Download as pdf or txt
You might also like
- HIV Mobile Testing Unit Grant RequestDocument7 pagesHIV Mobile Testing Unit Grant RequestBrenna CallahanNo ratings yet
- HIV Statistics San AntonioDocument30 pagesHIV Statistics San AntonioIvan HerreraNo ratings yet
- UNAIDS HIV Epidemic Overview 2018Document39 pagesUNAIDS HIV Epidemic Overview 2018Bhekisisa Health100% (1)
- Local Public Health in Uncertain Times: Julie Morita, MD Commissioner Chicago Department of Public HealthDocument39 pagesLocal Public Health in Uncertain Times: Julie Morita, MD Commissioner Chicago Department of Public HealthNational Press FoundationNo ratings yet
- Document OutputDocument95 pagesDocument Outputngtiequang2No ratings yet
- Pediatric Hiv - Zambia.Document59 pagesPediatric Hiv - Zambia.Linus PuleNo ratings yet
- Hiv Conference 2019Document45 pagesHiv Conference 2019Keletso NyathiNo ratings yet
- Seminar Epidemi HIV Indonesia - 10april2019 - C6Document59 pagesSeminar Epidemi HIV Indonesia - 10april2019 - C6Eny VeronikaNo ratings yet
- 2015 PHE Leptospirosis CaldasDocument22 pages2015 PHE Leptospirosis Caldasno nameNo ratings yet
- GPH Tutok Gamutan Davao OrientalDocument3 pagesGPH Tutok Gamutan Davao Orientalrizza RiveraNo ratings yet
- Patofisiologi Kanker RahimDocument98 pagesPatofisiologi Kanker RahimOjo Nesu100% (1)
- Infectious and Congenital Syphilis in Canada, 2010-2015: Y Choudhri, J Miller, J Sandhu, A Leon, J AhoDocument6 pagesInfectious and Congenital Syphilis in Canada, 2010-2015: Y Choudhri, J Miller, J Sandhu, A Leon, J AhoKrinta AlisaNo ratings yet
- Ped HIV QuizDocument56 pagesPed HIV QuizRizqi AmaliaNo ratings yet
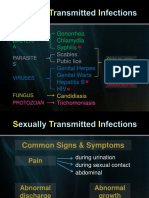
- Sti Hiv Aids LectureDocument89 pagesSti Hiv Aids Lecturepedrong dodongNo ratings yet
- AidsDocument45 pagesAidsrockycamaligan2356No ratings yet
- Diabetes Patient EducationDocument96 pagesDiabetes Patient EducationbajaocNo ratings yet
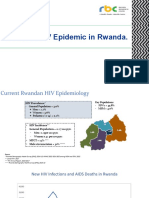
- State of HIV Epidemic in RwandaDocument17 pagesState of HIV Epidemic in RwandaNshimiyimana Jean ClaudeNo ratings yet
- Pencegahan HivDocument36 pagesPencegahan HivyaneemayNo ratings yet
- Health and Nutritional Status of Filipino Adults, 20-59 Years OldDocument32 pagesHealth and Nutritional Status of Filipino Adults, 20-59 Years OldJose Mari TrinidadNo ratings yet
- Cancer Hospital Case Study ChennaiDocument19 pagesCancer Hospital Case Study ChennaiVelram ShanmugamNo ratings yet
- Hiv Aids 131221220813 Phpapp02Document46 pagesHiv Aids 131221220813 Phpapp0261 Pankaj RochwaniNo ratings yet
- Laryngeal Cancer, Risk Factors, Symptoms and Treatment PDFDocument8 pagesLaryngeal Cancer, Risk Factors, Symptoms and Treatment PDFandre halimNo ratings yet
- NAP (Harry P.) PDFDocument29 pagesNAP (Harry P.) PDFaldyNo ratings yet
- Case Ana Pancreatic CaDocument21 pagesCase Ana Pancreatic CakingpinNo ratings yet
- HIV 101 EditedDocument47 pagesHIV 101 EditedJordan MBNo ratings yet
- Cancer Incidence in The Gaza Strip Facts & Figures 2015-2016Document13 pagesCancer Incidence in The Gaza Strip Facts & Figures 2015-2016PressureserveNo ratings yet
- Prof. (DR.) V.P.Acharya MBBS, Md. PHDDocument41 pagesProf. (DR.) V.P.Acharya MBBS, Md. PHDDrViyatprajna AcharyaNo ratings yet
- 2018 HIV STD OverviewDocument40 pages2018 HIV STD OverviewMadeline CiakNo ratings yet
- Overview of Global HIVDocument27 pagesOverview of Global HIVAhmed AdemNo ratings yet
- 2021aug Hiv Sti 101 2018 Stats v1Document66 pages2021aug Hiv Sti 101 2018 Stats v1Narendra GowdaNo ratings yet
- 2016 Tuberculosis Statistical Report FinalDocument36 pages2016 Tuberculosis Statistical Report FinalBurcu OzdemirNo ratings yet
- Country Factsheets Zambia 2019changeDocument8 pagesCountry Factsheets Zambia 2019changeMangani “Prince” ChinyimbaNo ratings yet
- Hiv Aids Programme Update Arv Logistic: Sumatera UtaraDocument48 pagesHiv Aids Programme Update Arv Logistic: Sumatera UtaraindahflsaragihNo ratings yet
- Novel Coronavirus (COVID-19) : Updates For Clinicians: September 4, 2020Document44 pagesNovel Coronavirus (COVID-19) : Updates For Clinicians: September 4, 2020Mahita SainiNo ratings yet
- 2WW Cancer Referrals PowerPoint 2021Document25 pages2WW Cancer Referrals PowerPoint 2021Umer AnwarNo ratings yet
- March 17 Grand Forks Health Officer's DashboardDocument11 pagesMarch 17 Grand Forks Health Officer's DashboardJoe BowenNo ratings yet
- HIV in RwandaDocument29 pagesHIV in RwandaRichard BalaisNo ratings yet
- Coping and Health in Tanzania (CHAT) : Preliminary FindingsDocument27 pagesCoping and Health in Tanzania (CHAT) : Preliminary Findingskyle_hamilton9947No ratings yet
- CCO 2020 Contemporary Management of HIV Emerging Approaches DownloadableDocument52 pagesCCO 2020 Contemporary Management of HIV Emerging Approaches Downloadableluis hernandezNo ratings yet
- Covid RosarioDocument11 pagesCovid RosarioDiego MussettaNo ratings yet
- WHO - HQ - Reports G2 PROD EXT TBCountryProfileDocument1 pageWHO - HQ - Reports G2 PROD EXT TBCountryProfileAngelo Santos EstrellaNo ratings yet
- DR O Power Point Pediatric COVID CasesDocument28 pagesDR O Power Point Pediatric COVID CasesErika EsquivelNo ratings yet
- 10b Measuring Energy Input and OutputDocument69 pages10b Measuring Energy Input and OutputRay PeramathevanNo ratings yet
- Hepatitis B in Pregnancy PDFDocument38 pagesHepatitis B in Pregnancy PDFAlsyNo ratings yet
- Case Processing SummaryDocument4 pagesCase Processing SummaryLuthfi LazuardiNo ratings yet
- SURABAYA TB UPDATE DR - Asik SuryaDocument71 pagesSURABAYA TB UPDATE DR - Asik Suryawidya vannesaNo ratings yet
- Substance Abuse Cat ADocument57 pagesSubstance Abuse Cat AShonaMalhanNo ratings yet
- Contemporary Management of HIV: Emerging Paradigms in ARTDocument45 pagesContemporary Management of HIV: Emerging Paradigms in ARTluamsmarinsNo ratings yet
- The Preliminary Findings of South Africa's Latest HIV Household SurveyDocument4 pagesThe Preliminary Findings of South Africa's Latest HIV Household SurveyBhekisisa HealthNo ratings yet
- Clinical Profile of Isolation Ward Patients Amidst Pandemic of Covid-19 in Workshop Hospital Kanchrapara, Eastern Railway & Their ManagementDocument24 pagesClinical Profile of Isolation Ward Patients Amidst Pandemic of Covid-19 in Workshop Hospital Kanchrapara, Eastern Railway & Their ManagementSubhashish DasNo ratings yet
- Management of AIDS-Related Opportunistic Infections IDocument53 pagesManagement of AIDS-Related Opportunistic Infections IRaniNo ratings yet
- Multiple Choice Questions: ST RDDocument6 pagesMultiple Choice Questions: ST RDAbdulrab SaeedNo ratings yet
- 2016 W. Va. Overdose Fatality AnalysisDocument26 pages2016 W. Va. Overdose Fatality AnalysisAnna MooreNo ratings yet
- HIV Testing in Clinical SettingsDocument16 pagesHIV Testing in Clinical SettingszidabyNo ratings yet
- From DOTS To The Stop TB Strategy - Summary Report of 30 October by DR R. VianzonDocument18 pagesFrom DOTS To The Stop TB Strategy - Summary Report of 30 October by DR R. VianzonNaddia NNo ratings yet
- Mpox Outbreak Response Vaccine EffectivenessDocument59 pagesMpox Outbreak Response Vaccine EffectivenessTreyNo ratings yet
- Ospe Statistics and Occupational HealthDocument21 pagesOspe Statistics and Occupational HealthHariNo ratings yet
- Cancer Trends Progress Report: Note To UsersDocument8 pagesCancer Trends Progress Report: Note To UsersGanapathi RajNo ratings yet
- gtbr2017 Annex2Document62 pagesgtbr2017 Annex2Helao SilasNo ratings yet
- Histopathology Reporting: Guidelines for Surgical CancerFrom EverandHistopathology Reporting: Guidelines for Surgical CancerDavid P. BoyleNo ratings yet
- Eugenia Cooney ObituaryDocument14 pagesEugenia Cooney ObituaryRain NakagoNo ratings yet
- Questions and Answers: Hepatitis BDocument4 pagesQuestions and Answers: Hepatitis BRain NakagoNo ratings yet
- UntitledDocument104 pagesUntitledRain NakagoNo ratings yet
- Synsacra of The Eocene Antarctic PeDocument13 pagesSynsacra of The Eocene Antarctic PeRain NakagoNo ratings yet
- ZOO 3713 Syllabus SP20Document4 pagesZOO 3713 Syllabus SP20Rain NakagoNo ratings yet
- Diagnosis of Viral Hepatitis: ReviewDocument13 pagesDiagnosis of Viral Hepatitis: ReviewReza Redha AnandaNo ratings yet
- World AIDS Day Infographic: Fighting HIV/AIDS in The LGBT CommunityDocument1 pageWorld AIDS Day Infographic: Fighting HIV/AIDS in The LGBT CommunityFenway HealthNo ratings yet
- GWL InaDocument25 pagesGWL Inatugba1234No ratings yet
- 2011 Sex Workers Gap Analysis ReportDocument68 pages2011 Sex Workers Gap Analysis ReportOfficeNo ratings yet
- STD Facts - Syphilis (Detailed)Document4 pagesSTD Facts - Syphilis (Detailed)Dorothy Pearl Loyola PalabricaNo ratings yet
- Report - Impact of The Naz Foundation JudgmentDocument60 pagesReport - Impact of The Naz Foundation JudgmentNidhi KhannaNo ratings yet
- The Evolving Epidemiology of HIV AIDS.9Document9 pagesThe Evolving Epidemiology of HIV AIDS.9JuliaNo ratings yet
- Psychology FinalsDocument139 pagesPsychology FinalsHoney Grace Calica RamirezNo ratings yet
- Stefania Boccia, Paolo Villari, Walter Ricciardi (Eds.) - A Systematic Review of Key Issues in Public Health (2015, Springer International Publishing)Document294 pagesStefania Boccia, Paolo Villari, Walter Ricciardi (Eds.) - A Systematic Review of Key Issues in Public Health (2015, Springer International Publishing)Agus GunadiNo ratings yet
- Homosexuality in Church and State - Mapping The IssuesDocument78 pagesHomosexuality in Church and State - Mapping The IssuesPaul Christopher James BurgessNo ratings yet
- LGBT FactsDocument43 pagesLGBT Factsjohn kaneNo ratings yet
- Drug Abuse HIV and AIDSDocument12 pagesDrug Abuse HIV and AIDSTaranisaNo ratings yet
- Survey Tool Dummy TableDocument10 pagesSurvey Tool Dummy TableJPJessiePaulNo ratings yet
- HIV/AIDS in The PhilippinesDocument5 pagesHIV/AIDS in The PhilippinesRop RabinoNo ratings yet
- Task 1 - PDD - Completed Task Model AnswerssDocument5 pagesTask 1 - PDD - Completed Task Model AnswerssGis ThaNo ratings yet
- Fundamental Baptist Churches Wade Into Anti LGBTQI+ BillDocument11 pagesFundamental Baptist Churches Wade Into Anti LGBTQI+ BillGertrude OtchereNo ratings yet
- Can Oral Sex Transmit HIV?Document52 pagesCan Oral Sex Transmit HIV?Leo LamsNo ratings yet
- Hiv in The Asean Region Regional Report On Hiv Aids 1decDocument118 pagesHiv in The Asean Region Regional Report On Hiv Aids 1decFrans LandiNo ratings yet
- Oliver Ross (Auth.) Same-Sex Desire in Indian Culture Representations in Literature and Film, 1970-2015-Palgrave Macmillan US (2016)Document211 pagesOliver Ross (Auth.) Same-Sex Desire in Indian Culture Representations in Literature and Film, 1970-2015-Palgrave Macmillan US (2016)Lucero López100% (1)
- 1117Document5 pages1117Melvin WijayaNo ratings yet
- Chapter 4 Communicable DiseaseDocument33 pagesChapter 4 Communicable DiseaseAyro Business CenterNo ratings yet
- Mansci G16 Final PaperDocument21 pagesMansci G16 Final PaperAllan Patrick AlsimNo ratings yet
- Law & Morality of Suicide & HomosexualityDocument70 pagesLaw & Morality of Suicide & HomosexualityJaya VatsNo ratings yet
- Weil 10162778 Thesis Sigs RemovedDocument326 pagesWeil 10162778 Thesis Sigs RemovedDoromalXD SorbitoNo ratings yet
- Dahod District Final Updated ReportDocument27 pagesDahod District Final Updated Reportapi-19964711No ratings yet
- JULY 2019: Newly Diagnosed Hiv CasesDocument8 pagesJULY 2019: Newly Diagnosed Hiv CasesJan Shaltiel Vincent EstradaNo ratings yet
- Rbap HHD 2014 Blia Nepal Country ReportDocument82 pagesRbap HHD 2014 Blia Nepal Country ReportSwati AnandNo ratings yet
- AIDS and Its Discontents in Serbia: Silencing Gay Sexuality in The Age of IllnessDocument94 pagesAIDS and Its Discontents in Serbia: Silencing Gay Sexuality in The Age of IllnessDjurica StankovNo ratings yet
- Sextrans 2018 053705Document6 pagesSextrans 2018 053705HoangNo ratings yet