Download as pdf or txt
You might also like
- Insert - Elecsys IgE II.04827031500.V12.enDocument4 pagesInsert - Elecsys IgE II.04827031500.V12.enRaj KumarNo ratings yet
- WNG Upright Action ProcedureDocument31 pagesWNG Upright Action ProcedureChris HsiaoNo ratings yet
- 21505IDocument1 page21505INisa Javadd100% (2)
- AVEVA E3D Tutorial Equipment Modeling With Practical ExampleDocument8 pagesAVEVA E3D Tutorial Equipment Modeling With Practical ExampleRamon Alejandro Porras Hernandez100% (1)
- hdlc4 2017-07 v2Document5 pageshdlc4 2017-07 v2Farid AbderahmaneNo ratings yet
- CHOLDocument3 pagesCHOLKhuon BunthaNo ratings yet
- EN CHOLESTEROLBAOSR6x16Document3 pagesEN CHOLESTEROLBAOSR6x16Yến Minh NguyễnNo ratings yet
- Ifu r920 e HDLC Direct 5Document4 pagesIfu r920 e HDLC Direct 5Osama Ben DawNo ratings yet
- PI e CHOL - 5 7Document2 pagesPI e CHOL - 5 7Salsabila Nur OktavianiNo ratings yet
- PI e LDLC - DIRECT 3Document3 pagesPI e LDLC - DIRECT 3bhanuNo ratings yet
- CholesterolDocument2 pagesCholesterolMidecal LABsNo ratings yet
- LDLC3Document4 pagesLDLC3Michael HenzuNo ratings yet
- PI e CHOL - 5 11Document2 pagesPI e CHOL - 5 11ahmadjaffal2003No ratings yet
- IFU HDL Cholesterol Monlabtest EnglishDocument2 pagesIFU HDL Cholesterol Monlabtest EnglishmrashrafiNo ratings yet
- HDL Cholesterol: PrecipitantDocument2 pagesHDL Cholesterol: PrecipitantMaria NogueraNo ratings yet
- PI e CHOL - 10 18Document2 pagesPI e CHOL - 10 18Osama Ben DawNo ratings yet
- CHED2 0104498631190COIN V3 enDocument4 pagesCHED2 0104498631190COIN V3 enARIF AHAMMED PNo ratings yet
- Cholesterol Reagent: Symbols in Product Labelling Product SummaryDocument2 pagesCholesterol Reagent: Symbols in Product Labelling Product SummaryPaul TuveraNo ratings yet
- PI e LDLC - SELECT 20Document2 pagesPI e LDLC - SELECT 20Naufal NurfNo ratings yet
- 11 CholesterolDocument8 pages11 CholesterolAzhar Clinical Laboratory TubeNo ratings yet
- CHOLESTEROL BLOSR6x16 ENDocument2 pagesCHOLESTEROL BLOSR6x16 ENMeethuanNo ratings yet
- SYNCHRON System(s) Chemistry Information Sheet HDL CholesterolDocument11 pagesSYNCHRON System(s) Chemistry Information Sheet HDL CholesterolanggaririnNo ratings yet
- Cholestest LDLDocument3 pagesCholestest LDLAntz GrownesiaNo ratings yet
- New w7 Cholesterol, Triglyceride Determination, HDL CholesterolDocument118 pagesNew w7 Cholesterol, Triglyceride Determination, HDL Cholesterollily beautyNo ratings yet
- Week 7 Compile WordDocument41 pagesWeek 7 Compile Wordlily beautyNo ratings yet
- At 90406Document2 pagesAt 90406mrashrafiNo ratings yet
- HDL DirectDocument2 pagesHDL DirectanggaririnNo ratings yet
- CholDocument2 pagesCholSinari AlfatNo ratings yet
- 40. High-density lipoprotein (HDL)- (pdf.io)Document1 page40. High-density lipoprotein (HDL)- (pdf.io)tuan vănNo ratings yet
- CholDocument2 pagesCholAnel RedzicNo ratings yet
- Cholesterol HDL DirectDocument1 pageCholesterol HDL DirectTrần Tiến ĐạtNo ratings yet
- En Ldl-CholesterolDocument4 pagesEn Ldl-CholesterolcarineNo ratings yet
- Cholesterol: (Chod / Pod Method)Document2 pagesCholesterol: (Chod / Pod Method)psychejaneNo ratings yet
- Cholesterol HDL Direct: Up To 35 MG/DL 0.91 Mmol/l High Risk 60 MG/DL 1.56 Mmol/l Low RiskDocument1 pageCholesterol HDL Direct: Up To 35 MG/DL 0.91 Mmol/l High Risk 60 MG/DL 1.56 Mmol/l Low RiskAltiemaNo ratings yet
- Clonatest Cholesterol MRDocument4 pagesClonatest Cholesterol MRSuprovet LabotatorioNo ratings yet
- CH200Document4 pagesCH200infocarol2017No ratings yet
- Hdl-Cholesterol: Direct MethodDocument2 pagesHdl-Cholesterol: Direct MethodRabie KhoualdiaNo ratings yet
- Laboratory Procedure ManualDocument23 pagesLaboratory Procedure ManualIseth ISethNo ratings yet
- Cholesterol PAP Stable Liquid+standardDocument1 pageCholesterol PAP Stable Liquid+standardberkahNo ratings yet
- TriglyseridesDocument1 pageTriglyseridesDesiNo ratings yet
- 10.total CholesterolDocument2 pages10.total Cholesteroltuan vănNo ratings yet
- Cholesterol - Liquizyme CHOD-PAP (Single Reagent) PDFDocument2 pagesCholesterol - Liquizyme CHOD-PAP (Single Reagent) PDFHamed AlsalhyNo ratings yet
- Alere Cholestech LDX Cassette CLSI PacketDocument25 pagesAlere Cholestech LDX Cassette CLSI PacketRoberto NutiNo ratings yet
- 11505IDocument1 page11505ITrần Tiến ĐạtNo ratings yet
- Apobt: Nacl Diluent 9%Document3 pagesApobt: Nacl Diluent 9%Yunita RapaNo ratings yet
- Cholesterol ARC CHEMDocument8 pagesCholesterol ARC CHEMSalah AnamNo ratings yet
- Chol10 9Document2 pagesChol10 9Chafa NickNo ratings yet
- Package Insert - CholesterolDocument1 pagePackage Insert - CholesterolliezylcagasNo ratings yet
- CholesterolDocument2 pagesCholesterolAmmar MostafaNo ratings yet
- Automated LDL Cholesterol - Dimension - Rev D DXDCM 09008b838085cac0-1508285940764Document15 pagesAutomated LDL Cholesterol - Dimension - Rev D DXDCM 09008b838085cac0-1508285940764Rizka Diana PutriNo ratings yet
- Assignment 2 SerumDocument4 pagesAssignment 2 Serumhaseeb ShafaatNo ratings yet
- C7510 01 2276Document2 pagesC7510 01 2276topurNo ratings yet
- Bridget BiochemDocument9 pagesBridget BiochemColombia snyperNo ratings yet
- Clinical ChemistryDocument22 pagesClinical ChemistryEarl Francis DarantinaoNo ratings yet
- LIPASEDocument4 pagesLIPASEsyufriyadiNo ratings yet
- HDL DirectDocument2 pagesHDL DirectDinesh SreedharanNo ratings yet
- FNSC 3002 Practical 1 Determination of Plasma Ldl-Cholesterol Hdl-Cholesterol Triacylglycerol and ApolipoproteinsDocument7 pagesFNSC 3002 Practical 1 Determination of Plasma Ldl-Cholesterol Hdl-Cholesterol Triacylglycerol and ApolipoproteinsPurple DecibelNo ratings yet
- Cholesterol KitDocument2 pagesCholesterol KitRahma Ayu WulandariNo ratings yet
- Cholesterol Quantification Using A Spectrophotometric AssayDocument3 pagesCholesterol Quantification Using A Spectrophotometric AssayAlisa LimNo ratings yet
- ContentDocument30 pagesContentZainab Manzoor 340No ratings yet
- HDL RandoxDocument4 pagesHDL RandoxJesus Guillermo Caceres FernandezNo ratings yet
- Food Safety: Innovative Analytical Tools for Safety AssessmentFrom EverandFood Safety: Innovative Analytical Tools for Safety AssessmentUmile Gianfranco SpizzirriNo ratings yet
- Cobas DF EjDocument3 pagesCobas DF EjRaj KumarNo ratings yet
- Insert - Elecsys BRAHMS PCT.08828679501.V3.enDocument11 pagesInsert - Elecsys BRAHMS PCT.08828679501.V3.enRaj KumarNo ratings yet
- Coinv 12Document4 pagesCoinv 12Raj KumarNo ratings yet
- Aakash AIPMT 2014 Code R SolutionDocument27 pagesAakash AIPMT 2014 Code R Solutionblue_l1No ratings yet
- Pythagorean Theorem in BusinessDocument4 pagesPythagorean Theorem in BusinessDeelanshiNo ratings yet
- Katalog 150AET-175AET-200AET-L150AET-L200AET 08Document75 pagesKatalog 150AET-175AET-200AET-L150AET-L200AET 08JONI JONINo ratings yet
- Solutions Nss NC 17Document13 pagesSolutions Nss NC 17lethiphuongdan50% (2)
- Tariq PHD Thesis 13-08Document168 pagesTariq PHD Thesis 13-08unaialapontNo ratings yet
- Class 8 CH 5 Data Handling August 19Document3 pagesClass 8 CH 5 Data Handling August 19shayn budihardjoNo ratings yet
- Rule Book 1Document112 pagesRule Book 1Mukul SoniNo ratings yet
- A&P Book - Aeronautical Charts and CompassDocument17 pagesA&P Book - Aeronautical Charts and CompassHarry NuryantoNo ratings yet
- Mcgill: Ecse 461 - Electric MachineryDocument1 pageMcgill: Ecse 461 - Electric MachineryChirag SoodNo ratings yet
- NJM4558Document4 pagesNJM4558Capuñay Diaz ChristianNo ratings yet
- C# Code ShutdownDocument5 pagesC# Code ShutdownNhạt PhaiNo ratings yet
- Honeywell Thermostat T775A2009Document8 pagesHoneywell Thermostat T775A2009Marco Antonio MartinezNo ratings yet
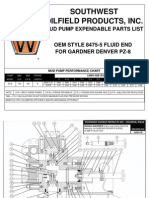
- Oem Gardner Denver Pz-8Document8 pagesOem Gardner Denver Pz-8caballero_tigreNo ratings yet
- 9 - Introduction To Network LayerDocument28 pages9 - Introduction To Network LayerDjangoNo ratings yet
- 09 Ra41219en10gla1 Mimo ModeDocument34 pages09 Ra41219en10gla1 Mimo Modeyaro82No ratings yet
- Bc4157 Course ProfileDocument5 pagesBc4157 Course ProfileMan HongNo ratings yet
- Sampa Axle Rod CatalogueDocument189 pagesSampa Axle Rod CatalogueFabio OchoaNo ratings yet
- LCM and GCFDocument5 pagesLCM and GCFJULIA ALLANANo ratings yet
- Nehru Institute of Engineering and TechnologyDocument2 pagesNehru Institute of Engineering and Technologysaravanaeee2004No ratings yet
- NSO Sample Paper Class 10Document11 pagesNSO Sample Paper Class 10Rana MukherjeeNo ratings yet
- 1 Ex 2A - The Exponential FunctionDocument18 pages1 Ex 2A - The Exponential FunctionRalph Rezin MooreNo ratings yet
- 4037 Additional Mathematics: MARK SCHEME For The October/November 2013 SeriesDocument6 pages4037 Additional Mathematics: MARK SCHEME For The October/November 2013 SeriesSamin IslamNo ratings yet
- Fabrication and Experimental Analysis of Carbon Fibre/Epoxy Composite Leaf SpringDocument9 pagesFabrication and Experimental Analysis of Carbon Fibre/Epoxy Composite Leaf SpringSTEPS WAYNo ratings yet
- Lab Report Marking Rubrics Phy645Document3 pagesLab Report Marking Rubrics Phy645Ridhwan RosliNo ratings yet
- Manage Tablespaces in A Container Database (CDB) and Pluggable Database (PDB)Document3 pagesManage Tablespaces in A Container Database (CDB) and Pluggable Database (PDB)Ahmed NagyNo ratings yet
- Session No. 1.4. The Cell - Transport MechanismsDocument28 pagesSession No. 1.4. The Cell - Transport MechanismsShekaina Faith Cuizon LozadaNo ratings yet
- Panel Punch Points Report-06!08!2019Document165 pagesPanel Punch Points Report-06!08!2019Kamesh MarwadeNo ratings yet
- Strengths: Mixers - AeratorsDocument2 pagesStrengths: Mixers - AeratorsKashif MasudNo ratings yet