Download as docx, pdf, or txt
You might also like
- 2020 OPT Plus Results in NCR - PPT - FinalDocument26 pages2020 OPT Plus Results in NCR - PPT - FinalGodece RosalNo ratings yet
- Narinig Kaya Nila Ang: Tsismis??Document27 pagesNarinig Kaya Nila Ang: Tsismis??iammerbinpransiskoNo ratings yet
- MDM New Monthly Report - Feb.2019Document8 pagesMDM New Monthly Report - Feb.2019MD.khalilNo ratings yet
- Form 1 Monitoring Form and Masterlist of BeneficiariesDocument2 pagesForm 1 Monitoring Form and Masterlist of BeneficiariesShantal LopezNo ratings yet
- MDM NEW MONTHLY REPORT - March.2019Document14 pagesMDM NEW MONTHLY REPORT - March.2019MD.khalilNo ratings yet
- 12 OPT Plus Form 1B List of Affected at Risk Preschoolers 0 59 Months Old 5 CopiesDocument1 page12 OPT Plus Form 1B List of Affected at Risk Preschoolers 0 59 Months Old 5 CopiesExzur Chavez100% (2)
- Republic of The PhilippinesDocument1 pageRepublic of The PhilippinesUnissNo ratings yet
- 052 AHDC Quarantine Checkpoint Monthly Consolidated ReportDocument2 pages052 AHDC Quarantine Checkpoint Monthly Consolidated ReportAllen Marie Gualingco-FuentesNo ratings yet
- 4113 SOP StuntingDocument3 pages4113 SOP StuntingAmelia OnestiNo ratings yet
- Case CapsuleDocument8 pagesCase CapsuleLiza BulsaraNo ratings yet
- Actual 2Document1 pageActual 2joaquin trinidadNo ratings yet
- Nutrition Situation 2018Document28 pagesNutrition Situation 2018nnnn hhhhNo ratings yet
- September MenuDocument1 pageSeptember MenuJHON JAIRO PEDRAZA VELANDIANo ratings yet
- Student Vital Signs Monitoring Sheet: Ward Student's Name Patient's Name T P R BP T P R BP Bed NoDocument4 pagesStudent Vital Signs Monitoring Sheet: Ward Student's Name Patient's Name T P R BP T P R BP Bed NolizaroaNo ratings yet
- Practicum ChecklistDocument5 pagesPracticum Checklistpelagioalbert24No ratings yet
- Cavite City Accomplishement Garantisadong Pambata DateDocument60 pagesCavite City Accomplishement Garantisadong Pambata DateMike Ace MonzonNo ratings yet
- Assessment Protocol For PR PDFDocument9 pagesAssessment Protocol For PR PDFMikaela Eris CortelloNo ratings yet
- SFP Masterlist, CNS Forms For LGUs 2021-2022Document7 pagesSFP Masterlist, CNS Forms For LGUs 2021-2022XilcaNo ratings yet
- Quality of Care Measures2Document2 pagesQuality of Care Measures2dskubi8661No ratings yet
- Health FormsDocument151 pagesHealth FormsJasmin Kerre VillarinNo ratings yet
- Rabies Summit 2018 Final Raffy DerayDocument28 pagesRabies Summit 2018 Final Raffy DerayMheng Mheng100% (1)
- Rincian Laporan Gizi Ke Dinkes Kabupaten: BulananDocument7 pagesRincian Laporan Gizi Ke Dinkes Kabupaten: BulananernaferiNo ratings yet
- Woodbury County COVID-19 TrendsDocument3 pagesWoodbury County COVID-19 TrendsKatie CoppleNo ratings yet
- STA-LUCIA-BLOOD-DONATION-CERTDocument1 pageSTA-LUCIA-BLOOD-DONATION-CERTimkeepobleteNo ratings yet
- SFP Form 2A & ACCOMPLISHMENT REPORTDocument2 pagesSFP Form 2A & ACCOMPLISHMENT REPORTMary Jane Martinez80% (5)
- Imar ReportDocument1 pageImar ReportCarmina T. JuanicoNo ratings yet
- National Safe Motherhood Program 10 19y.o and Unmetneeds WRA 5Document3 pagesNational Safe Motherhood Program 10 19y.o and Unmetneeds WRA 5suari tantoNo ratings yet
- Attendance Pob - EastDocument1 pageAttendance Pob - EastSylvia N. CantoriaNo ratings yet
- Dashboard of Public Health Indicators: Newly Reported Cases Today Confirmed CasesDocument19 pagesDashboard of Public Health Indicators: Newly Reported Cases Today Confirmed CasesLyleChristineNo ratings yet
- Bliss 1 - MicroscopeDocument2 pagesBliss 1 - MicroscopeSiboyi Ang'anaNo ratings yet
- Form Unified K 7 Masterlisting Form SBI 2019 1Document8 pagesForm Unified K 7 Masterlisting Form SBI 2019 1Art DollosaNo ratings yet
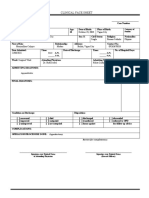
- Clinical Face Sheet: October 23, 2003 Vigan City Single Roman Catholic FilipinoDocument15 pagesClinical Face Sheet: October 23, 2003 Vigan City Single Roman Catholic FilipinoCaitlynNo ratings yet
- Please Check ( ) If Vaccine Has Been GivenDocument2 pagesPlease Check ( ) If Vaccine Has Been GivenClarie Jane MortelNo ratings yet
- Daily Session FormDocument5 pagesDaily Session Formmichael christian orenciadaNo ratings yet
- Toothbrushing ATTENDANCEDocument1 pageToothbrushing ATTENDANCEMaria VistoNo ratings yet
- SBFP Forms 1 6Document25 pagesSBFP Forms 1 6mindalyn aripNo ratings yet
- Deped Memo No. 165, S 2010: WastedDocument6 pagesDeped Memo No. 165, S 2010: WastedJayne InoferioNo ratings yet
- SBFP-Form-5 - PAPAACDocument2 pagesSBFP-Form-5 - PAPAACRenabeth CastroNo ratings yet
- MORTALITY AUDIT FORM FOR HIV - TB - HEI CLIENTS Final VersionDocument12 pagesMORTALITY AUDIT FORM FOR HIV - TB - HEI CLIENTS Final VersionMigori ArtNo ratings yet
- Abstract 3Document6 pagesAbstract 3Wobik HopeNo ratings yet
- Laporan Bulanan Sikda AprilDocument9 pagesLaporan Bulanan Sikda AprilSport J T ENo ratings yet
- Com Di 2021 Revise FINAL 2.0Document44 pagesCom Di 2021 Revise FINAL 2.0Maria Sofia DGNo ratings yet
- Demand and Supply AnalysisDocument12 pagesDemand and Supply AnalysisMary Chriszle DomisiwNo ratings yet
- Please Check ( ) If Vaccine Has Been GivenDocument2 pagesPlease Check ( ) If Vaccine Has Been GivenClarie Jane MortelNo ratings yet
- Kusta 2018Document23 pagesKusta 2018rita rosdianaNo ratings yet
- ExchangeDocument1 pageExchangespaghettanNo ratings yet
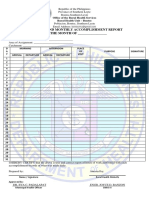
- Office of The City Health Officer: CertificationDocument2 pagesOffice of The City Health Officer: CertificationKathleen Shei Dela CruzNo ratings yet
- Inventory SheetDocument1 pageInventory SheetMoisha DacaraNo ratings yet
- 23-09-2021 HMB EnglishDocument9 pages23-09-2021 HMB EnglishduraivelanNo ratings yet
- Anemia en RNDocument21 pagesAnemia en RNDaniel Martinez DiazNo ratings yet
- MDM New Monthly Report - June.2019Document78 pagesMDM New Monthly Report - June.2019MD.khalilNo ratings yet
- CatchUp Form TemplateDocument7 pagesCatchUp Form TemplateGinalyn Gine- GarduqueNo ratings yet
- Program Terminal ReportDocument5 pagesProgram Terminal ReportIrene BalinbinNo ratings yet
- Regional Nutrition Situation Result Based On EOPT and School Weighing Result 2018-2020Document13 pagesRegional Nutrition Situation Result Based On EOPT and School Weighing Result 2018-2020nnnn hhhhNo ratings yet
- SFP - Masterlist 2014 - NHTSDocument79 pagesSFP - Masterlist 2014 - NHTSEllaine Grace ArenasNo ratings yet
- Population Development Core Indicators Data Date SourceDocument2 pagesPopulation Development Core Indicators Data Date SourceLemuel CayabyabNo ratings yet
- Kardex: GCS: 12-13/15 (M:5, V:4-5, E:3)Document11 pagesKardex: GCS: 12-13/15 (M:5, V:4-5, E:3)Dienizs Labini TadenaNo ratings yet
- New Argao LatestDocument44 pagesNew Argao LatestMhike EvansNo ratings yet
- Opt 2022Document312 pagesOpt 2022bhagzc khuyaNo ratings yet
- Under WeightDocument2 pagesUnder Weightbhagzc khuyaNo ratings yet
- OPT Plus Form 1A - WT 4 AgeDocument2 pagesOPT Plus Form 1A - WT 4 Agebhagzc khuyaNo ratings yet
- NO. Name of Mother Name of Child Birthday AGE in Mos. AGE in YearsDocument21 pagesNO. Name of Mother Name of Child Birthday AGE in Mos. AGE in Yearsbhagzc khuyaNo ratings yet
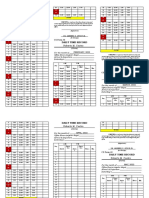
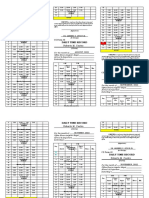
- Roberto M. Castro: Daily Time RecordDocument3 pagesRoberto M. Castro: Daily Time Recordbhagzc khuyaNo ratings yet
- Record of Barangay InhabitantDocument246 pagesRecord of Barangay Inhabitantbhagzc khuyaNo ratings yet
- DTR Form JULY - DECEMBERDocument3 pagesDTR Form JULY - DECEMBERbhagzc khuyaNo ratings yet
- Memorandum of AgreementDocument2 pagesMemorandum of Agreementbhagzc khuya100% (1)
- DTR Form JANUARY - JUNEDocument3 pagesDTR Form JANUARY - JUNEbhagzc khuyaNo ratings yet
- Budget PlanDocument2 pagesBudget Planbhagzc khuyaNo ratings yet