoleroNo ratings yet
- Muthu HT ReportDocument87 pagesMuthu HT ReportSridharan DNo ratings yet
- Cerebrospinal Fluid - AUBFDocument9 pagesCerebrospinal Fluid - AUBFMitch IbayNo ratings yet
- Medical Diseases in PregnancyDocument37 pagesMedical Diseases in PregnancyAsteway MesfinNo ratings yet
- FMGE JUNE-2109 Questions: AriseDocument20 pagesFMGE JUNE-2109 Questions: AriseSugithaTamilarasanNo ratings yet
- 5 6280832050500993149Document77 pages5 6280832050500993149Nitish AggarwalNo ratings yet
- Clinical Insights: Dr. Wathik M. Thijar MBBCH, Febm, Mrcp-Uk Lecturer of Internal MedicineDocument20 pagesClinical Insights: Dr. Wathik M. Thijar MBBCH, Febm, Mrcp-Uk Lecturer of Internal MedicineYousif AlaaNo ratings yet
- Pancreatic Ductal Adenocarcinoma and Its Variants: Pearls and PerilsDocument20 pagesPancreatic Ductal Adenocarcinoma and Its Variants: Pearls and PerilsGeorge MogaNo ratings yet
- Kode Pintar Icd 10Document60 pagesKode Pintar Icd 10Nur LailaNo ratings yet
- CLIN CHEM: Nonprotein Nitrogen Compounds (NPN) : Topic Outline Urea Uric AcidDocument7 pagesCLIN CHEM: Nonprotein Nitrogen Compounds (NPN) : Topic Outline Urea Uric AcidJezzah Mae CañeteNo ratings yet
- Abnormal PsychologyDocument136 pagesAbnormal PsychologyMary Ye Ariola Magsino100% (3)
- NCM 112 E LEARNING AutosavedDocument7 pagesNCM 112 E LEARNING AutosavedMikko McDonie VeloriaNo ratings yet
- Manual Urinalysis: Lynne PowellDocument37 pagesManual Urinalysis: Lynne PowellAdhya TiaraNo ratings yet
- Anatomy of Human EyeDocument41 pagesAnatomy of Human EyeCarly MelachioNo ratings yet
- Immuno-Serology: Antistreptolysin 0Document13 pagesImmuno-Serology: Antistreptolysin 0Romie SolacitoNo ratings yet
- BLOCK II LMS Quiz AnatomyDocument27 pagesBLOCK II LMS Quiz AnatomyAshley BuchananNo ratings yet
- High Yield Psychiatry: Shelf Exam Review Emma Holliday RamahiDocument71 pagesHigh Yield Psychiatry: Shelf Exam Review Emma Holliday RamahisamNo ratings yet
- Background of The StudyDocument7 pagesBackground of The StudyVern LeStrangeNo ratings yet
- Study Guid Patho 1Document41 pagesStudy Guid Patho 1sturner7887No ratings yet
- Alzheimer Disease EngDocument35 pagesAlzheimer Disease EngAna IantucNo ratings yet
- Basic Brain AnatomyDocument36 pagesBasic Brain Anatomymartha wibawaNo ratings yet




































































































Download as pdf or txt
You might also like
- Pa 1 Persuasive EssayDocument4 pagesPa 1 Persuasive Essayapi-458023500No ratings yet
- E773 FullDocument6 pagesE773 FullanhiramdhaniNo ratings yet
- Aldosteronismo PrimarioDocument23 pagesAldosteronismo PrimarioLuisNo ratings yet
- Joim 12831 PDFDocument23 pagesJoim 12831 PDFnurhidayahNo ratings yet
- Hypertensive EmergencyDocument4 pagesHypertensive EmergencyRara MuuztmuuztmuccuNo ratings yet
- Astra End HipDocument47 pagesAstra End HipIlze KonrādeNo ratings yet
- Evaluationandmanagement Ofprimary Hyperaldosteronism: Frances T. Lee,, Dina ElarajDocument15 pagesEvaluationandmanagement Ofprimary Hyperaldosteronism: Frances T. Lee,, Dina ElarajDiego BallesterosNo ratings yet
- Ardhanari 2015Document11 pagesArdhanari 2015Vivi DeviyanaNo ratings yet
- Primary Hyperaldosteronism - StatPearls - NCBI BookshelfDocument7 pagesPrimary Hyperaldosteronism - StatPearls - NCBI BookshelfCecil-An DalanonNo ratings yet
- Manchester Presentation Final 2Document21 pagesManchester Presentation Final 2api-610233914No ratings yet
- Stopp Start ToolkitDocument22 pagesStopp Start ToolkitRifky IlhamiNo ratings yet
- Crisis HipertensivasDocument17 pagesCrisis HipertensivasJuan C. Moreno BarraganNo ratings yet
- Antihypertensive DrugsDocument52 pagesAntihypertensive Drugsapi-224264169No ratings yet
- 1 Dental Management of Patients With Cardiovascular DiseasesDocument14 pages1 Dental Management of Patients With Cardiovascular Diseasesاحمد سلامNo ratings yet
- HypertensionDocument10 pagesHypertensionaa zzNo ratings yet
- HypertensionDocument5 pagesHypertensiongoinggreen91No ratings yet
- Jama Hta ResistenteDocument9 pagesJama Hta ResistenteMayra Alejandra Prada SerranoNo ratings yet
- Diagnosis and Treatment of Primary AldosteronismDocument17 pagesDiagnosis and Treatment of Primary AldosteronismcastillojessNo ratings yet
- Articles: Spironolactone Management of Resistant HypertensionDocument8 pagesArticles: Spironolactone Management of Resistant HypertensionKatherine America Camac DelgadoNo ratings yet
- HTN EmergenciesDocument7 pagesHTN EmergenciesBarry Tumpal Wouter NapitupuluNo ratings yet
- سريرية نظري٢Document12 pagesسريرية نظري٢مصطفى ابراهيم سعيدNo ratings yet
- 5 HypertensionDocument8 pages5 Hypertensioniraqeana100100No ratings yet
- Managing Hyperkalemia Caused by Inhibitors of The Renin-Angiotensin-Aldosterone SystemDocument8 pagesManaging Hyperkalemia Caused by Inhibitors of The Renin-Angiotensin-Aldosterone SystemMedranoReyesLuisinNo ratings yet
- Ferne HTN Emerg Feldstein 2007 PDFDocument5 pagesFerne HTN Emerg Feldstein 2007 PDFridwan020392No ratings yet
- Case StudiesDocument5 pagesCase Studiespragna novaNo ratings yet
- Hypertension Definition:: Nitric OxideDocument5 pagesHypertension Definition:: Nitric OxideAnonymous bbeAZHxZNo ratings yet
- Drug Treatment For Hypertensive Emergencies: New Concepts and Emerging Technologies For Emergency PhysiciansDocument0 pagesDrug Treatment For Hypertensive Emergencies: New Concepts and Emerging Technologies For Emergency PhysiciansRajihah JihahNo ratings yet
- Flashcards - QuizletDocument7 pagesFlashcards - QuizletNEsreNo ratings yet
- DBP: Diastolic Blood Pressure SBP: Systolic Blood PressureDocument7 pagesDBP: Diastolic Blood Pressure SBP: Systolic Blood PressureM. JoyceNo ratings yet
- Essential Hypertension Review - USMLE Step 2Document26 pagesEssential Hypertension Review - USMLE Step 2Marc Imhotep Cray, M.D.No ratings yet
- Why Hard To Control Blood Pressure ?: Atma GunawanDocument35 pagesWhy Hard To Control Blood Pressure ?: Atma GunawanLies Pramana SariNo ratings yet
- Anesthetic Management in Conn's Syndrome and PheochromocytomaDocument35 pagesAnesthetic Management in Conn's Syndrome and PheochromocytomaShashikant RamNo ratings yet
- Acquired TTP - Clinical Manifestations and Diagnosis - UpToDateDocument16 pagesAcquired TTP - Clinical Manifestations and Diagnosis - UpToDatepradeep danielNo ratings yet
- Hyperkalemia in Heart Failure: The Present and FutureDocument15 pagesHyperkalemia in Heart Failure: The Present and FutureLizette Galvan GalvanNo ratings yet
- High Yield Board ReviewDocument5 pagesHigh Yield Board ReviewMarcoNo ratings yet
- Lec 3Document13 pagesLec 3fbbqbcht6yNo ratings yet
- HypertensionDocument55 pagesHypertensionSr.Jyothy SABSNo ratings yet
- Sodium Disorders AAFP PDFDocument12 pagesSodium Disorders AAFP PDFIvan Tintaya UrureNo ratings yet
- Hypertensiveemergencies PDFDocument7 pagesHypertensiveemergencies PDFGede AdiNo ratings yet
- Drug Induced Hyperuricemia GoutDocument3 pagesDrug Induced Hyperuricemia GoutAnggun Cahya MertyanaNo ratings yet
- Acute Heart FailureDocument24 pagesAcute Heart FailureTeddy MauriceNo ratings yet
- Diagnostic Tests and ProceduresDocument49 pagesDiagnostic Tests and Procedurespmahi8854No ratings yet
- WJH 5 14Document15 pagesWJH 5 14Elena Borş MorariNo ratings yet
- Art 40Document4 pagesArt 40Francesca BertaccaNo ratings yet
- Farmacos de Hta en EmbarazoDocument5 pagesFarmacos de Hta en EmbarazoДжек ХавокNo ratings yet
- Cardiac Medication LectureDocument23 pagesCardiac Medication LectureilikeedsheeranNo ratings yet
- CVS (HF, HTN) PharmacologyDocument99 pagesCVS (HF, HTN) PharmacologyCherenet TomaNo ratings yet
- Hypertension: 1-Hypertension Is Defined As (BP)Document37 pagesHypertension: 1-Hypertension Is Defined As (BP)hussein alnasryNo ratings yet
- Crisis Hipertensiva CHEST 2007 PDFDocument16 pagesCrisis Hipertensiva CHEST 2007 PDFJenny AlexandraNo ratings yet
- Hypertensive CrisisDocument60 pagesHypertensive CrisisDzikrul Haq KarimullahNo ratings yet
- OmapatrilatDocument3 pagesOmapatrilataislineazpeitia23No ratings yet
- Reviews: Novel Therapeutic Targets For HypertensionDocument11 pagesReviews: Novel Therapeutic Targets For HypertensiongpatwallahNo ratings yet
- LAS 4 Drugs For HypertensionDocument28 pagesLAS 4 Drugs For HypertensionMuhammad Haroon RazaNo ratings yet
- Contraindications To Vasoconstrictors in Dentistry: Part IIDocument5 pagesContraindications To Vasoconstrictors in Dentistry: Part IIBunga Erlita RosaliaNo ratings yet
- Hiperkalemia en ERDocument8 pagesHiperkalemia en ERmjbb1310No ratings yet
- Hyperkalemia Management in The Emergency Department: An Expert Panel ConsensusDocument8 pagesHyperkalemia Management in The Emergency Department: An Expert Panel ConsensusDaniel HeSaNo ratings yet
- Critical Care Medications: Vasopressors, Inotropes and Anti-Hypertensives Study Guide: Critical Care EssentialsFrom EverandCritical Care Medications: Vasopressors, Inotropes and Anti-Hypertensives Study Guide: Critical Care EssentialsNo ratings yet
- Hypotensive Syndromes in Geriatric PatientsFrom EverandHypotensive Syndromes in Geriatric PatientsKannayiram AlagiakrishnanNo ratings yet
- Secondary Hypertension: Clinical Presentation, Diagnosis, and TreatmentFrom EverandSecondary Hypertension: Clinical Presentation, Diagnosis, and TreatmentGeorge A. MansoorNo ratings yet
- Conn Syndrome, (Hyper-Aldosteronism) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandConn Syndrome, (Hyper-Aldosteronism) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- 976c5091-5277-4d13-8655-371a2eb3d13fDocument2 pages976c5091-5277-4d13-8655-371a2eb3d13fParishan SaeedNo ratings yet
- Bone Age For Chronological Age Determination - November2018Document4 pagesBone Age For Chronological Age Determination - November2018Parishan SaeedNo ratings yet
- 1 s2.0 S0009912017307178 MainDocument23 pages1 s2.0 S0009912017307178 MainParishan SaeedNo ratings yet
- Decreased Ligand Affinity Rather Than Glucocorticoid Receptor Down-Regulation in Patients With Endogenous Cushing's SyndromeDocument5 pagesDecreased Ligand Affinity Rather Than Glucocorticoid Receptor Down-Regulation in Patients With Endogenous Cushing's SyndromeParishan SaeedNo ratings yet
- Effect of Knowledge of Chronologic Age On The Variability of Pediatric Bone Age Determined Using The Greulich and Pyle StandardsDocument7 pagesEffect of Knowledge of Chronologic Age On The Variability of Pediatric Bone Age Determined Using The Greulich and Pyle StandardsParishan SaeedNo ratings yet
- Cortisol II 2020-03 v6Document5 pagesCortisol II 2020-03 v6Parishan SaeedNo ratings yet
- Guidance Statement: Hormone Supplementation For Pubertal Induction in GirlsDocument21 pagesGuidance Statement: Hormone Supplementation For Pubertal Induction in GirlsParishan SaeedNo ratings yet
- Guideline Treatment of T2DM 2020 ESCDocument1 pageGuideline Treatment of T2DM 2020 ESCParishan SaeedNo ratings yet
- Ece Home 2023 Paag DDocument1 pageEce Home 2023 Paag DParishan SaeedNo ratings yet
- See Full Prescribing Information For Complete Boxed WarningDocument43 pagesSee Full Prescribing Information For Complete Boxed WarningParishan SaeedNo ratings yet
- Glp-1 Receptor Agonists (GLP-1 RA) : Presented By: Nermeen S. Esa (Clinical Pharmacist)Document10 pagesGlp-1 Receptor Agonists (GLP-1 RA) : Presented By: Nermeen S. Esa (Clinical Pharmacist)Parishan SaeedNo ratings yet
- COVID-19 Disease SeverityDocument7 pagesCOVID-19 Disease SeverityParishan SaeedNo ratings yet
- Junior Grade 9 Junior Grade 9Document2 pagesJunior Grade 9 Junior Grade 9Mark Joseph Nepomuceno CometaNo ratings yet
- Neonatal Meningitis: Designed By: Dr. Esraa AlnabilsyDocument19 pagesNeonatal Meningitis: Designed By: Dr. Esraa AlnabilsyAli FalihNo ratings yet
- List of Basic Essential Medicines Ministry of Health Seychelles 2010Document14 pagesList of Basic Essential Medicines Ministry of Health Seychelles 2010portosinNo ratings yet
- Neurology Clerkship UWORLD: Brain TumoursDocument13 pagesNeurology Clerkship UWORLD: Brain TumoursHaadi AliNo ratings yet
- Drugs Influencing Internal Organs Part2Document92 pagesDrugs Influencing Internal Organs Part2Jemi LoriNo ratings yet
- 4 Sitagliptin (Raysiglip)Document200 pages4 Sitagliptin (Raysiglip)Thet Su LwinNo ratings yet
- Polycythemia VeraDocument33 pagesPolycythemia VeramesseeeNo ratings yet
- Loresca - Ratio Mtle - HistopathDocument10 pagesLoresca - Ratio Mtle - HistopathKaycee Gretz LorescaNo ratings yet
- Kawasaki Disease-NcpDocument5 pagesKawasaki Disease-NcpBelen SoleroNo ratings yet
- Muthu HT ReportDocument87 pagesMuthu HT ReportSridharan DNo ratings yet
- Cerebrospinal Fluid - AUBFDocument9 pagesCerebrospinal Fluid - AUBFMitch IbayNo ratings yet
- Medical Diseases in PregnancyDocument37 pagesMedical Diseases in PregnancyAsteway MesfinNo ratings yet
- FMGE JUNE-2109 Questions: AriseDocument20 pagesFMGE JUNE-2109 Questions: AriseSugithaTamilarasanNo ratings yet
- 5 6280832050500993149Document77 pages5 6280832050500993149Nitish AggarwalNo ratings yet
- Clinical Insights: Dr. Wathik M. Thijar MBBCH, Febm, Mrcp-Uk Lecturer of Internal MedicineDocument20 pagesClinical Insights: Dr. Wathik M. Thijar MBBCH, Febm, Mrcp-Uk Lecturer of Internal MedicineYousif AlaaNo ratings yet
- Pancreatic Ductal Adenocarcinoma and Its Variants: Pearls and PerilsDocument20 pagesPancreatic Ductal Adenocarcinoma and Its Variants: Pearls and PerilsGeorge MogaNo ratings yet
- Kode Pintar Icd 10Document60 pagesKode Pintar Icd 10Nur LailaNo ratings yet
- CLIN CHEM: Nonprotein Nitrogen Compounds (NPN) : Topic Outline Urea Uric AcidDocument7 pagesCLIN CHEM: Nonprotein Nitrogen Compounds (NPN) : Topic Outline Urea Uric AcidJezzah Mae CañeteNo ratings yet
- Abnormal PsychologyDocument136 pagesAbnormal PsychologyMary Ye Ariola Magsino100% (3)
- NCM 112 E LEARNING AutosavedDocument7 pagesNCM 112 E LEARNING AutosavedMikko McDonie VeloriaNo ratings yet
- Manual Urinalysis: Lynne PowellDocument37 pagesManual Urinalysis: Lynne PowellAdhya TiaraNo ratings yet
- Anatomy of Human EyeDocument41 pagesAnatomy of Human EyeCarly MelachioNo ratings yet
- Immuno-Serology: Antistreptolysin 0Document13 pagesImmuno-Serology: Antistreptolysin 0Romie SolacitoNo ratings yet
- BLOCK II LMS Quiz AnatomyDocument27 pagesBLOCK II LMS Quiz AnatomyAshley BuchananNo ratings yet
- High Yield Psychiatry: Shelf Exam Review Emma Holliday RamahiDocument71 pagesHigh Yield Psychiatry: Shelf Exam Review Emma Holliday RamahisamNo ratings yet
- Background of The StudyDocument7 pagesBackground of The StudyVern LeStrangeNo ratings yet
- Study Guid Patho 1Document41 pagesStudy Guid Patho 1sturner7887No ratings yet
- Alzheimer Disease EngDocument35 pagesAlzheimer Disease EngAna IantucNo ratings yet
- Basic Brain AnatomyDocument36 pagesBasic Brain Anatomymartha wibawaNo ratings yet