Download as docx, pdf, or txt
You might also like
- Epidural Technique in Obstetric Anesthesia-Springer International Publishing - Springer (2020) PDFDocument176 pagesEpidural Technique in Obstetric Anesthesia-Springer International Publishing - Springer (2020) PDFomarvillaNo ratings yet
- Hygiene (NCLEX) Flashcards - QuizletDocument5 pagesHygiene (NCLEX) Flashcards - QuizletA.No ratings yet
- Or NCP (Knowledge Deficit)Document1 pageOr NCP (Knowledge Deficit)Nikki M. ArapolNo ratings yet
- NCP PreoperativeDocument3 pagesNCP PreoperativeMark Allison Buenaventura75% (4)
- Risk For InjuryDocument4 pagesRisk For InjuryJanina Patricia BuddleNo ratings yet
- Malnutrition AdimeDocument2 pagesMalnutrition Adimeapi-508953960No ratings yet
- Planning Fixed Partial Dentures For Severely Misaligned AbutmentsDocument7 pagesPlanning Fixed Partial Dentures For Severely Misaligned AbutmentsAntonny VasquezNo ratings yet
- NURSING CARE PLAN (Glaucoma)Document5 pagesNURSING CARE PLAN (Glaucoma)Calvo AdrianNo ratings yet
- Nursing Care Plan Nursing Care PlanDocument3 pagesNursing Care Plan Nursing Care PlanVince Christian BartulabaNo ratings yet
- St. Paul University PhilippinesDocument3 pagesSt. Paul University PhilippinesMia GarciaNo ratings yet
- Or NCP Impaired Elimination - CompressDocument1 pageOr NCP Impaired Elimination - CompressWeird WorldNo ratings yet
- PostPartum NCP1Document3 pagesPostPartum NCP1serummapleNo ratings yet
- Ectopic PregnancyDocument2 pagesEctopic PregnancyKim GalamgamNo ratings yet
- Cues/Evidences Nursing Diagnosis Objectives Interventions Rationale EvaluationDocument4 pagesCues/Evidences Nursing Diagnosis Objectives Interventions Rationale EvaluationJoanne Therese ArbasNo ratings yet
- Viii. Nursing Management Nursing Care Plan # 1 Assessment Diagnosis Planning Implementation Rationale EvaluationDocument6 pagesViii. Nursing Management Nursing Care Plan # 1 Assessment Diagnosis Planning Implementation Rationale EvaluationStar AlvarezNo ratings yet
- Assessment Diagnosis Planning Intervention Rationale Evaluation Goal MetDocument2 pagesAssessment Diagnosis Planning Intervention Rationale Evaluation Goal MetDickson,Emilia JadeNo ratings yet
- Western Mindanao State University College of Nursing Fundamentals in Nursing Practice (Lecture) Course Output (Final Term)Document3 pagesWestern Mindanao State University College of Nursing Fundamentals in Nursing Practice (Lecture) Course Output (Final Term)Reann LeeNo ratings yet
- NCP Anxiety - BSN114 FEU-IN 2010-2011Document3 pagesNCP Anxiety - BSN114 FEU-IN 2010-2011merryechevarriaNo ratings yet
- Nursing Assessment S - O Pt. May ManifestDocument4 pagesNursing Assessment S - O Pt. May Manifestk_a1990No ratings yet
- Assignment 4 - Fernandez, Dexter IvanDocument4 pagesAssignment 4 - Fernandez, Dexter IvanIvan FernandezNo ratings yet
- Nursing Care Plan: Saint Paul University PhilippinesDocument6 pagesNursing Care Plan: Saint Paul University PhilippinesChristian UmosoNo ratings yet
- Situational Low Self-Esteem - NCPDocument3 pagesSituational Low Self-Esteem - NCPLizzey YuNo ratings yet
- Mark Norriel CelisDocument2 pagesMark Norriel CelisMark Norriel CajandabNo ratings yet
- Nursing Care Plan of Disturbed Thought Process: Subjective Cues: General Objectives: Independent InterventionDocument15 pagesNursing Care Plan of Disturbed Thought Process: Subjective Cues: General Objectives: Independent InterventionJanella JinksonNo ratings yet
- Anxiety Psychological NCPDocument2 pagesAnxiety Psychological NCPKit Lara100% (1)
- Anxiety in WIlm's TumorDocument3 pagesAnxiety in WIlm's TumorDwinxelle Eiven CristobalNo ratings yet
- Assessment Nursing Diagnosis Planning Intervention Rationale EvaluationDocument2 pagesAssessment Nursing Diagnosis Planning Intervention Rationale EvaluationMonteroso, Kae Rhenzel A.No ratings yet
- NCP 66Document1 pageNCP 66Dheng EsquijoNo ratings yet
- NCP FinalDocument5 pagesNCP Finalnorhain4.aNo ratings yet
- NPI Format: General ObjDocument5 pagesNPI Format: General ObjMeryville JacildoNo ratings yet
- Delivery Nursing Care PlanDocument6 pagesDelivery Nursing Care PlanKayelyn-Rose CombateNo ratings yet
- Assessment Diagnosis Planning Intervention Rationale EvaluationDocument1 pageAssessment Diagnosis Planning Intervention Rationale EvaluationLex CatNo ratings yet
- Nursing Care Plan. CabgDocument4 pagesNursing Care Plan. CabgCecil MonteroNo ratings yet
- College of Health Sciences: Urdaneta City UniversityDocument2 pagesCollege of Health Sciences: Urdaneta City UniversityDan Dan ManaoisNo ratings yet
- NCP Template 11Document8 pagesNCP Template 11Carey Jamille YadanNo ratings yet
- NCP For Surgical CasesDocument10 pagesNCP For Surgical Caseslouie roderosNo ratings yet
- NCPDocument7 pagesNCPChris Denver BancaleNo ratings yet
- Assessment Diagnosis Planning Intervention Rationale Evaluation SubjectiveDocument15 pagesAssessment Diagnosis Planning Intervention Rationale Evaluation SubjectiveWhoo CaresNo ratings yet
- NCP Anxiety RT Diagnostic ProcedureDocument2 pagesNCP Anxiety RT Diagnostic ProcedureJenny Ajoc0% (1)
- Nursing Care PlanDocument3 pagesNursing Care PlanGlady mae LimNo ratings yet
- NCP-and-Drug-study For MENDocument8 pagesNCP-and-Drug-study For MENVillie SumandeNo ratings yet
- NCP PrioritizationDocument7 pagesNCP PrioritizationLouwella RamosNo ratings yet
- NCPDocument6 pagesNCPIrene Grace BalcuevaNo ratings yet
- نسخة case med and ncpDocument8 pagesنسخة case med and ncpBudoor AlatawiNo ratings yet
- NCP (Gonzales) Mar 29 - Ventura PDFDocument3 pagesNCP (Gonzales) Mar 29 - Ventura PDFJian VenturaNo ratings yet
- Schizophrenia XIII-XIV (091323) NCPsDocument11 pagesSchizophrenia XIII-XIV (091323) NCPsGlenn ConcepcionNo ratings yet
- NCP CnsDocument3 pagesNCP Cnsandrea salesNo ratings yet
- Nursing Care Plan Nursing Diagnosis Anxiety (Mild)Document4 pagesNursing Care Plan Nursing Diagnosis Anxiety (Mild)yvenette_kris871881% (27)
- Revised NCPDocument11 pagesRevised NCPRovic Selga TrisinioNo ratings yet
- NCP of Endometrical CancerDocument2 pagesNCP of Endometrical CancerFrando kennethNo ratings yet
- Family Nursing Care Plan (Hypertension)Document4 pagesFamily Nursing Care Plan (Hypertension)KANT JAMES D. MAHANNo ratings yet
- Asehan Heart NCP NCM 112Document9 pagesAsehan Heart NCP NCM 112ACOB, Jamil C.No ratings yet
- NCP3 Risk InjuryDocument2 pagesNCP3 Risk InjuryEkusu Yu ShunNo ratings yet
- Clinical Teaching Plan DRDocument4 pagesClinical Teaching Plan DRCagabcab Canibel MelanyNo ratings yet
- Nursing Care PlanDocument3 pagesNursing Care PlanSophia Loraine Dorone Jesura100% (1)
- Anxiety NCPDocument4 pagesAnxiety NCPMARK JASON DIAZNo ratings yet
- Assessment Diagnosis Planning Implimentation Rationale ResponseDocument3 pagesAssessment Diagnosis Planning Implimentation Rationale Responsekhate fonteNo ratings yet
- Nursing Care PlanDocument3 pagesNursing Care PlandeliejoyceNo ratings yet
- Scientific Analysis Goal: Goal:: Subjective CuesDocument2 pagesScientific Analysis Goal: Goal:: Subjective CuesChloie Marie RosalejosNo ratings yet
- Nursing Care Plan: - Appraise Knowledge Toward The ProcedureDocument5 pagesNursing Care Plan: - Appraise Knowledge Toward The ProcedureimnasNo ratings yet
- Medical Integration Model as it Pertains to Musculoskeletal ConditionsFrom EverandMedical Integration Model as it Pertains to Musculoskeletal ConditionsNo ratings yet
- Crunch Time Review for the Certified Nursing Assistant (CNA) ExamFrom EverandCrunch Time Review for the Certified Nursing Assistant (CNA) ExamNo ratings yet
- Information Overload: Framework, Tips, and Tools to Manage in Complex Healthcare EnvironmentsFrom EverandInformation Overload: Framework, Tips, and Tools to Manage in Complex Healthcare EnvironmentsNo ratings yet
- Git-Ppt 20240207 095930 0000Document63 pagesGit-Ppt 20240207 095930 0000Airha Mhae HomoNo ratings yet
- Medical Surgical Nursing LECDocument573 pagesMedical Surgical Nursing LECAirha Mhae HomoNo ratings yet
- Health Teaching Homo ManuelDocument2 pagesHealth Teaching Homo ManuelAirha Mhae HomoNo ratings yet
- Journal Report NCM 107 Rle MaternalDocument3 pagesJournal Report NCM 107 Rle MaternalAirha Mhae HomoNo ratings yet
- Nursing Open - 2022 - Wang - Assessing Patient Safety Culture in Obstetrics Ward A Pilot Study Using A Modified ManchesterDocument7 pagesNursing Open - 2022 - Wang - Assessing Patient Safety Culture in Obstetrics Ward A Pilot Study Using A Modified ManchesterAirha Mhae HomoNo ratings yet
- Thera. Comm AlsDocument32 pagesThera. Comm AlsMelody LandichoNo ratings yet
- Articles Rgarding Importantce of Minerals and Effects of Food DepletionDocument16 pagesArticles Rgarding Importantce of Minerals and Effects of Food Depletionapi-3827527No ratings yet
- Emergency Department PolicyDocument18 pagesEmergency Department PolicyKumar Gavali Suryanarayana100% (1)
- Thermolite 890 Stabilizer - PSSDocument3 pagesThermolite 890 Stabilizer - PSSQwerty RoyalNo ratings yet
- Ag Listing 05oct2023Document98 pagesAg Listing 05oct2023kiranduggarajuNo ratings yet
- Sanet Me0803120575Document169 pagesSanet Me0803120575parallax1957No ratings yet
- Legal Responsibilities of The NurseDocument8 pagesLegal Responsibilities of The NurseWisley GadinganNo ratings yet
- Lesson 5.1 Introduction To Health Information System HIS 1Document36 pagesLesson 5.1 Introduction To Health Information System HIS 1mariel santosNo ratings yet
- Module 3 WorksheetDocument6 pagesModule 3 Worksheetemje torrionNo ratings yet
- Exm 2020Document5 pagesExm 2020Frederick MullerNo ratings yet
- Acute Respiratory Distress SyndromeDocument17 pagesAcute Respiratory Distress SyndromeSanjeet Sah100% (1)
- Iim Grp-1 Capstone ProjectDocument24 pagesIim Grp-1 Capstone ProjectAbhi SNo ratings yet
- 9 ANO - 3 AV Inglês (Com Gabarito e Contéudo)Document5 pages9 ANO - 3 AV Inglês (Com Gabarito e Contéudo)Aila CastroNo ratings yet
- Quick Guide To TTEDocument16 pagesQuick Guide To TTEwen1190No ratings yet
- Konru 3 Sep 2022Document24 pagesKonru 3 Sep 2022sibbNo ratings yet
- Alpesh Patel: Sam's Club Pharmacy: (2011-Current) Wal-Mart Pharmacy: (September 2005-2011)Document2 pagesAlpesh Patel: Sam's Club Pharmacy: (2011-Current) Wal-Mart Pharmacy: (September 2005-2011)Hani EsmaelNo ratings yet
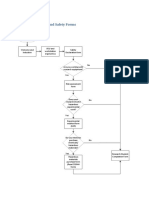
- Flow Chart: Health and Safety FormsDocument2 pagesFlow Chart: Health and Safety FormsBenouna FertNo ratings yet
- Asa Physical Status Classification SystemDocument1 pageAsa Physical Status Classification SystemFredy PaulNo ratings yet
- Heath and SafetyDocument14 pagesHeath and SafetyAyesha KashaNo ratings yet
- RETRATRUTIDEDocument13 pagesRETRATRUTIDECristobal Alvarado LivacicNo ratings yet
- Curriculum Vitae: Anil Shivangala Career ObjectiveDocument2 pagesCurriculum Vitae: Anil Shivangala Career ObjectiveHema KrishnaNo ratings yet
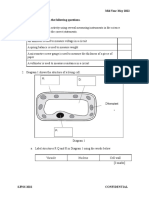
- F2 Mid-Year Exam Section BDocument3 pagesF2 Mid-Year Exam Section BAnne Marian Anak JOSEPHNo ratings yet
- 3.hospital RHC Stgs - Federal Government of Somalia PDFDocument200 pages3.hospital RHC Stgs - Federal Government of Somalia PDFFaisal mohammed AbdullahiNo ratings yet
- SupradynDocument5 pagesSupradynashrayagrawalNo ratings yet
- 3 23 2005 Aviation EnglishDocument14 pages3 23 2005 Aviation EnglishSky LukeNo ratings yet
- Leadership Development For Students of Color - KarmaHall Edu (2024)Document1 pageLeadership Development For Students of Color - KarmaHall Edu (2024)marcelNo ratings yet