Download as pdf or txt
You might also like
- Life Sciences Grade 10 Revision Material Term 2 - 2023Document28 pagesLife Sciences Grade 10 Revision Material Term 2 - 2023Linati Dawedi100% (1)
- Revalidas 2017 - WholeDocument99 pagesRevalidas 2017 - WholeAffie SaikolNo ratings yet
- Cytoplasm Mitochondrion Nucleolus Nucleus Organ Tissue Vacuole Cell Membrane Cell Wall Chlorophyll Chloroplast ChromosomeDocument17 pagesCytoplasm Mitochondrion Nucleolus Nucleus Organ Tissue Vacuole Cell Membrane Cell Wall Chlorophyll Chloroplast Chromosomeardusias100% (1)
- The Development of The Middle Ear Spaces and Their Surgical SignificanceDocument15 pagesThe Development of The Middle Ear Spaces and Their Surgical SignificanceDrTarek Mahmoud Abo Kammer100% (2)
- Microbiology-ELISA Testing Lab ReportDocument2 pagesMicrobiology-ELISA Testing Lab Reportsaraebo33% (3)
- 2-Referencias y Tecnicas Usadas en Clasificacion Hueso Alveolar - SeriwatanachaiDocument5 pages2-Referencias y Tecnicas Usadas en Clasificacion Hueso Alveolar - SeriwatanachaimnhjrtbnzbNo ratings yet
- Reference and Techniques Used in Alveolar Bone ClassificationDocument5 pagesReference and Techniques Used in Alveolar Bone ClassificationAna Carolina LoyolaNo ratings yet
- Algun DiaDocument6 pagesAlgun DiaMarco Antonio García LunaNo ratings yet
- Wee Neutral ZoneDocument7 pagesWee Neutral ZoneGeby JeonNo ratings yet
- Perio PaperDocument15 pagesPerio PaperJunita Elvrida DoloksaribuNo ratings yet
- Tomography 09 00098 v2Document10 pagesTomography 09 00098 v2salsabilaadellaNo ratings yet
- Zona Neutra Maxilofacial PacienteDocument6 pagesZona Neutra Maxilofacial Pacientemargarita de montenegroNo ratings yet
- Taub - Nonunion of Mandibular MidlineDocument4 pagesTaub - Nonunion of Mandibular MidlineChristopher McMullinNo ratings yet
- 2020 Article 73180Document11 pages2020 Article 73180rachmadyNo ratings yet
- Calvarial Bone Grafting For Three-Dimensi Reconstruction of Severe Maxillary Defects: A CDocument11 pagesCalvarial Bone Grafting For Three-Dimensi Reconstruction of Severe Maxillary Defects: A Cmatias112No ratings yet
- Ridge Preservation Techniques For Implant Therapy: JO M I 2009 24 :260-271Document12 pagesRidge Preservation Techniques For Implant Therapy: JO M I 2009 24 :260-271Viorel FaneaNo ratings yet
- 1 s2.0 S0889540609009482 Main PDFDocument7 pages1 s2.0 S0889540609009482 Main PDFSoe San KyawNo ratings yet
- Materiales P Vs RDocument11 pagesMateriales P Vs RJuliana RodriguezNo ratings yet
- Articulo 1 PerioDocument8 pagesArticulo 1 PerioJose Enrique AvilaNo ratings yet
- 1548-1336 (2004) 030 0030 Aocarc 2 0 Co 2Document10 pages1548-1336 (2004) 030 0030 Aocarc 2 0 Co 2waf51No ratings yet
- Prediction of Implant Loss and Marginal Bone Loss by Analysis of Dental Panoramic RadiographsDocument6 pagesPrediction of Implant Loss and Marginal Bone Loss by Analysis of Dental Panoramic RadiographsMuhammad RidwanNo ratings yet
- Bodily Distalization of Molars With Absolute AnchorageDocument12 pagesBodily Distalization of Molars With Absolute AnchorageAnamika AttrishiNo ratings yet
- AJDSM Volume 22 Issue 3 Pages 247-251Document5 pagesAJDSM Volume 22 Issue 3 Pages 247-251MarisbebelaNo ratings yet
- Densit Osoasa A Palatului DurDocument8 pagesDensit Osoasa A Palatului DurDiana DrutaNo ratings yet
- Biologic Width and Crown Lengthening: Case Reports and ReviewDocument7 pagesBiologic Width and Crown Lengthening: Case Reports and ReviewSusi LpjNo ratings yet
- Split Technique 2Document8 pagesSplit Technique 2Alejandro RuizNo ratings yet
- Mandibular Bone Block Harvesting From The Retromolar Region: A 10-Year Prospective Clinical StudyDocument10 pagesMandibular Bone Block Harvesting From The Retromolar Region: A 10-Year Prospective Clinical StudyFerenc NagyNo ratings yet
- Fuhrmann 2002Document6 pagesFuhrmann 2002DentalErNo ratings yet
- EDI Journal - A Graftless Solution For Adjacent Implants in The Aesthetic Zone - Dr. Tunkiwala Et AlDocument6 pagesEDI Journal - A Graftless Solution For Adjacent Implants in The Aesthetic Zone - Dr. Tunkiwala Et AlNaina TalwarNo ratings yet
- Cambios Histológicos Asociados A La Extracción DentalDocument10 pagesCambios Histológicos Asociados A La Extracción DentalAle ZuzaNo ratings yet
- Fotos OclusalesDocument6 pagesFotos OclusalesMarco Antonio García LunaNo ratings yet
- Cirugía OralDocument7 pagesCirugía OralLenny GrauNo ratings yet
- Vital Pulp Therapy of Mandibular Incisor PDFDocument4 pagesVital Pulp Therapy of Mandibular Incisor PDFSebastian CastroNo ratings yet
- Safe Zone AjoDocument7 pagesSafe Zone AjojoeNo ratings yet
- Alargamento Coronario en Zonas EsteticasDocument9 pagesAlargamento Coronario en Zonas EsteticasCamila BórquezNo ratings yet
- Bone Ring 1Document6 pagesBone Ring 1Pradusha RevuruNo ratings yet
- Thickness BoneDocument9 pagesThickness BonemalifaragNo ratings yet
- Journal of Oral Biology and Craniofacial ResearchDocument5 pagesJournal of Oral Biology and Craniofacial ResearchBagis Emre GulNo ratings yet
- Free Flaps MaxillaDocument7 pagesFree Flaps MaxillaFahad QiamNo ratings yet
- 1 s2.0 S088954060901155X MainDocument8 pages1 s2.0 S088954060901155X Mainbruno mañonNo ratings yet
- Itsmo en Conducto Mesiobucal en Primera MolarDocument7 pagesItsmo en Conducto Mesiobucal en Primera MolarSaray ValerioNo ratings yet
- Mermigos 11 01Document4 pagesMermigos 11 01Sankurnia HariwijayadiNo ratings yet
- Extraction Socket Presenvation Using A Collagen Plug Combined With Platelet Rich Plasma (PRP) RADIOGRAPIHICDocument7 pagesExtraction Socket Presenvation Using A Collagen Plug Combined With Platelet Rich Plasma (PRP) RADIOGRAPIHICrachmadyNo ratings yet
- Mandibular Reconstruction With Lateral Tibial Bone Graft: An Excellent Option For Oral and Maxillofacial SurgeryDocument7 pagesMandibular Reconstruction With Lateral Tibial Bone Graft: An Excellent Option For Oral and Maxillofacial SurgeryDwifitri MaretaNo ratings yet
- The Effect of Conventional Surgery and Piezoelectric Surgery Bone Harvesting Techniques On The Donor Site Morbidity of The Mandibular Ramus and SymphysisDocument7 pagesThe Effect of Conventional Surgery and Piezoelectric Surgery Bone Harvesting Techniques On The Donor Site Morbidity of The Mandibular Ramus and SymphysisguhanderNo ratings yet
- 371-Article Text-1509-3-10-20210710Document6 pages371-Article Text-1509-3-10-20210710Fransiski HoNo ratings yet
- Corticotomia Tunel AsistidoDocument7 pagesCorticotomia Tunel Asistidokatya Serrano LemusNo ratings yet
- Quantitative Evaluation of Cortical BoneDocument6 pagesQuantitative Evaluation of Cortical Bonehector rinconNo ratings yet
- Artículo Khoury2018Document10 pagesArtículo Khoury2018Basma Derdabi100% (1)
- Screw Tent Pole Graft TechniqueDocument8 pagesScrew Tent Pole Graft TechniqueSweet ToothNo ratings yet
- Mandibular Anterior Intrusion Using Miniscrews For Skeletal Anchorage: A 3-Dimensional Finite Element AnalysisDocument8 pagesMandibular Anterior Intrusion Using Miniscrews For Skeletal Anchorage: A 3-Dimensional Finite Element AnalysisBruno M. StrangioNo ratings yet
- Maxillary Buccal Cortical Plate InclinationDocument6 pagesMaxillary Buccal Cortical Plate InclinationDa Hae SungNo ratings yet
- Microsaw and Piezosurgery in Harvesting Mandibular Bone Blocks From The Retromolar Region: A Randomized Split-Mouth Prospective Clinical TrialDocument8 pagesMicrosaw and Piezosurgery in Harvesting Mandibular Bone Blocks From The Retromolar Region: A Randomized Split-Mouth Prospective Clinical TrialdivyaNo ratings yet
- Pietrokovski 2007Document7 pagesPietrokovski 2007vickydivi09No ratings yet
- Zachrisson2004 Management of Missing Maxillary Anterior Teeth With Emphasis On AutotransplantationDocument5 pagesZachrisson2004 Management of Missing Maxillary Anterior Teeth With Emphasis On AutotransplantationplsssssNo ratings yet
- A Long-Term Study of 370 Autotransplanted Premolars.Document11 pagesA Long-Term Study of 370 Autotransplanted Premolars.jing.zhao222No ratings yet
- 7-Rapid Maxillary Expansion PDFDocument10 pages7-Rapid Maxillary Expansion PDFAmro YounisNo ratings yet
- Change in Crown-to-Implant Ratio of Implants Placed in Grafted and Nongrafted Posterior Maxillary Sites: A 5-Year Prospective Randomized StudyDocument6 pagesChange in Crown-to-Implant Ratio of Implants Placed in Grafted and Nongrafted Posterior Maxillary Sites: A 5-Year Prospective Randomized StudyValeria CrespoNo ratings yet
- Prosthodontic Management of Dentate Maxillectomy Patient A Clinical Case ReportActa Marisiensis Seria MedicaDocument4 pagesProsthodontic Management of Dentate Maxillectomy Patient A Clinical Case ReportActa Marisiensis Seria MedicaSaniaNo ratings yet
- Case SeriesDocument7 pagesCase Seriesemi_alaNo ratings yet
- Aula EduinaDocument7 pagesAula EduinaJoão S NetoNo ratings yet
- Buccal-Lingual Bone Remodeling in Immediately Loaded Fresh Socket Implants A Cone Beam Computed Tomography StudyDocument8 pagesBuccal-Lingual Bone Remodeling in Immediately Loaded Fresh Socket Implants A Cone Beam Computed Tomography StudyYuki MuraNo ratings yet
- Isidor 1985Document9 pagesIsidor 1985Tania GonzálezNo ratings yet
- Case PPDocument8 pagesCase PPAbhishek GuptaNo ratings yet
- Short ImplantsFrom EverandShort ImplantsBoyd J. TomasettiNo ratings yet
- Kantor 1976, Alv Bone Regeneration After Removal of Inflammatory and Traumatic FactorsDocument9 pagesKantor 1976, Alv Bone Regeneration After Removal of Inflammatory and Traumatic Factorsshir keshalesNo ratings yet
- 5 - Circulation GraysDocument33 pages5 - Circulation GraysdrmanojkulNo ratings yet
- URINALYSISDocument1 pageURINALYSISSyan ApuyanNo ratings yet
- Laboratory Activity 11 - Cardiovascular SystemDocument4 pagesLaboratory Activity 11 - Cardiovascular SystemMV ANo ratings yet
- Pages From Physio Term 2Document453 pagesPages From Physio Term 2Deshi SportsNo ratings yet
- McMinn's Concise Human Anatomy 2nd EdDocument289 pagesMcMinn's Concise Human Anatomy 2nd Edica ssNo ratings yet
- SCIENCE 8 - SummativeDocument4 pagesSCIENCE 8 - SummativeJERIZZA MAGNE PARAFINANo ratings yet
- (Final) Intervertebral Disc Replacement Using Origami Structures - Luke PrudhoeDocument26 pages(Final) Intervertebral Disc Replacement Using Origami Structures - Luke PrudhoelukeNo ratings yet
- AIM Homoeopathy AIAPGET 2022 Mock SyllabusDocument19 pagesAIM Homoeopathy AIAPGET 2022 Mock SyllabusDr-Sayantan BasuNo ratings yet
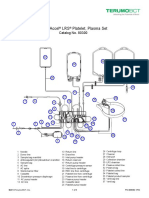
- Trima Accel LRS Platelet, Plasma Set: Catalog No. 80300Document10 pagesTrima Accel LRS Platelet, Plasma Set: Catalog No. 80300Suneo HonekawaNo ratings yet
- PALPATION of Swelling D Hussain NazeeshaDocument17 pagesPALPATION of Swelling D Hussain NazeeshaHUSSAIN NAZEESHANo ratings yet
- Class 12 Subject: Biology Chapter-2: FlowerDocument30 pagesClass 12 Subject: Biology Chapter-2: FlowerSufiyanNo ratings yet
- Autonomic Nervus System: Dr. Meida Sofyana, MbiomedDocument26 pagesAutonomic Nervus System: Dr. Meida Sofyana, MbiomedAyu Tiara FitriNo ratings yet
- Red Cell Suspension Preparation and Reverse Typing ProcedureDocument2 pagesRed Cell Suspension Preparation and Reverse Typing Procedurediversedct100% (4)
- Retention Times For Records, Reports, and SpecimensDocument1 pageRetention Times For Records, Reports, and SpecimensDayledaniel SorvetoNo ratings yet
- Secretion of Small IntestineDocument18 pagesSecretion of Small IntestineMaliha MumtazNo ratings yet
- Science 7 Compendium 2nd QTR With CoverDocument66 pagesScience 7 Compendium 2nd QTR With CoverLyra Mae De BotonNo ratings yet
- TomboyDocument26 pagesTomboyMuhammad AbubakarNo ratings yet
- ManjistaDocument103 pagesManjistaSundara Veerraju100% (2)
- 5 DR Nico PPt. PIT IKABI 2022Document45 pages5 DR Nico PPt. PIT IKABI 2022dewiswahyuNo ratings yet
- AnatomDocument11 pagesAnatomDragan DragovicNo ratings yet
- Anti-HG Eng Rev04Document2 pagesAnti-HG Eng Rev04Ventas2lp IcerlabNo ratings yet
- Anatomy and PhysiologyDocument10 pagesAnatomy and PhysiologyLiwayway Bayoca LozanoNo ratings yet
- Anatomy Psychology: "Biomechanical Movement"Document10 pagesAnatomy Psychology: "Biomechanical Movement"IlyasroisulfahmiNo ratings yet
- Class:10 Subject:biology Chapter:control and CoordinationDocument16 pagesClass:10 Subject:biology Chapter:control and Coordinationkhushi guptaNo ratings yet