
School Health Examination Card: Nutritional Status (NS) (BMI/Weight-for-Age)
School Health Examination Card: Nutritional Status (NS) (BMI/Weight-for-Age)
You might also like
- English SBADocument7 pagesEnglish SBAnaseeb60% (169)
- Dental Health CardDocument3 pagesDental Health Cardodessa delos santos100% (1)
- 2021 Vaccine Exemption Form LetterDocument1 page2021 Vaccine Exemption Form Lettermaria100% (2)
- SHD Form 2Document44 pagesSHD Form 2Kristoffer Alcantara Rivera100% (9)
- PerDev - Q2 - Module 3Document45 pagesPerDev - Q2 - Module 3jeysel calumbaNo ratings yet
- Skin Assessment FormDocument2 pagesSkin Assessment FormOng KarlNo ratings yet
- School Health Examination Card: Republic of The Philippines Department of EducationDocument4 pagesSchool Health Examination Card: Republic of The Philippines Department of EducationJunard Asentista100% (2)
- School Health Card 2018Document39 pagesSchool Health Card 2018klaircruz100% (1)
- Complete Dentures - Extraoral ExamDocument8 pagesComplete Dentures - Extraoral ExamlindaNo ratings yet
- Student Name: - Date: - Evaluator Name: - Skill Performance Checklist: HEENT ExaminationDocument2 pagesStudent Name: - Date: - Evaluator Name: - Skill Performance Checklist: HEENT ExaminationAji PicanteNo ratings yet
- 2019 ARNG Enlistment ApplicationDocument29 pages2019 ARNG Enlistment Applicationmaximilian.zandynNo ratings yet
- Fraud On The Court by An Officer of The CourtDocument2 pagesFraud On The Court by An Officer of The CourtTerry Green100% (3)
- Leetcode Solutions in JavaDocument2 pagesLeetcode Solutions in JavaKunal KapoorNo ratings yet
- Name: - LRNDocument2 pagesName: - LRNjrose fay amatNo ratings yet
- H I-FORMfinalELEMENTARYDocument2 pagesH I-FORMfinalELEMENTARYKAYE ANNE AMORANTONo ratings yet
- Health Examination FormDocument4 pagesHealth Examination FormVangie MarikitNo ratings yet
- Elem Sec Health CardsDocument17 pagesElem Sec Health CardsMary Grace CalipesNo ratings yet
- Sdo PM QF Sgod SHN 001 Students Health Card ElementaryDocument3 pagesSdo PM QF Sgod SHN 001 Students Health Card ElementaryShiela E. EladNo ratings yet
- DentalAssistantHealthFormDocument4 pagesDentalAssistantHealthFormcr littleNo ratings yet
- Elementary Health CardDocument1 pageElementary Health CardJennyRose AmistadNo ratings yet
- School Health Examination Card: Bureau of Learner Support Services - School Health DivisionDocument44 pagesSchool Health Examination Card: Bureau of Learner Support Services - School Health DivisionShanaiya CabzNo ratings yet
- New School Health FormsDocument42 pagesNew School Health FormsJoanna MarieNo ratings yet
- Sbip Forms 2019-2020Document14 pagesSbip Forms 2019-2020Princess May Olea ItaliaNo ratings yet
- SBFP - OK Sa DepEd Division UpdateDocument44 pagesSBFP - OK Sa DepEd Division UpdateOcir AyaberNo ratings yet
- SHN Form 001 School Health Examination Card ElementaryDocument2 pagesSHN Form 001 School Health Examination Card ElementaryJohn BunayNo ratings yet
- Health Card FrontDocument3 pagesHealth Card FrontCarlaGomezNo ratings yet
- HealthDocument16 pagesHealthMaria Lucille Mejias IINo ratings yet
- Name: Region/Division: Date of Birth: Address: School Address: Laguile, Taal, Batangas Name of Parent/GuardianDocument1 pageName: Region/Division: Date of Birth: Address: School Address: Laguile, Taal, Batangas Name of Parent/GuardiankristineNo ratings yet
- School Health Examination Card: Republic of The Philippines Department of EducationDocument44 pagesSchool Health Examination Card: Republic of The Philippines Department of EducationelizabethNo ratings yet
- Common Medical PrefixesDocument5 pagesCommon Medical PrefixesRoshua DaclanNo ratings yet
- College of Nursing: Collecting and Clustering Objective Data (Initial Comprehensive P.E. - Ippa)Document2 pagesCollege of Nursing: Collecting and Clustering Objective Data (Initial Comprehensive P.E. - Ippa)Carolyn CalupitanNo ratings yet
- Area Assessment Description of Findings & Interpretation General Appearance PostureDocument7 pagesArea Assessment Description of Findings & Interpretation General Appearance PostureMica OmotsosircNo ratings yet
- Different Types of FaciesDocument9 pagesDifferent Types of FaciesSwati Pathak GiriNo ratings yet
- Swallowing ChecklistsDocument5 pagesSwallowing ChecklistsTaylor MayNo ratings yet
- Initial Examination Form: Jordan University of Science & Technology Faculty of Dentistry Dental Teaching CenterDocument2 pagesInitial Examination Form: Jordan University of Science & Technology Faculty of Dentistry Dental Teaching Centersadeen2249No ratings yet
- Initial Examination Form: Jordan University of Science & Technology Faculty of Dentistry Dental Teaching CenterDocument2 pagesInitial Examination Form: Jordan University of Science & Technology Faculty of Dentistry Dental Teaching Centersadeen2249No ratings yet
- Initial Examination Form: Jordan University of Science & Technology Faculty of Dentistry Dental Teaching CenterDocument2 pagesInitial Examination Form: Jordan University of Science & Technology Faculty of Dentistry Dental Teaching Centersadeen2249No ratings yet
- Student Admission Form Messila 1Document3 pagesStudent Admission Form Messila 1everestNo ratings yet
- Final Year Clinicals: Malocclusions and Etiology (Graber)Document31 pagesFinal Year Clinicals: Malocclusions and Etiology (Graber)Sruthy NairNo ratings yet
- Matary Surgery Summary - 2012 PDFDocument365 pagesMatary Surgery Summary - 2012 PDFfayiz1982No ratings yet
- ENT Skill SheetDocument1 pageENT Skill SheetMuhammed ElgasimNo ratings yet
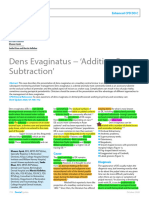
- Dens EvaginatusDocument5 pagesDens EvaginatusFatima AliNo ratings yet
- In Consortium With N. Bacalso Ave. Cor Panganiban ST., 6000 Cebu City, Cebu, Philippines Tel. Nos. (032) 316-5128/ (032) 4186105 Email AddressDocument5 pagesIn Consortium With N. Bacalso Ave. Cor Panganiban ST., 6000 Cebu City, Cebu, Philippines Tel. Nos. (032) 316-5128/ (032) 4186105 Email AddressCarl Jayson LeysonNo ratings yet
- Physical Assessment GuidelinesDocument3 pagesPhysical Assessment Guidelinesyjjkbx9vypNo ratings yet
- Initial Patient History ChecklistDocument1 pageInitial Patient History Checklistinfo7588No ratings yet
- Area Assessment Description of Findings & Interpretation General Appearance PostureDocument6 pagesArea Assessment Description of Findings & Interpretation General Appearance PostureZAY EMNo ratings yet
- Instant Download PDF Dental Assisting A Comprehensive Approach 5th Edition Phinney Test Bank Full ChapterDocument56 pagesInstant Download PDF Dental Assisting A Comprehensive Approach 5th Edition Phinney Test Bank Full Chapterzvikpleisa100% (4)
- Lab Guide: Head, Face, and Neck AssessmentDocument5 pagesLab Guide: Head, Face, and Neck AssessmentDaisy MellaNo ratings yet
- HypohidroticDocument1 pageHypohidroticHimanshu GaikwadNo ratings yet
- (ENT) 2.05 Diseases of The Oral Cavity - DR - CalaveraDocument12 pages(ENT) 2.05 Diseases of The Oral Cavity - DR - CalaveraNoreen Hannah GabrielNo ratings yet
- Ebook Dental Assisting A Comprehensive Approach 5Th Edition Phinney Test Bank Full Chapter PDFDocument54 pagesEbook Dental Assisting A Comprehensive Approach 5Th Edition Phinney Test Bank Full Chapter PDFsauflyallowerrf1qs100% (14)
- Ophthalmology Case Profoma - AgamDocument8 pagesOphthalmology Case Profoma - AgamHarshitha ANo ratings yet
- Assessment ToolDocument2 pagesAssessment ToolSarah CruzNo ratings yet
- Term 2 Year 7 Classification HW BOOKDocument8 pagesTerm 2 Year 7 Classification HW BOOKSia GuptaNo ratings yet
- New Normal Health Assessment Form For Learners 2020 RegionDocument4 pagesNew Normal Health Assessment Form For Learners 2020 RegionCleofe Mae Piñero AseñasNo ratings yet
- Dental Anomalies ملخصDocument8 pagesDental Anomalies ملخصهند عبداللهNo ratings yet
- Miracle Hill Medical Center: DashboardDocument43 pagesMiracle Hill Medical Center: Dashboardmarcojempleo019No ratings yet
- Nur 101 Data Base 1Document23 pagesNur 101 Data Base 1api-337919180No ratings yet
- AbbreviationsDocument11 pagesAbbreviationsSara MarinNo ratings yet
- Cleft Lip and Cleft PalateDocument54 pagesCleft Lip and Cleft Palatedr parveen bathla100% (3)
- Retdem Physical AssessmentDocument6 pagesRetdem Physical AssessmentTrishia May DanaoNo ratings yet
- AllergyQuestionnaire PDFDocument2 pagesAllergyQuestionnaire PDFCrazy about JunglesNo ratings yet
- New Patient Forms Package1Document2 pagesNew Patient Forms Package1Ache HNo ratings yet
- Cardio Respiratory Asessment For PhysiotDocument10 pagesCardio Respiratory Asessment For PhysiotJayden HiiNo ratings yet
- ENGLISH3 Q2 MOD5 MeettheConsonantDiagraphschandsh v4Document22 pagesENGLISH3 Q2 MOD5 MeettheConsonantDiagraphschandsh v4April Rose CaballeroNo ratings yet
- English3 Q2 Mod3 Wordswithinitialandfinalconsonantblends v3Document34 pagesEnglish3 Q2 Mod3 Wordswithinitialandfinalconsonantblends v3April Rose CaballeroNo ratings yet
- ENGLISH3 Q2 MOD4 CommonSightWords v3Document16 pagesENGLISH3 Q2 MOD4 CommonSightWords v3April Rose CaballeroNo ratings yet
- Different Types of Business CommunicationDocument10 pagesDifferent Types of Business CommunicationApril Rose CaballeroNo ratings yet
- Support Material Learning Activity 1: Aspects Vocabulary ExamplesDocument9 pagesSupport Material Learning Activity 1: Aspects Vocabulary ExamplesEmmanuel Campos OsorioNo ratings yet
- ZaslawDocument23 pagesZaslawRamiro Vera SepulvedaNo ratings yet
- Unit 2Document8 pagesUnit 2Ansuman SamalNo ratings yet
- Operaion Case 1Document2 pagesOperaion Case 1Maulesh PatelNo ratings yet
- He Graph Below Shows Radio and Television Audiences Throughout The Day in 1992Document4 pagesHe Graph Below Shows Radio and Television Audiences Throughout The Day in 1992Armanai KhamzinaNo ratings yet
- Stephen SONDEM NATIONAL HUMAN RIGHTS INSTITUTIONS - THE GHANAIAN EXPERIENCEDocument17 pagesStephen SONDEM NATIONAL HUMAN RIGHTS INSTITUTIONS - THE GHANAIAN EXPERIENCECentre for Regional Policy Research and Cooperation StudiorumNo ratings yet
- Calendar ConversionDocument40 pagesCalendar Conversionjake100% (1)
- Japan and SexDocument6 pagesJapan and SexRicardoParraoNo ratings yet
- THE WOMAN IN BLACK Last VersionDocument11 pagesTHE WOMAN IN BLACK Last VersionavilamarialuzNo ratings yet
- Mus189 Concert Comparison Assignment GuidelinesDocument3 pagesMus189 Concert Comparison Assignment Guidelinesapi-300390896No ratings yet
- 9 EeeDocument82 pages9 EeeRiya AgrawalNo ratings yet
- IIM Calcutta Recruitment Brochure 2015Document17 pagesIIM Calcutta Recruitment Brochure 2015Sankalp Akash SinghNo ratings yet
- Political OrganizationsDocument15 pagesPolitical Organizationsastherielle cameroNo ratings yet
- Implicit DifferentiationDocument12 pagesImplicit DifferentiationNaitsirc UluputipanNo ratings yet
- Intro To Human Computer InteractionDocument53 pagesIntro To Human Computer InteractionKanit WongsuphasasawatNo ratings yet
- Ethical Disintegration of Enron: PHI 401: Business EthicsDocument14 pagesEthical Disintegration of Enron: PHI 401: Business EthicsAnikaNo ratings yet
- 新概念英语第三册全部语法Document47 pages新概念英语第三册全部语法蔣偉宏No ratings yet
- RupDocument52 pagesRupmojtaba7No ratings yet
- 1 LogicDocument9 pages1 Logicakash vermaNo ratings yet
- Godel Escher Bach Ebook ItaDocument4 pagesGodel Escher Bach Ebook ItaJulie0% (1)
- Design Life vs. Seismic Return PeriodDocument19 pagesDesign Life vs. Seismic Return PeriodShivamMishraNo ratings yet
- APA Jamii Plus Family Medical Cover BrochureDocument8 pagesAPA Jamii Plus Family Medical Cover BrochureADANARABOW100% (1)
- Difference Between Precis WritingDocument2 pagesDifference Between Precis WritingNauman MashwaniNo ratings yet
- PVH EuropeDocument1 pagePVH Europeapi-237852926No ratings yet
- SdasasasDocument22 pagesSdasasasGianne Robert MalavegaNo ratings yet


























































































Download as docx, pdf, or txt
You might also like
- English SBADocument7 pagesEnglish SBAnaseeb60% (169)
- Dental Health CardDocument3 pagesDental Health Cardodessa delos santos100% (1)
- 2021 Vaccine Exemption Form LetterDocument1 page2021 Vaccine Exemption Form Lettermaria100% (2)
- SHD Form 2Document44 pagesSHD Form 2Kristoffer Alcantara Rivera100% (9)
- PerDev - Q2 - Module 3Document45 pagesPerDev - Q2 - Module 3jeysel calumbaNo ratings yet
- Skin Assessment FormDocument2 pagesSkin Assessment FormOng KarlNo ratings yet
- School Health Examination Card: Republic of The Philippines Department of EducationDocument4 pagesSchool Health Examination Card: Republic of The Philippines Department of EducationJunard Asentista100% (2)
- School Health Card 2018Document39 pagesSchool Health Card 2018klaircruz100% (1)
- Complete Dentures - Extraoral ExamDocument8 pagesComplete Dentures - Extraoral ExamlindaNo ratings yet
- Student Name: - Date: - Evaluator Name: - Skill Performance Checklist: HEENT ExaminationDocument2 pagesStudent Name: - Date: - Evaluator Name: - Skill Performance Checklist: HEENT ExaminationAji PicanteNo ratings yet
- 2019 ARNG Enlistment ApplicationDocument29 pages2019 ARNG Enlistment Applicationmaximilian.zandynNo ratings yet
- Fraud On The Court by An Officer of The CourtDocument2 pagesFraud On The Court by An Officer of The CourtTerry Green100% (3)
- Leetcode Solutions in JavaDocument2 pagesLeetcode Solutions in JavaKunal KapoorNo ratings yet
- Name: - LRNDocument2 pagesName: - LRNjrose fay amatNo ratings yet
- H I-FORMfinalELEMENTARYDocument2 pagesH I-FORMfinalELEMENTARYKAYE ANNE AMORANTONo ratings yet
- Health Examination FormDocument4 pagesHealth Examination FormVangie MarikitNo ratings yet
- Elem Sec Health CardsDocument17 pagesElem Sec Health CardsMary Grace CalipesNo ratings yet
- Sdo PM QF Sgod SHN 001 Students Health Card ElementaryDocument3 pagesSdo PM QF Sgod SHN 001 Students Health Card ElementaryShiela E. EladNo ratings yet
- DentalAssistantHealthFormDocument4 pagesDentalAssistantHealthFormcr littleNo ratings yet
- Elementary Health CardDocument1 pageElementary Health CardJennyRose AmistadNo ratings yet
- School Health Examination Card: Bureau of Learner Support Services - School Health DivisionDocument44 pagesSchool Health Examination Card: Bureau of Learner Support Services - School Health DivisionShanaiya CabzNo ratings yet
- New School Health FormsDocument42 pagesNew School Health FormsJoanna MarieNo ratings yet
- Sbip Forms 2019-2020Document14 pagesSbip Forms 2019-2020Princess May Olea ItaliaNo ratings yet
- SBFP - OK Sa DepEd Division UpdateDocument44 pagesSBFP - OK Sa DepEd Division UpdateOcir AyaberNo ratings yet
- SHN Form 001 School Health Examination Card ElementaryDocument2 pagesSHN Form 001 School Health Examination Card ElementaryJohn BunayNo ratings yet
- Health Card FrontDocument3 pagesHealth Card FrontCarlaGomezNo ratings yet
- HealthDocument16 pagesHealthMaria Lucille Mejias IINo ratings yet
- Name: Region/Division: Date of Birth: Address: School Address: Laguile, Taal, Batangas Name of Parent/GuardianDocument1 pageName: Region/Division: Date of Birth: Address: School Address: Laguile, Taal, Batangas Name of Parent/GuardiankristineNo ratings yet
- School Health Examination Card: Republic of The Philippines Department of EducationDocument44 pagesSchool Health Examination Card: Republic of The Philippines Department of EducationelizabethNo ratings yet
- Common Medical PrefixesDocument5 pagesCommon Medical PrefixesRoshua DaclanNo ratings yet
- College of Nursing: Collecting and Clustering Objective Data (Initial Comprehensive P.E. - Ippa)Document2 pagesCollege of Nursing: Collecting and Clustering Objective Data (Initial Comprehensive P.E. - Ippa)Carolyn CalupitanNo ratings yet
- Area Assessment Description of Findings & Interpretation General Appearance PostureDocument7 pagesArea Assessment Description of Findings & Interpretation General Appearance PostureMica OmotsosircNo ratings yet
- Different Types of FaciesDocument9 pagesDifferent Types of FaciesSwati Pathak GiriNo ratings yet
- Swallowing ChecklistsDocument5 pagesSwallowing ChecklistsTaylor MayNo ratings yet
- Initial Examination Form: Jordan University of Science & Technology Faculty of Dentistry Dental Teaching CenterDocument2 pagesInitial Examination Form: Jordan University of Science & Technology Faculty of Dentistry Dental Teaching Centersadeen2249No ratings yet
- Initial Examination Form: Jordan University of Science & Technology Faculty of Dentistry Dental Teaching CenterDocument2 pagesInitial Examination Form: Jordan University of Science & Technology Faculty of Dentistry Dental Teaching Centersadeen2249No ratings yet
- Initial Examination Form: Jordan University of Science & Technology Faculty of Dentistry Dental Teaching CenterDocument2 pagesInitial Examination Form: Jordan University of Science & Technology Faculty of Dentistry Dental Teaching Centersadeen2249No ratings yet
- Student Admission Form Messila 1Document3 pagesStudent Admission Form Messila 1everestNo ratings yet
- Final Year Clinicals: Malocclusions and Etiology (Graber)Document31 pagesFinal Year Clinicals: Malocclusions and Etiology (Graber)Sruthy NairNo ratings yet
- Matary Surgery Summary - 2012 PDFDocument365 pagesMatary Surgery Summary - 2012 PDFfayiz1982No ratings yet
- ENT Skill SheetDocument1 pageENT Skill SheetMuhammed ElgasimNo ratings yet
- Dens EvaginatusDocument5 pagesDens EvaginatusFatima AliNo ratings yet
- In Consortium With N. Bacalso Ave. Cor Panganiban ST., 6000 Cebu City, Cebu, Philippines Tel. Nos. (032) 316-5128/ (032) 4186105 Email AddressDocument5 pagesIn Consortium With N. Bacalso Ave. Cor Panganiban ST., 6000 Cebu City, Cebu, Philippines Tel. Nos. (032) 316-5128/ (032) 4186105 Email AddressCarl Jayson LeysonNo ratings yet
- Physical Assessment GuidelinesDocument3 pagesPhysical Assessment Guidelinesyjjkbx9vypNo ratings yet
- Initial Patient History ChecklistDocument1 pageInitial Patient History Checklistinfo7588No ratings yet
- Area Assessment Description of Findings & Interpretation General Appearance PostureDocument6 pagesArea Assessment Description of Findings & Interpretation General Appearance PostureZAY EMNo ratings yet
- Instant Download PDF Dental Assisting A Comprehensive Approach 5th Edition Phinney Test Bank Full ChapterDocument56 pagesInstant Download PDF Dental Assisting A Comprehensive Approach 5th Edition Phinney Test Bank Full Chapterzvikpleisa100% (4)
- Lab Guide: Head, Face, and Neck AssessmentDocument5 pagesLab Guide: Head, Face, and Neck AssessmentDaisy MellaNo ratings yet
- HypohidroticDocument1 pageHypohidroticHimanshu GaikwadNo ratings yet
- (ENT) 2.05 Diseases of The Oral Cavity - DR - CalaveraDocument12 pages(ENT) 2.05 Diseases of The Oral Cavity - DR - CalaveraNoreen Hannah GabrielNo ratings yet
- Ebook Dental Assisting A Comprehensive Approach 5Th Edition Phinney Test Bank Full Chapter PDFDocument54 pagesEbook Dental Assisting A Comprehensive Approach 5Th Edition Phinney Test Bank Full Chapter PDFsauflyallowerrf1qs100% (14)
- Ophthalmology Case Profoma - AgamDocument8 pagesOphthalmology Case Profoma - AgamHarshitha ANo ratings yet
- Assessment ToolDocument2 pagesAssessment ToolSarah CruzNo ratings yet
- Term 2 Year 7 Classification HW BOOKDocument8 pagesTerm 2 Year 7 Classification HW BOOKSia GuptaNo ratings yet
- New Normal Health Assessment Form For Learners 2020 RegionDocument4 pagesNew Normal Health Assessment Form For Learners 2020 RegionCleofe Mae Piñero AseñasNo ratings yet
- Dental Anomalies ملخصDocument8 pagesDental Anomalies ملخصهند عبداللهNo ratings yet
- Miracle Hill Medical Center: DashboardDocument43 pagesMiracle Hill Medical Center: Dashboardmarcojempleo019No ratings yet
- Nur 101 Data Base 1Document23 pagesNur 101 Data Base 1api-337919180No ratings yet
- AbbreviationsDocument11 pagesAbbreviationsSara MarinNo ratings yet
- Cleft Lip and Cleft PalateDocument54 pagesCleft Lip and Cleft Palatedr parveen bathla100% (3)
- Retdem Physical AssessmentDocument6 pagesRetdem Physical AssessmentTrishia May DanaoNo ratings yet
- AllergyQuestionnaire PDFDocument2 pagesAllergyQuestionnaire PDFCrazy about JunglesNo ratings yet
- New Patient Forms Package1Document2 pagesNew Patient Forms Package1Ache HNo ratings yet
- Cardio Respiratory Asessment For PhysiotDocument10 pagesCardio Respiratory Asessment For PhysiotJayden HiiNo ratings yet
- ENGLISH3 Q2 MOD5 MeettheConsonantDiagraphschandsh v4Document22 pagesENGLISH3 Q2 MOD5 MeettheConsonantDiagraphschandsh v4April Rose CaballeroNo ratings yet
- English3 Q2 Mod3 Wordswithinitialandfinalconsonantblends v3Document34 pagesEnglish3 Q2 Mod3 Wordswithinitialandfinalconsonantblends v3April Rose CaballeroNo ratings yet
- ENGLISH3 Q2 MOD4 CommonSightWords v3Document16 pagesENGLISH3 Q2 MOD4 CommonSightWords v3April Rose CaballeroNo ratings yet
- Different Types of Business CommunicationDocument10 pagesDifferent Types of Business CommunicationApril Rose CaballeroNo ratings yet
- Support Material Learning Activity 1: Aspects Vocabulary ExamplesDocument9 pagesSupport Material Learning Activity 1: Aspects Vocabulary ExamplesEmmanuel Campos OsorioNo ratings yet
- ZaslawDocument23 pagesZaslawRamiro Vera SepulvedaNo ratings yet
- Unit 2Document8 pagesUnit 2Ansuman SamalNo ratings yet
- Operaion Case 1Document2 pagesOperaion Case 1Maulesh PatelNo ratings yet
- He Graph Below Shows Radio and Television Audiences Throughout The Day in 1992Document4 pagesHe Graph Below Shows Radio and Television Audiences Throughout The Day in 1992Armanai KhamzinaNo ratings yet
- Stephen SONDEM NATIONAL HUMAN RIGHTS INSTITUTIONS - THE GHANAIAN EXPERIENCEDocument17 pagesStephen SONDEM NATIONAL HUMAN RIGHTS INSTITUTIONS - THE GHANAIAN EXPERIENCECentre for Regional Policy Research and Cooperation StudiorumNo ratings yet
- Calendar ConversionDocument40 pagesCalendar Conversionjake100% (1)
- Japan and SexDocument6 pagesJapan and SexRicardoParraoNo ratings yet
- THE WOMAN IN BLACK Last VersionDocument11 pagesTHE WOMAN IN BLACK Last VersionavilamarialuzNo ratings yet
- Mus189 Concert Comparison Assignment GuidelinesDocument3 pagesMus189 Concert Comparison Assignment Guidelinesapi-300390896No ratings yet
- 9 EeeDocument82 pages9 EeeRiya AgrawalNo ratings yet
- IIM Calcutta Recruitment Brochure 2015Document17 pagesIIM Calcutta Recruitment Brochure 2015Sankalp Akash SinghNo ratings yet
- Political OrganizationsDocument15 pagesPolitical Organizationsastherielle cameroNo ratings yet
- Implicit DifferentiationDocument12 pagesImplicit DifferentiationNaitsirc UluputipanNo ratings yet
- Intro To Human Computer InteractionDocument53 pagesIntro To Human Computer InteractionKanit WongsuphasasawatNo ratings yet
- Ethical Disintegration of Enron: PHI 401: Business EthicsDocument14 pagesEthical Disintegration of Enron: PHI 401: Business EthicsAnikaNo ratings yet
- 新概念英语第三册全部语法Document47 pages新概念英语第三册全部语法蔣偉宏No ratings yet
- RupDocument52 pagesRupmojtaba7No ratings yet
- 1 LogicDocument9 pages1 Logicakash vermaNo ratings yet
- Godel Escher Bach Ebook ItaDocument4 pagesGodel Escher Bach Ebook ItaJulie0% (1)
- Design Life vs. Seismic Return PeriodDocument19 pagesDesign Life vs. Seismic Return PeriodShivamMishraNo ratings yet
- APA Jamii Plus Family Medical Cover BrochureDocument8 pagesAPA Jamii Plus Family Medical Cover BrochureADANARABOW100% (1)
- Difference Between Precis WritingDocument2 pagesDifference Between Precis WritingNauman MashwaniNo ratings yet
- PVH EuropeDocument1 pagePVH Europeapi-237852926No ratings yet
- SdasasasDocument22 pagesSdasasasGianne Robert MalavegaNo ratings yet