Download as pdf or txt
You might also like
- 343 - StatStripINT 1.75 GLU KET 7 - 13Document6 pages343 - StatStripINT 1.75 GLU KET 7 - 13Digitacion EvaNo ratings yet
- 2014 IIHTTDesignand MethodsDocument12 pages2014 IIHTTDesignand MethodsSIMON PEREZ LOPEZNo ratings yet
- The Laryngoscope - 2019 - XieDocument6 pagesThe Laryngoscope - 2019 - XieLNo ratings yet
- Prognostic Factors in ALS A Critical ReviewDocument22 pagesPrognostic Factors in ALS A Critical ReviewJaque LineNo ratings yet
- 2017 ParkDocument8 pages2017 ParkRahul GoyalNo ratings yet
- Fneur 13 962376Document8 pagesFneur 13 962376Miss AmyNo ratings yet
- Alcohol Flushing Syndrome Is Significantly Associated With Intracranial Aneurysm Rupture in The Chinese Han PopulationDocument9 pagesAlcohol Flushing Syndrome Is Significantly Associated With Intracranial Aneurysm Rupture in The Chinese Han PopulationKasturi SriramNo ratings yet
- Chen 2018Document10 pagesChen 2018Maximiliano MahardhikaNo ratings yet
- Perdida Auditiva Por RuidoDocument3 pagesPerdida Auditiva Por RuidotmorlmisatoNo ratings yet
- Hearing LossDocument12 pagesHearing LossFirdha Aulia NisaNo ratings yet
- Presentasi Kasus Sudden Deafness Dhana 2017Document9 pagesPresentasi Kasus Sudden Deafness Dhana 2017Pradhana FwNo ratings yet
- SSNHL EmergensiDocument8 pagesSSNHL EmergensiYayan AkhyarNo ratings yet
- Sudden Deafness 2Document8 pagesSudden Deafness 2Aldhi Putra PradanaNo ratings yet
- s13063 020 04579 6Document11 pagess13063 020 04579 6BTS LGONo ratings yet
- Dapus 6 Referat 1Document6 pagesDapus 6 Referat 1Akramanto RidwanNo ratings yet
- Umesh Synopsis NewDocument22 pagesUmesh Synopsis NewChitra gayathri.nNo ratings yet
- Predictive Factors For Recovery in Idiopathic Sudden Sensory Neural Hearing LossDocument8 pagesPredictive Factors For Recovery in Idiopathic Sudden Sensory Neural Hearing LossMiss AmyNo ratings yet
- AutoimmuneDocument10 pagesAutoimmuneapi-526465275No ratings yet
- IJC Heart & VasculatureDocument2 pagesIJC Heart & VasculatureGledia LindaNo ratings yet
- Batson2017 OtosclerosisDocument6 pagesBatson2017 OtosclerosisnuhajazminNo ratings yet
- Journal Homepage: - : IntroductionDocument31 pagesJournal Homepage: - : IntroductionIJAR JOURNALNo ratings yet
- Jao 21 9Document7 pagesJao 21 9Miss AmyNo ratings yet
- Sudden Deafness JournalDocument2 pagesSudden Deafness JournalRestiNo ratings yet
- Systematic Review of The Evidence For The Etiology of Adult Sudden Sensorineural Hearing LossDocument11 pagesSystematic Review of The Evidence For The Etiology of Adult Sudden Sensorineural Hearing Lossronaldyohanesf87No ratings yet
- estudio KoreaDocument9 pagesestudio KoreaLaura Sofía Miranda RellánNo ratings yet
- Obstructive Sleep ApneaDocument21 pagesObstructive Sleep ApneaIJAR JOURNALNo ratings yet
- Association of Midlife Hypertension With Late-Life Hearing LossDocument8 pagesAssociation of Midlife Hypertension With Late-Life Hearing Lossharyo wiryantoNo ratings yet
- Jurnal 1 Titin SuhartinaDocument8 pagesJurnal 1 Titin SuhartinaTitinNo ratings yet
- Systemic Lupus Erythematosus and Hearing Disorders: Literature Review and Meta-Analysis of Clinical and Temporal Bone FindingsDocument11 pagesSystemic Lupus Erythematosus and Hearing Disorders: Literature Review and Meta-Analysis of Clinical and Temporal Bone FindingsLNo ratings yet
- The Relationship Between Serum Lipids and Sudden Sensorineural Hearing Loss: A Systematic Review and Meta-AnalysisDocument11 pagesThe Relationship Between Serum Lipids and Sudden Sensorineural Hearing Loss: A Systematic Review and Meta-AnalysisDenny LukasNo ratings yet
- The Clinical Value of A Thorough Diagnostic Evalua 2019 American Journal ofDocument6 pagesThe Clinical Value of A Thorough Diagnostic Evalua 2019 American Journal ofGhulam GilmaniNo ratings yet
- American Journal of Otolaryngology-Head and Neck Medicine and SurgeryDocument6 pagesAmerican Journal of Otolaryngology-Head and Neck Medicine and SurgeryMamadou FayeNo ratings yet
- Das 2019Document6 pagesDas 2019KarenNo ratings yet
- Seminar: Benjamin E Schreiber, Charlotte Agrup, Dorian O Haskard, Linda M LuxonDocument9 pagesSeminar: Benjamin E Schreiber, Charlotte Agrup, Dorian O Haskard, Linda M Luxonmaria_garaveNo ratings yet
- A2 - Loi, 2021Document8 pagesA2 - Loi, 2021bayu seno ajiNo ratings yet
- Ahl N DepressionDocument7 pagesAhl N DepressionDr Pavina RayamajhiNo ratings yet
- Siadh CSWSDocument11 pagesSiadh CSWStsanikawaiNo ratings yet
- Screening para Biomarcadores Asociado A EVC Isquemico en Fibrilacion AuricularDocument41 pagesScreening para Biomarcadores Asociado A EVC Isquemico en Fibrilacion AuricularAdán TreminioNo ratings yet
- Otolaryngol - Head Neck Surg - 2020 - Basura - Clinical Practice Guideline M Ni Re S DiseaseDocument56 pagesOtolaryngol - Head Neck Surg - 2020 - Basura - Clinical Practice Guideline M Ni Re S DiseaseTruong Ngoc HuyNo ratings yet
- Mortality Rates in Patients With Anorexia Nervosa and Other Eating Disorders A Meta-Analysis of 36 StudiesDocument9 pagesMortality Rates in Patients With Anorexia Nervosa and Other Eating Disorders A Meta-Analysis of 36 StudiesANDREA GISSELA CHAMORRO DIONICIONo ratings yet
- Fneur 13 853054Document8 pagesFneur 13 853054RAFAEL BRITONo ratings yet
- Intralabyrinthine Schwannoma Distinct Features For Differential DiagnosisDocument8 pagesIntralabyrinthine Schwannoma Distinct Features For Differential DiagnosisvsberraondoNo ratings yet
- Ginjal 3Document11 pagesGinjal 3wonderNo ratings yet
- Alzheimers Disease and Dental ManagementDocument5 pagesAlzheimers Disease and Dental ManagementMalu OliveiraNo ratings yet
- Fneur 15 1360385Document11 pagesFneur 15 1360385arif 2006No ratings yet
- Surdite Drepano SsDocument6 pagesSurdite Drepano SsMamadou FayeNo ratings yet
- Management of Adult Sensorineural Hearing Loss: EtiologiesDocument10 pagesManagement of Adult Sensorineural Hearing Loss: EtiologiesaldimugniNo ratings yet
- Samtani, 2022Document25 pagesSamtani, 2022candela pelaezNo ratings yet
- Sudden Hearing Loss WordDocument56 pagesSudden Hearing Loss WordjustuareNo ratings yet
- Applications of Nanotechnology in The Treatment ofDocument15 pagesApplications of Nanotechnology in The Treatment oflolaNo ratings yet
- Rivers Auty2020Document25 pagesRivers Auty2020Nadia SaiNo ratings yet
- Dementia Incidence and Population-Attributable Fraction For Dementia Risk Factors in Republic of Korea A 12-Year Longitudinal Follow-Up Study of A National CohortDocument10 pagesDementia Incidence and Population-Attributable Fraction For Dementia Risk Factors in Republic of Korea A 12-Year Longitudinal Follow-Up Study of A National CohortDrHellenNo ratings yet
- Oa PDFDocument7 pagesOa PDFFrandy HuangNo ratings yet
- Noise-Induced Hearing LossDocument34 pagesNoise-Induced Hearing LossKiswah YohanaNo ratings yet
- Noise 4Document34 pagesNoise 4NIKOLAOS CHATZAKISNo ratings yet
- Fix Journal 1Document14 pagesFix Journal 1Lavenia Ellein MokiwangNo ratings yet
- Otology: Special Paper in Celebration of Prof. Yang'S 50 Years Career in MedicineDocument6 pagesOtology: Special Paper in Celebration of Prof. Yang'S 50 Years Career in Medicinechipta lestariNo ratings yet
- 2021 - M Risal - Relationship Between Family Support and Self-Care Among Non Hemorrhagic Stroke PatientsDocument8 pages2021 - M Risal - Relationship Between Family Support and Self-Care Among Non Hemorrhagic Stroke PatientsMaudia IndrianiiNo ratings yet
- CNS Neuroscience Therapeutics - 2024 - Xu - The Use of Optical Coherence Tomography OCT and OCT Angiography inDocument9 pagesCNS Neuroscience Therapeutics - 2024 - Xu - The Use of Optical Coherence Tomography OCT and OCT Angiography inJuanma CarasaNo ratings yet
- Genicular Nerve Ablation Zeitlinger2019Document7 pagesGenicular Nerve Ablation Zeitlinger2019drjorgewtorresNo ratings yet
- Small Fiber Neuropathy and Related Syndromes: Pain and NeurodegenerationFrom EverandSmall Fiber Neuropathy and Related Syndromes: Pain and NeurodegenerationSung-Tsang HsiehNo ratings yet
- UntitledDocument13 pagesUntitledmarcos crescencioNo ratings yet
- Uc201707281ee Rev C Minimed 640g Getting Started GuideDocument35 pagesUc201707281ee Rev C Minimed 640g Getting Started Guidejulio geraldoNo ratings yet
- Preventing Chronic Disease:: Physical Activity and Healthy EatingDocument54 pagesPreventing Chronic Disease:: Physical Activity and Healthy EatingCHANGEZ KHAN SARDARNo ratings yet
- Assessment Diagnosis Planning Intervention Rationale EvaluationDocument4 pagesAssessment Diagnosis Planning Intervention Rationale EvaluationChristine LebicoNo ratings yet
- Diabetes: Statistics Symptoms Causes Diagnosis PreventionDocument67 pagesDiabetes: Statistics Symptoms Causes Diagnosis PreventionShanthi_KVNo ratings yet
- Babor. Belen. Bulaklak. Estayan. Guevarra, M. Guevarra, S. Juaneza. MalvarDocument34 pagesBabor. Belen. Bulaklak. Estayan. Guevarra, M. Guevarra, S. Juaneza. MalvarElla DevezaNo ratings yet
- Applied Chemistry Quarter 4Document8 pagesApplied Chemistry Quarter 4Now OnwooNo ratings yet
- Walsh2015association of Diabetic Foot Ulcer and Death in A Population-Based Cohort From The United KingdomDocument6 pagesWalsh2015association of Diabetic Foot Ulcer and Death in A Population-Based Cohort From The United KingdomAnonymous SMLzNANo ratings yet
- ADA Medication Profiles and Side EffectsDocument1 pageADA Medication Profiles and Side EffectsHillariNo ratings yet
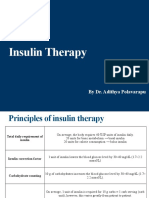
- Insulin Therapy: by Dr. Adithya PolavarapuDocument18 pagesInsulin Therapy: by Dr. Adithya Polavarapuadithya polavarapuNo ratings yet
- Rybelsus Product MedicalDocument58 pagesRybelsus Product MedicalNovo NORDISK BalajiNo ratings yet
- Theme 1: Role of Betaine in Controlling Gestational Diabetes MellitusDocument9 pagesTheme 1: Role of Betaine in Controlling Gestational Diabetes MellitusBhargav MosesNo ratings yet
- SBI242 - Week 9 Kahoot's QuizDocument3 pagesSBI242 - Week 9 Kahoot's Quizjessicalrogers01No ratings yet
- Assignment NO # 04: Subject: EchocardiographyDocument3 pagesAssignment NO # 04: Subject: EchocardiographyANAM IQBALNo ratings yet
- Diabetes Mellitus and Laboratory Tests of DiabetesDocument24 pagesDiabetes Mellitus and Laboratory Tests of DiabetesturkiNo ratings yet
- Empagliflozin Prescribing InformationDocument35 pagesEmpagliflozin Prescribing InformationMohammed Shamiul ShahidNo ratings yet
- Practical Biochemistry: Number of Experiment: (1) Name of Exp.:-Blood Glucose TestDocument6 pagesPractical Biochemistry: Number of Experiment: (1) Name of Exp.:-Blood Glucose TestHiba EmadNo ratings yet
- Nurs FPX 4030 Assessment 3 Pico T Questions and An Evidence Based ApproachDocument5 pagesNurs FPX 4030 Assessment 3 Pico T Questions and An Evidence Based Approachjoohnsmith070No ratings yet
- Demographic and Clinical Features of Diabetes Mellitus in 1095 Yemeni PatientsDocument9 pagesDemographic and Clinical Features of Diabetes Mellitus in 1095 Yemeni PatientsRoaaNo ratings yet
- Class 8 Comprehension Passage - Practice Worksheet I. Read The Passage and Answer The Questions That FollowDocument3 pagesClass 8 Comprehension Passage - Practice Worksheet I. Read The Passage and Answer The Questions That FollowDharini KrishnamoorthyNo ratings yet
- Module 4 Assignment PosterDocument1 pageModule 4 Assignment PosterChelsie Rachelle BrownNo ratings yet
- A Review of GLP-1 Receptor Agonists in Type 2 DiabDocument11 pagesA Review of GLP-1 Receptor Agonists in Type 2 Diab이호원No ratings yet
- Horm S 23 00313 1Document32 pagesHorm S 23 00313 1andreopNo ratings yet
- Diaba Health - 2a FinalDocument19 pagesDiaba Health - 2a FinalK StoriesNo ratings yet
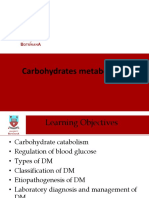
- Lecture 6 Carbohydrate MetabolismDocument36 pagesLecture 6 Carbohydrate MetabolismDuduetsang MosalakataneNo ratings yet
- List of AbrevationDocument25 pagesList of AbrevationNhänâ FrëshNo ratings yet
- Dapagliflozin HFpEF Journal ClubDocument22 pagesDapagliflozin HFpEF Journal ClubRaquel WeinbergNo ratings yet
- Biology Chapter 3Document26 pagesBiology Chapter 3SajithKumarVariathNo ratings yet
- PhysioEx Exercise 4 Activity 2Document4 pagesPhysioEx Exercise 4 Activity 2PabloAndresPalaciosAgilaNo ratings yet