Download as pdf or txt
You might also like
- 062 Pathology MCQ Respiratory SystemDocument4 pages062 Pathology MCQ Respiratory Systemمجتبى علي100% (18)
- Ortho Survival GuideDocument28 pagesOrtho Survival GuideAmir AliNo ratings yet
- AG 8th TermDocument50 pagesAG 8th TermNeelesh PatilNo ratings yet
- Lec 2 Peripheral Nerve CompressionDocument4 pagesLec 2 Peripheral Nerve CompressionEmily MurrayNo ratings yet
- Lec 2 Peripheral Nerve CompressionDocument4 pagesLec 2 Peripheral Nerve CompressionEmily MurrayNo ratings yet
- Hand ExamDocument49 pagesHand Examياسر نعيم الربيعيNo ratings yet
- Tinywow Communicable-Diseases 48897647 4Document1 pageTinywow Communicable-Diseases 48897647 4JULIUS CEZAR QUINAYNo ratings yet
- Iontophoresis Carpal Tunnel SyndromeDocument2 pagesIontophoresis Carpal Tunnel SyndromeIkre19No ratings yet
- (SEMINAR) Median Nerve Injury + Carpal Tunnel SyndromeDocument25 pages(SEMINAR) Median Nerve Injury + Carpal Tunnel SyndromeAda JoraimiNo ratings yet
- Dedos y ManoDocument15 pagesDedos y ManoSamantha AriasNo ratings yet
- Rhumato5an Poly-Sd Canalaires2017Document3 pagesRhumato5an Poly-Sd Canalaires2017Amine OuanayaNo ratings yet
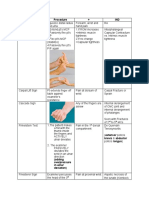
- Test Name Procedure + IND: ND TH STDocument3 pagesTest Name Procedure + IND: ND TH STDesi SmithNo ratings yet
- MODULE 5: Neurological Infection. Autoimmune and NeuropathiesDocument6 pagesMODULE 5: Neurological Infection. Autoimmune and NeuropathiesClemente AbinesNo ratings yet
- Surgery Bites and Stings With TetanusDocument5 pagesSurgery Bites and Stings With TetanusEduardo Marco Villarama DayritNo ratings yet
- Avoiding Nerve Injury From VenipunctureDocument10 pagesAvoiding Nerve Injury From VenipunctureKeren Nathaniel AlvaradoNo ratings yet
- WK 8 Study Guide Quest Ans PCP 1 2020 GHDocument5 pagesWK 8 Study Guide Quest Ans PCP 1 2020 GHapi-453771787No ratings yet
- Median NerveDocument40 pagesMedian Nervehumera100% (2)
- Peripheral Nerve Disorders (Dr. Ken)Document72 pagesPeripheral Nerve Disorders (Dr. Ken)Nurindha Shimelia M ZNo ratings yet
- Wrist and Hand Disease Description Pathophysiology Sign and Symptoms Management Carpal Tunnel SyndromeDocument4 pagesWrist and Hand Disease Description Pathophysiology Sign and Symptoms Management Carpal Tunnel SyndromeMei BejeranoNo ratings yet
- FW2A AssignemntsDocument7 pagesFW2A Assignemntsekalvino1610No ratings yet
- Wrist and Finger SeminarDocument40 pagesWrist and Finger SeminarMisoNo ratings yet
- Carpal Tunnel PresentationDocument27 pagesCarpal Tunnel PresentationsboNo ratings yet
- OSCEstop Neurological Hand ExaminationDocument1 pageOSCEstop Neurological Hand Examinationtaek123No ratings yet
- Hand InjuriesDocument13 pagesHand InjuriesRifQi KurniawanNo ratings yet
- REFERAT Koass Neurologi - Carpal Tunnel SyndromeDocument34 pagesREFERAT Koass Neurologi - Carpal Tunnel SyndromeVindhita RatiputriNo ratings yet
- US Spine ExtremitiesDocument3 pagesUS Spine ExtremitiesBrent DizonNo ratings yet
- Greenhill 2017Document4 pagesGreenhill 2017BSPT BooksNo ratings yet
- Closed Comminutive Fracture Middle Left Clavicle Allman Classification Group IDocument32 pagesClosed Comminutive Fracture Middle Left Clavicle Allman Classification Group IWilliamtatokieesz Tembokrumahampebenjol-benjolNo ratings yet
- DISASTERDocument3 pagesDISASTERAndrea Mae AngkicoNo ratings yet
- Iontophoresis TENNIS ELBOW (Lateral Humeral Epicondylitis)Document2 pagesIontophoresis TENNIS ELBOW (Lateral Humeral Epicondylitis)Ikre19No ratings yet
- PCP Q WK 8Document3 pagesPCP Q WK 8api-477982644No ratings yet
- Rheumatoid Arthritis SLE Scleroderma Dermatomyositis: Dr. Khaled KhaliliaDocument17 pagesRheumatoid Arthritis SLE Scleroderma Dermatomyositis: Dr. Khaled KhaliliaMihaela Munteanu100% (1)
- Tinywow Communicable-Diseases 48897647 5Document1 pageTinywow Communicable-Diseases 48897647 5JULIUS CEZAR QUINAYNo ratings yet
- NCP DMDocument4 pagesNCP DMAarav (мя Ρєяfєт)No ratings yet
- Sample Power PointDocument7 pagesSample Power PointZanie CruzNo ratings yet
- NCP Requirements RleDocument7 pagesNCP Requirements RleZymer Lee AbasoloNo ratings yet
- 3 - ALR Main - DoigtsDocument62 pages3 - ALR Main - DoigtsProfesseur Christian Dumontier100% (1)
- Impaired Skin Integrity Related To Trauma or Infection: ObjectivesDocument5 pagesImpaired Skin Integrity Related To Trauma or Infection: Objectivesmhean azneitaNo ratings yet
- Microbiology 19 PDFDocument6 pagesMicrobiology 19 PDFLyka Villagracia AsiloNo ratings yet
- Hand Injuries Guidelines 2020Document64 pagesHand Injuries Guidelines 2020Andrew WongNo ratings yet
- HandTrauma-1 0Document103 pagesHandTrauma-1 0mhmad AbbadiNo ratings yet
- Peripheral Nerve Injuries c61Document69 pagesPeripheral Nerve Injuries c61Kevo YoungNo ratings yet
- Hand PeDocument2 pagesHand PeIffah NabihaNo ratings yet
- Carpal Tunnel Syndrome (CTS) Adalah Penyakit DegenerativeDocument2 pagesCarpal Tunnel Syndrome (CTS) Adalah Penyakit DegenerativenatasyahNo ratings yet
- Peripheral Nerve DisordersDocument66 pagesPeripheral Nerve DisordersReno Andri0% (1)
- HAND ExaminationDocument11 pagesHAND ExaminationEbtesamNo ratings yet
- Leprosy Type 1 Reaction (Formerly Reversal Reaction) : Bernard Naafs, MD, PHD, Colette L.M. Van Hees, MDDocument14 pagesLeprosy Type 1 Reaction (Formerly Reversal Reaction) : Bernard Naafs, MD, PHD, Colette L.M. Van Hees, MDAdrianus KevinNo ratings yet
- CD Additional LessonsDocument13 pagesCD Additional LessonsAlma Janella TOSINONo ratings yet
- Trigger Finger: Dr. Aswedi Putra, SP - OT, FICS Universitas MalahayatiDocument9 pagesTrigger Finger: Dr. Aswedi Putra, SP - OT, FICS Universitas MalahayatiJessy WidiyantiNo ratings yet
- DeQuervain TenosynovitisDocument24 pagesDeQuervain TenosynovitisKavivarma Raj RajendranNo ratings yet
- Trigger Finger (Digital Tenovaginosis) (Subset of Stenosing Tenosynovitis)Document7 pagesTrigger Finger (Digital Tenovaginosis) (Subset of Stenosing Tenosynovitis)Md Ahsanuzzaman PinkuNo ratings yet
- Endodontic Emergency (Dr. Imran)Document2 pagesEndodontic Emergency (Dr. Imran)aelessyaNo ratings yet
- The Temporomandibular JointDocument57 pagesThe Temporomandibular JointAminah KhanNo ratings yet
- Locomotive Disorders FALLERDocument7 pagesLocomotive Disorders FALLERRoyce Vincent TizonNo ratings yet
- Hand InfectionsDocument68 pagesHand InfectionsSuren VishvanathNo ratings yet
- Angela Hand and Upper ExtremityDocument59 pagesAngela Hand and Upper ExtremityJenny RajanNo ratings yet
- Roles and Responsibilities of The First AiderDocument8 pagesRoles and Responsibilities of The First AiderPascual Ronald PatrickNo ratings yet
- Carpal Tunnel Syndrome (CTS)Document50 pagesCarpal Tunnel Syndrome (CTS)Nor Fatin GaliNo ratings yet
- Tetanus: DR - Vemuri ChaitanyaDocument49 pagesTetanus: DR - Vemuri ChaitanyaalifNo ratings yet
- HandTrauma-1 0Document103 pagesHandTrauma-1 0Dragne AlinaNo ratings yet
- Hand Disorders, A Simple Guide To The Condition, Diagnosis, Treatment And Improvised TreatmentFrom EverandHand Disorders, A Simple Guide To The Condition, Diagnosis, Treatment And Improvised TreatmentNo ratings yet
- Research Governance HandbookDocument41 pagesResearch Governance HandbookIbrahim QariNo ratings yet
- Research As A Transferable Skill Course OverviewDocument4 pagesResearch As A Transferable Skill Course OverviewIbrahim QariNo ratings yet
- Russia Political MapDocument1 pageRussia Political MapIbrahim QariNo ratings yet
- Basic Swahili Course For TouristsDocument12 pagesBasic Swahili Course For TouristsIbrahim QariNo ratings yet
- jcm00141 0073Document6 pagesjcm00141 0073Ibrahim QariNo ratings yet
- Module 4 Considerations and Capacities of Contact LawsDocument4 pagesModule 4 Considerations and Capacities of Contact LawsIbrahim QariNo ratings yet
- References:: 1-Essen4al of Molecular Biology by George M. Malacinski 4 Edi4on 2Document19 pagesReferences:: 1-Essen4al of Molecular Biology by George M. Malacinski 4 Edi4on 2Ibrahim QariNo ratings yet
- Specification Accredited A Level Gce History A h505Document132 pagesSpecification Accredited A Level Gce History A h505Ibrahim QariNo ratings yet
- Transferable Skills Information PackDocument20 pagesTransferable Skills Information PackIbrahim QariNo ratings yet
- Susy CourseDocument359 pagesSusy CourseIbrahim QariNo ratings yet
- Laos PDFDocument1 pageLaos PDFIbrahim QariNo ratings yet
- Poland MapDocument1 pagePoland MapIbrahim QariNo ratings yet
- Marketing Your ProductDocument101 pagesMarketing Your ProductIbrahim QariNo ratings yet
- Kotobati - كتاب حكم وأمثال شعبية للكاتبة رانيا بوراس.Document87 pagesKotobati - كتاب حكم وأمثال شعبية للكاتبة رانيا بوراس.Ibrahim QariNo ratings yet
- Map of ItalyDocument1 pageMap of ItalyIbrahim QariNo ratings yet
- ConjunctivitisDocument1 pageConjunctivitisIbrahim QariNo ratings yet
- Module 2 Ministry of JusticeDocument3 pagesModule 2 Ministry of JusticeIbrahim QariNo ratings yet
- Defining Cuisine and Types of Cuisine: Jordan Kocevski, PHD Michael Risteski, PHDDocument12 pagesDefining Cuisine and Types of Cuisine: Jordan Kocevski, PHD Michael Risteski, PHDIbrahim QariNo ratings yet
- Uia 09 PHYSIOLOGY OF THE KIDNEYDocument5 pagesUia 09 PHYSIOLOGY OF THE KIDNEYIbrahim QariNo ratings yet
- Infective ConjunctivitisDocument2 pagesInfective ConjunctivitisIbrahim QariNo ratings yet
- Accounting & Finance (Session-5)Document52 pagesAccounting & Finance (Session-5)Ibrahim QariNo ratings yet
- Emojevwe V Respiratory Physiologyoer1595509Document133 pagesEmojevwe V Respiratory Physiologyoer1595509Ibrahim QariNo ratings yet
- Introduction To Carpentry Tools and JointsDocument8 pagesIntroduction To Carpentry Tools and JointsIbrahim QariNo ratings yet
- The Marketing "Mix"Document5 pagesThe Marketing "Mix"Ibrahim QariNo ratings yet
- Chapter One: The Role of Marketing Research in Management Decision MakingDocument17 pagesChapter One: The Role of Marketing Research in Management Decision MakingIbrahim QariNo ratings yet
- Accounting & Finance (Session-2)Document33 pagesAccounting & Finance (Session-2)Ibrahim QariNo ratings yet
- Introduction To MarketingDocument17 pagesIntroduction To MarketingIbrahim QariNo ratings yet
- APznzaZjEw5YQRByekcj2P79uwLOg8h--2J_rjMfs_LJYwNtCqpMToKzsAUaeIIcxDgEJS_UeGGsGWhJBs0ek6wChxnVlWvrLFdMxDkgMs...-YWRjq37tAIJmhMiFlLLYpMXYM0iM9pUzxdZK2Zt_Mk4Irf-jH6S85QiKsJKafYuuKN81x9_8AVsu0le2w5FL63Zv_fo-rhvt9tvLUwmFiB3kIVbAHMVZP0g==Document39 pagesAPznzaZjEw5YQRByekcj2P79uwLOg8h--2J_rjMfs_LJYwNtCqpMToKzsAUaeIIcxDgEJS_UeGGsGWhJBs0ek6wChxnVlWvrLFdMxDkgMs...-YWRjq37tAIJmhMiFlLLYpMXYM0iM9pUzxdZK2Zt_Mk4Irf-jH6S85QiKsJKafYuuKN81x9_8AVsu0le2w5FL63Zv_fo-rhvt9tvLUwmFiB3kIVbAHMVZP0g==Ibrahim QariNo ratings yet
- Accounting & Finance (Session-3)Document41 pagesAccounting & Finance (Session-3)Ibrahim QariNo ratings yet
- Accounting & Finance (Session-8)Document37 pagesAccounting & Finance (Session-8)Ibrahim QariNo ratings yet
- Vitamin B6 Deficiency As A Cause of Polyneuropathy in POEMS Syndrome Rapid Recovery With Supplementation in Two CasesDocument7 pagesVitamin B6 Deficiency As A Cause of Polyneuropathy in POEMS Syndrome Rapid Recovery With Supplementation in Two CasesYaseen MohamnadNo ratings yet
- Pathology: Tutorial 5Document18 pagesPathology: Tutorial 5Salma AshrafNo ratings yet
- Bell's Palsy Treatments & Medications - SingleCareDocument11 pagesBell's Palsy Treatments & Medications - SingleCareRoxan PacsayNo ratings yet
- Bino - Lec - Midterm Exam - Yellow - PadDocument11 pagesBino - Lec - Midterm Exam - Yellow - PadDanielle SangalangNo ratings yet
- Treacher-Collins Syndrome (TCS), Also Known As Treacher-Collins-Franceschetti Syndrome, Mandibulofacial DysostosisDocument17 pagesTreacher-Collins Syndrome (TCS), Also Known As Treacher-Collins-Franceschetti Syndrome, Mandibulofacial DysostosisAilyn LoroNo ratings yet
- Blood Blank 1 PDFDocument6 pagesBlood Blank 1 PDFRajkumar RoderickNo ratings yet
- Essential Epidemiology An Introduction For Students and Health Professionals 3rd Webb Test BankDocument8 pagesEssential Epidemiology An Introduction For Students and Health Professionals 3rd Webb Test BankNatalie Joy100% (37)
- A Literally Review On ArbudaDocument5 pagesA Literally Review On ArbudaEditor IJTSRDNo ratings yet
- What Is ThalassemiaDocument2 pagesWhat Is ThalassemiaFatima Azzahra Khairul AnuarNo ratings yet
- Renal Tubular Acidosis Type IDocument7 pagesRenal Tubular Acidosis Type IAmber LiaqatNo ratings yet
- DP New Patient Form - 2023Document5 pagesDP New Patient Form - 2023cdbn2326No ratings yet
- Gastrointestinal Imaging - The Requisites (4e) (2014) (Unitedvrg)Document435 pagesGastrointestinal Imaging - The Requisites (4e) (2014) (Unitedvrg)crazyballerman80890% (10)
- CVA Activity IntoleranceDocument1 pageCVA Activity IntoleranceNursesLabs.com75% (4)
- Tetraogy of FallotDocument9 pagesTetraogy of FallotMary Louise MadariagaNo ratings yet
- DR Lohiya 8 Page Book EnglishDocument8 pagesDR Lohiya 8 Page Book Englishdrsunilk100% (1)
- 04 SPS SAINS TG2-Nota Grafik B4Document6 pages04 SPS SAINS TG2-Nota Grafik B4AZAMOLLYNo ratings yet
- Drug DetoxcificationDocument23 pagesDrug DetoxcificationPUSAT LATIHAN AADKNo ratings yet
- NCPDocument2 pagesNCPdimple caspilloNo ratings yet
- New Born ScreeningDocument30 pagesNew Born ScreeningJastine Miguel EGUIANo ratings yet
- GingivitisDocument30 pagesGingivitisSharon DingNo ratings yet
- Pengetahuan Dan Sikap Masyarakat Terhadap Penyakit Malaria Di Desa Kolongan Kecamatan Talawaan Kabupaten Minahasa UtaraDocument6 pagesPengetahuan Dan Sikap Masyarakat Terhadap Penyakit Malaria Di Desa Kolongan Kecamatan Talawaan Kabupaten Minahasa Utarasri humaerahNo ratings yet
- Term Paper On Anxiety DisorderDocument5 pagesTerm Paper On Anxiety Disorderc5qrar20100% (1)
- Assessment Diagnosis Scientific Explanation Planning Interventions Rationale Expected Outcome Subjective: O Short Term: Short TermDocument3 pagesAssessment Diagnosis Scientific Explanation Planning Interventions Rationale Expected Outcome Subjective: O Short Term: Short TermRaidis PangilinanNo ratings yet
- 13q Deletions Various FTNPDocument4 pages13q Deletions Various FTNPMartin GirardNo ratings yet
- MelasmaDocument2 pagesMelasmaAngelique SewgobindNo ratings yet
- Case Presentation OralcavityDocument33 pagesCase Presentation Oralcavityapi-250609678No ratings yet
- Thesis On Inguinal HerniaDocument7 pagesThesis On Inguinal Herniaambermooreeverett100% (3)
- CBD - Kiki Bangun Wijaya - PPOKDocument13 pagesCBD - Kiki Bangun Wijaya - PPOKkiki WijayaNo ratings yet
- Burns MGNT and CalculationDocument7 pagesBurns MGNT and CalculationPoova RagavanNo ratings yet