Download as pdf or txt
You might also like
- AWS Module 3 - AWS Global InfrastructureDocument36 pagesAWS Module 3 - AWS Global Infrastructuredsadasdasdas0% (1)
- P66 B1 M5 Lufthansa PDFDocument196 pagesP66 B1 M5 Lufthansa PDFDAVID FAJARDO PUERTO100% (1)
- Jci Ssi ToolkitDocument191 pagesJci Ssi ToolkitMr. Jonathan Hudson O.T. Manager, Justice K.S. Hegde Charitable Hospital100% (3)
- American College of Surgeons and Surgical Infection Society - Surgical Site Infection Guidelines, 2016 Update (SSI)Document16 pagesAmerican College of Surgeons and Surgical Infection Society - Surgical Site Infection Guidelines, 2016 Update (SSI)Anonymous LnWIBo1GNo ratings yet
- HPD-suliburk 2019 Oi 190321Document12 pagesHPD-suliburk 2019 Oi 190321tallatjabeenhumairaNo ratings yet
- Patterns of Technical Error Among Surgical Malpractice ClaimsDocument7 pagesPatterns of Technical Error Among Surgical Malpractice ClaimsMroan AlmshrqyNo ratings yet
- Interventions To Decrease Catheter-Related Bloodstream Infections in The ICU: The Keystone Intensive Care Unit ProjectDocument5 pagesInterventions To Decrease Catheter-Related Bloodstream Infections in The ICU: The Keystone Intensive Care Unit ProjectanggitaNo ratings yet
- Surgical Safety ChecklistDocument20 pagesSurgical Safety ChecklistAnonymous h8gt8KlpiCNo ratings yet
- Practices: in Patient CareDocument5 pagesPractices: in Patient Careahmad nuril hidayatNo ratings yet
- PPM PS 2.15 Safe Surgery and AnesthesiaDocument4 pagesPPM PS 2.15 Safe Surgery and AnesthesiacapedeaqNo ratings yet
- Abdominoplasty: Risk Factors, Complication Rates, and Safety of Combined ProceduresDocument10 pagesAbdominoplasty: Risk Factors, Complication Rates, and Safety of Combined Proceduresraja yasminNo ratings yet
- Patient Safety Incident Reporting - Canadian Health SystemDocument13 pagesPatient Safety Incident Reporting - Canadian Health SystemRhod Bernaldez EstaNo ratings yet
- Insiden Kritis Selama Anestesi Dan Periode Awal Pasca Anestesi Studi Cross-Sectional DeskriptifDocument23 pagesInsiden Kritis Selama Anestesi Dan Periode Awal Pasca Anestesi Studi Cross-Sectional DeskriptifTri AyatiNo ratings yet
- PIIS0094129813000345Document8 pagesPIIS0094129813000345Aura RivasNo ratings yet
- Impact of The World Health Organization Surgical Safety Checklist On Patient SafetyDocument6 pagesImpact of The World Health Organization Surgical Safety Checklist On Patient SafetyANDIS SHAFANo ratings yet
- Minimizing Population Health Loss in Times of Scarce Surgical Capacity During The Coronavirus Disease 2019 Crisis and Beyond: A Modeling StudyDocument10 pagesMinimizing Population Health Loss in Times of Scarce Surgical Capacity During The Coronavirus Disease 2019 Crisis and Beyond: A Modeling StudyAriani SukmadiwantiNo ratings yet
- Surgical Site InfectionDocument7 pagesSurgical Site InfectionCaxton ThumbiNo ratings yet
- Preventing Breast Implant ContaminationDocument4 pagesPreventing Breast Implant Contaminationvictorubong404No ratings yet
- Dos Décadas Desde Errar Es HumanoDocument8 pagesDos Décadas Desde Errar Es Humanov3r0-chanNo ratings yet
- Advancing The Science of Measurement of Diagnostic Errors in Healthcare, The Safer DX FrameworkDocument9 pagesAdvancing The Science of Measurement of Diagnostic Errors in Healthcare, The Safer DX FrameworkLucien DedravoNo ratings yet
- 1 s2.0 S0039606007003480 MainDocument8 pages1 s2.0 S0039606007003480 MainAna MîndrilăNo ratings yet
- Problem-Based Research PaperDocument12 pagesProblem-Based Research Paperapi-349372265No ratings yet
- Rba 0 AheadOfPrint 6036c54fa95395582f07f644Document5 pagesRba 0 AheadOfPrint 6036c54fa95395582f07f644STRMoch Hafizh AlfiansyahNo ratings yet
- Never Events in Surgery': Mere Error or An Avoidable DisasterDocument7 pagesNever Events in Surgery': Mere Error or An Avoidable DisasterGopi JaladiNo ratings yet
- Effect of Lean QI Implementation Program On Surgical Pathology Specimen Accessioning and Gross Preparation Error FrequencyDocument7 pagesEffect of Lean QI Implementation Program On Surgical Pathology Specimen Accessioning and Gross Preparation Error Frequencyadin hamiguNo ratings yet
- Groah 2014 Table TalkDocument12 pagesGroah 2014 Table TalkChandra JohannesNo ratings yet
- Colorectal BundlesDocument16 pagesColorectal BundlesDamie ChaulaNo ratings yet
- 5390 20335 1 PBDocument4 pages5390 20335 1 PBSupun S WijekumaraNo ratings yet
- Haemo Vigilance 4Document5 pagesHaemo Vigilance 4Wyhana NadiraNo ratings yet
- 680 FullDocument9 pages680 FullRye CalderonNo ratings yet
- Roils PaperDocument4 pagesRoils Paperapi-575843507No ratings yet
- Continuous Quality Improvements and SafetyDocument3 pagesContinuous Quality Improvements and Safetyapi-518020510No ratings yet
- Jurnal Medical SafetyDocument14 pagesJurnal Medical SafetyMARWAH MARWAHNo ratings yet
- Evaluation of The Care Safety of Patients With Surgical Interventions From A High-Complexity Institution in Medellín, ColombiaDocument9 pagesEvaluation of The Care Safety of Patients With Surgical Interventions From A High-Complexity Institution in Medellín, ColombiaJaime Augusto Quimbayo GuarnizoNo ratings yet
- Shaffer2017-Tutku MacBook ProDocument6 pagesShaffer2017-Tutku MacBook ProMEKSELINA KALENDERNo ratings yet
- Adverse Event or Near-Miss AnalysisDocument10 pagesAdverse Event or Near-Miss Analysisjahxtow safariNo ratings yet
- 1 s2.0 S2049080122006756 MainDocument5 pages1 s2.0 S2049080122006756 MainReskyAyuWulandariNo ratings yet
- Effectiveness of A Multidisciplinary Patient Care Bundle For Reducing Surgical-Site InfectionsDocument8 pagesEffectiveness of A Multidisciplinary Patient Care Bundle For Reducing Surgical-Site InfectionsNurul AidaNo ratings yet
- International Journal of Surgery: ReviewDocument4 pagesInternational Journal of Surgery: ReviewMuhammad RuadiNo ratings yet
- Week2 Submitter PaperDocument3 pagesWeek2 Submitter Paperapi-299189797No ratings yet
- Preoperative Computed Tomography Angiography in Autologous Breast Reconstruction-Incidence and Impact of IncidentalomasDocument6 pagesPreoperative Computed Tomography Angiography in Autologous Breast Reconstruction-Incidence and Impact of IncidentalomasNora Vianey Alcantara VelascoNo ratings yet
- Special Edition From The Quality Assessment and Safety Committee Reducing Surgical Site Infection - Where Do I Look?Document3 pagesSpecial Edition From The Quality Assessment and Safety Committee Reducing Surgical Site Infection - Where Do I Look?Qamar Hafeez KianiNo ratings yet
- Quality Improvement Paper FinalDocument11 pagesQuality Improvement Paper Finalapi-291740538No ratings yet
- Effect of Implementation of A Surgical Safety Checklist On Perioperative and Postoperative Complications at An Academic Institution in North AmericaDocument14 pagesEffect of Implementation of A Surgical Safety Checklist On Perioperative and Postoperative Complications at An Academic Institution in North AmericaMuhammad BasharatullahNo ratings yet
- Making Health Care Safer.2Document9 pagesMaking Health Care Safer.2YANNo ratings yet
- Surgical Specimen Management: A Descriptive Study of 648 Adverse Events and Near MissesDocument7 pagesSurgical Specimen Management: A Descriptive Study of 648 Adverse Events and Near MissesRubia Sari Mamanya HaristNo ratings yet
- Jurnal 8Document10 pagesJurnal 8afri pakalessyNo ratings yet
- The World Health Organisation Surgical Safety Checklist A1: I. YardleyDocument2 pagesThe World Health Organisation Surgical Safety Checklist A1: I. YardleyrajarshikNo ratings yet
- Diagnostic Errors - UpToDateDocument23 pagesDiagnostic Errors - UpToDateJoyce SumagaysayNo ratings yet
- 7057 24972 1 PBDocument133 pages7057 24972 1 PBDen NisNo ratings yet
- FMT001 Prevention of Medical ErrorsDocument43 pagesFMT001 Prevention of Medical ErrorsgailgonesouthNo ratings yet
- Training Using Simulation in Internal Medicine Residencies: An Educational PerspectiveDocument3 pagesTraining Using Simulation in Internal Medicine Residencies: An Educational PerspectiveagaetioNo ratings yet
- Inappropriateness in Laboratory Medicine An Elephant in The RoomDocument4 pagesInappropriateness in Laboratory Medicine An Elephant in The RoomomaromranNo ratings yet
- Monitoring Complications of MeDocument8 pagesMonitoring Complications of Meaxl___No ratings yet
- Surgical Site InfectionDocument38 pagesSurgical Site InfectionRajarshi Kumar0% (1)
- P 19-35 Liability and Quality Issues in Health Case Fifth EditionDocument30 pagesP 19-35 Liability and Quality Issues in Health Case Fifth EditionbillNo ratings yet
- A Lean Six Sigma Team Increases Hand Hygiene ComplianceDocument10 pagesA Lean Six Sigma Team Increases Hand Hygiene Compliancedrustagi100% (1)
- Improving Diagnosis in Health CareDocument4 pagesImproving Diagnosis in Health CareHLMedit100% (1)
- Feature Article: Use of Failure Mode and Effects Analysis To Improve Emergency Department Handoff ProcessesDocument10 pagesFeature Article: Use of Failure Mode and Effects Analysis To Improve Emergency Department Handoff ProcessesAnatha ChrisciliaNo ratings yet
- THSS 10 1663974Document15 pagesTHSS 10 1663974Jamaah Ki HendroNo ratings yet
- Quality Indicators, Performance Measures, and Accountability: The Right Thing, at The Right Time, For The Right ReasonDocument8 pagesQuality Indicators, Performance Measures, and Accountability: The Right Thing, at The Right Time, For The Right ReasonMulyawan Safwandy NugrahaNo ratings yet
- Smoker S Melanosis Isolated Pigmented Lesion In.1603Document1 pageSmoker S Melanosis Isolated Pigmented Lesion In.1603made dharmaNo ratings yet
- Ytaa 560Document2 pagesYtaa 560made dharmaNo ratings yet
- Reconsidering Informed Consent For Trans Identified Children Adolescents and Young AdultsDocument23 pagesReconsidering Informed Consent For Trans Identified Children Adolescents and Young Adultsmade dharmaNo ratings yet
- Bilateral Smokers Melanosis With Rare Site of Occurrence in An Edentulous PatientDocument6 pagesBilateral Smokers Melanosis With Rare Site of Occurrence in An Edentulous Patientmade dharmaNo ratings yet
- Informed Consent For Medical Research - Case StudiesDocument5 pagesInformed Consent For Medical Research - Case Studiesmade dharmaNo ratings yet
- AKI 2 Primary Care Bundle Oxfordshire V 1.1Document1 pageAKI 2 Primary Care Bundle Oxfordshire V 1.1made dharmaNo ratings yet
- UPN Jatim, FinalDocument14 pagesUPN Jatim, Finalmade dharmaNo ratings yet
- Hpab 194Document3 pagesHpab 194made dharmaNo ratings yet
- Mini Note RadiologipdfDocument70 pagesMini Note Radiologipdfmade dharmaNo ratings yet
- Program at A Glannce APICD 2022 FINALDocument2 pagesProgram at A Glannce APICD 2022 FINALmade dharmaNo ratings yet
- Babesiosis in Pregnancy: An Imitator of HELLP SyndromeDocument6 pagesBabesiosis in Pregnancy: An Imitator of HELLP Syndromemade dharmaNo ratings yet
- PIIS0002937821019992Document2 pagesPIIS0002937821019992made dharmaNo ratings yet
- IJAISR210509Document13 pagesIJAISR210509made dharmaNo ratings yet
- Original Research Paper AyurvedaDocument3 pagesOriginal Research Paper Ayurvedamade dharmaNo ratings yet
- Journal GAJOMSDocument6 pagesJournal GAJOMSmade dharmaNo ratings yet
- 60d587530e3c120210625article - PDF - FileStudy of Maternal and Perinatal OutcomDocument4 pages60d587530e3c120210625article - PDF - FileStudy of Maternal and Perinatal Outcommade dharmaNo ratings yet
- Laporan Kasus Keratokonjungtivitis Atopik Dengan Limbal Stem Cell Deficiency - ViorasusiDocument10 pagesLaporan Kasus Keratokonjungtivitis Atopik Dengan Limbal Stem Cell Deficiency - Viorasusimade dharmaNo ratings yet
- Kopi-O: Seating ProductsDocument8 pagesKopi-O: Seating Productsishanj1991No ratings yet
- Fuzzy AHP Approach For Selecting The Suitable Bridge Construction MethodDocument8 pagesFuzzy AHP Approach For Selecting The Suitable Bridge Construction Methoda_sarfarazNo ratings yet
- LAW 323-Tax Law-Akhtar AliDocument5 pagesLAW 323-Tax Law-Akhtar AliMuhammad Irfan RiazNo ratings yet
- FSC International StandardDocument15 pagesFSC International StandardEMINANo ratings yet
- Results For Sri Lakshmi Chennakesava Tirupatham - Rajahmundry - Zonalinfo2Document2 pagesResults For Sri Lakshmi Chennakesava Tirupatham - Rajahmundry - Zonalinfo2SRINIVASARAO JONNALANo ratings yet
- Cisco Cloud DefinitionDocument72 pagesCisco Cloud DefinitionmienmobkNo ratings yet
- Carl Størmer's Auroral Discoveries: Alv Egeland and William J. BurkeDocument9 pagesCarl Størmer's Auroral Discoveries: Alv Egeland and William J. BurkesantiagoNo ratings yet
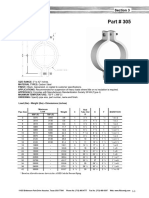
- Part 305 Heavy Pipe ClampDocument1 pagePart 305 Heavy Pipe ClampezhiljananiNo ratings yet
- Asian School Change in Profit Sharing Ratio Sample PaperDocument2 pagesAsian School Change in Profit Sharing Ratio Sample PaperMan your voice is breaking kuttyNo ratings yet
- Notes On The Marsh-BellDocument11 pagesNotes On The Marsh-BellTimóteo ThoberNo ratings yet
- Quantum NavigationDocument94 pagesQuantum NavigationVivek Ag100% (1)
- Resume Goutam AdwantDocument3 pagesResume Goutam AdwantGoutamNo ratings yet
- 2.1.c.ii. Theory of Liming and UnhairingDocument5 pages2.1.c.ii. Theory of Liming and UnhairingAnanthNo ratings yet
- Hands On 3.1 ActDocument7 pagesHands On 3.1 Actmarkkyle collantesNo ratings yet
- Transpo Case Digest 6Document2 pagesTranspo Case Digest 6kizh5mytNo ratings yet
- Oil and Gas ExplorationDocument87 pagesOil and Gas ExplorationVanix DesuasidoNo ratings yet
- Vincent Van GoghDocument6 pagesVincent Van Goghfrancy sharonNo ratings yet
- Casing Collar LocatorDocument1 pageCasing Collar LocatorVu Tuan PhongNo ratings yet
- Al Tronic Ill-Cpu Medium Engines, 2 16 Cylinders Service Instructions FORM Alii-CPU SL 4-91Document8 pagesAl Tronic Ill-Cpu Medium Engines, 2 16 Cylinders Service Instructions FORM Alii-CPU SL 4-91SMcNo ratings yet
- Continuous Line Graphs Lesson Plan 1Document2 pagesContinuous Line Graphs Lesson Plan 1api-491069377No ratings yet
- MDC Monthly Proposal Dec 2019Document2 pagesMDC Monthly Proposal Dec 2019Tushar Prakash ChaudhariNo ratings yet
- Combined Surface and Subsea P&P Test No. 2Document36 pagesCombined Surface and Subsea P&P Test No. 2tonyNo ratings yet
- NCERT Solutions For Class 12 Physics Chapter 3 Current ElectricityDocument24 pagesNCERT Solutions For Class 12 Physics Chapter 3 Current ElectricityDileep GNo ratings yet
- 11-SuperCritical Fluid ChromatographyDocument6 pages11-SuperCritical Fluid ChromatographyGopiNo ratings yet
- CSR Policy KsfeDocument6 pagesCSR Policy KsfeOhari NikshepamNo ratings yet
- RMS Titanic Was A British Passenger: Olympic - Class Ocean LinersDocument1 pageRMS Titanic Was A British Passenger: Olympic - Class Ocean Linersandreea uNo ratings yet
- B. 10 Situation - Care of Client With Problems in Metabolism & Endocrine Functioning.Document7 pagesB. 10 Situation - Care of Client With Problems in Metabolism & Endocrine Functioning.SOLEIL LOUISE LACSON MARBAS100% (1)