Download as pdf or txt
You might also like
- GXT SeriesDocument8 pagesGXT SeriesCésar S. Silva100% (2)
- Acute and Suppurative AppendicitisDocument25 pagesAcute and Suppurative AppendicitisSheba Ibabao-Alayon Moradilla0% (1)
- Factors Affecting The Prevalence of Gastro-Oesophageal Reflux in Childhood Corrosive Oesophageal StricturesDocument6 pagesFactors Affecting The Prevalence of Gastro-Oesophageal Reflux in Childhood Corrosive Oesophageal StricturesAlinaRellyyNo ratings yet
- CT EnterographyDocument8 pagesCT EnterographyAbin VlNo ratings yet
- Accepted Manuscript: Clinical Gastroenterology and HepatologyDocument20 pagesAccepted Manuscript: Clinical Gastroenterology and HepatologyСергей СадовниковNo ratings yet
- AppendicitisDocument3 pagesAppendicitisRindayu Julianti NurmanNo ratings yet
- Case Discussion Patient ILOWADocument1 pageCase Discussion Patient ILOWARuvz CerdeñoNo ratings yet
- Pan 12581Document8 pagesPan 12581claudiaNo ratings yet
- Apendisitis MRM 3Document8 pagesApendisitis MRM 3siti solikhaNo ratings yet
- Fulltext 09 2008 1902-1909Document9 pagesFulltext 09 2008 1902-1909Cristina RyallNo ratings yet
- Prospective & Comparative Study of Various Techniques Used in The Management of Liver Abscess in The Bundelkhand AreaDocument10 pagesProspective & Comparative Study of Various Techniques Used in The Management of Liver Abscess in The Bundelkhand AreaIJAR JOURNALNo ratings yet
- Kunio Et Al. - 2015 - Short EsophagusDocument12 pagesKunio Et Al. - 2015 - Short EsophagusDaniel PredaNo ratings yet
- Liver A BSC DrainDocument8 pagesLiver A BSC DrainAngelica AmesquitaNo ratings yet
- Laplant 2018Document14 pagesLaplant 2018AndikaNo ratings yet
- Jurnal Bahasa Inggris Radiologi AapDocument11 pagesJurnal Bahasa Inggris Radiologi AapDessy leonni100% (1)
- Imaging Signs For Determining Surgery Timing of Acute Intestinal ObstructionDocument7 pagesImaging Signs For Determining Surgery Timing of Acute Intestinal ObstructionshaffaNo ratings yet
- Laparoscopy in The Acute AbdomenDocument15 pagesLaparoscopy in The Acute AbdomenDragoiu AlexandraNo ratings yet
- Historical Overview: Abstract: Several Studies Have Demonstrated That A Diagnosis Based SolelyDocument8 pagesHistorical Overview: Abstract: Several Studies Have Demonstrated That A Diagnosis Based SolelyLuh Tu PebriyantiNo ratings yet
- Role of Early Ultrasound in Detecting Inflammatory Intestinal Disorders and Identifying Their Anatomical Location Within The Bowel - 2003Document8 pagesRole of Early Ultrasound in Detecting Inflammatory Intestinal Disorders and Identifying Their Anatomical Location Within The Bowel - 2003Сергей СадовниковNo ratings yet
- WES GuidelineDocument28 pagesWES Guidelinesolo surgical forumNo ratings yet
- IMU Learning Outcome: Psychomotor SkillsDocument11 pagesIMU Learning Outcome: Psychomotor SkillsRameshNo ratings yet
- 2022 - Clinical Value of Abdominal USG in The Diagnosis of Acute Abdomen in ChildrenDocument7 pages2022 - Clinical Value of Abdominal USG in The Diagnosis of Acute Abdomen in ChildrenRevivo RindaNo ratings yet
- (2020) Colonography Evaluation of The Relationship Between Colon Anatomy and DiverticulaDocument7 pages(2020) Colonography Evaluation of The Relationship Between Colon Anatomy and DiverticulaChristian ToalongoNo ratings yet
- @medicinejournal European Journal of Pediatric Surgery January 2020Document126 pages@medicinejournal European Journal of Pediatric Surgery January 2020Ricardo Uzcategui ArreguiNo ratings yet
- A Systematic Review of Dose-Volume Predictors and Constraints For Late Bowel Toxicity Following Pelvic RadiotherapyDocument14 pagesA Systematic Review of Dose-Volume Predictors and Constraints For Late Bowel Toxicity Following Pelvic RadiotherapyAlfian AfriansyahNo ratings yet
- Comparative Evaluation of Ultrasonography and Computed Tomography in Pancreatic LesionsDocument13 pagesComparative Evaluation of Ultrasonography and Computed Tomography in Pancreatic LesionsMultan SohanhalwaNo ratings yet
- Milk As Oral Contrast in Abdomen CTDocument9 pagesMilk As Oral Contrast in Abdomen CTClever BarbieNo ratings yet
- Narcotic Analgesia in AppendicitisDocument2 pagesNarcotic Analgesia in AppendicitisAdil KhurshidNo ratings yet
- Evidencia 1Document6 pagesEvidencia 1Ricardo Uzcategui ArreguiNo ratings yet
- Final Draft6 Group1Document13 pagesFinal Draft6 Group1api-598481829No ratings yet
- Final Draft6 Group1Document13 pagesFinal Draft6 Group1api-598481829No ratings yet
- Intestinal Ultrasound Detects An Increased Diameter and Submucosal Layer Thickness in The Appendix of Patients With Ulcerative Colitis Compared To Healthy Controls - A Prospective Cohort StudyDocument9 pagesIntestinal Ultrasound Detects An Increased Diameter and Submucosal Layer Thickness in The Appendix of Patients With Ulcerative Colitis Compared To Healthy Controls - A Prospective Cohort StudyСергей СадовниковNo ratings yet
- Feasibility of Simple Oral Preparation Contrast-Enhanced CT Colonography (SOP-CE-CTC) Using Mannitol As A Neutral Oral Contrast AgentDocument9 pagesFeasibility of Simple Oral Preparation Contrast-Enhanced CT Colonography (SOP-CE-CTC) Using Mannitol As A Neutral Oral Contrast AgenttitelcosminelNo ratings yet
- Revista Mexico GastroenterologiaDocument6 pagesRevista Mexico GastroenterologiaRafael CamachoNo ratings yet
- 0100 3984 RB 51 06 0VII PDFDocument2 pages0100 3984 RB 51 06 0VII PDFMarcelitaTaliaDuwiriNo ratings yet
- FitulotomyDocument5 pagesFitulotomyDenis StoicaNo ratings yet
- болезнь КронаDocument7 pagesболезнь КронаAlexander NatroshviliNo ratings yet
- Intestinal Ultrasound in InflammatoryDocument17 pagesIntestinal Ultrasound in InflammatoryСергей СадовниковNo ratings yet
- Nonneoplastic Diseases of The Small Intestine: Differential Diagnosis and Crohn DiseaseDocument9 pagesNonneoplastic Diseases of The Small Intestine: Differential Diagnosis and Crohn DiseaseWhy DharmawanNo ratings yet
- Colonic Atresia Revision 1Document10 pagesColonic Atresia Revision 1HenggarAPNo ratings yet
- A Study of Preoperative Predictive Factors of Strangulation in Acute Small Intestinal ObstructionDocument6 pagesA Study of Preoperative Predictive Factors of Strangulation in Acute Small Intestinal ObstructionSantosh BabuNo ratings yet
- The Role of Imaging in Inflammatory Bowel Disease EvaluationDocument15 pagesThe Role of Imaging in Inflammatory Bowel Disease Evaluationafudaru6043No ratings yet
- Administration of Mucolytic Solution Before Upper Endoscopy - Double-Blind, Monocentric, Randomized StudyDocument5 pagesAdministration of Mucolytic Solution Before Upper Endoscopy - Double-Blind, Monocentric, Randomized StudyginaNo ratings yet
- Cavallini 2010Document8 pagesCavallini 2010Israel BlancoNo ratings yet
- Cutaneous Needle Aspirations in Liver DiseaseDocument6 pagesCutaneous Needle Aspirations in Liver DiseaseRhian BrimbleNo ratings yet
- Versus: Laparoscopic Open Appendectomy: Which Way To Go?Document6 pagesVersus: Laparoscopic Open Appendectomy: Which Way To Go?Claudiu Ungureanu ClauNo ratings yet
- Joevence - Journal ArticleDocument15 pagesJoevence - Journal ArticleJoevence CuaresmaNo ratings yet
- Article ApendicitisDocument7 pagesArticle ApendicitisXerexNo ratings yet
- Sonography and The Acute AbdomenDocument8 pagesSonography and The Acute AbdomenAlexander NatroshviliNo ratings yet
- Ce 48 291Document6 pagesCe 48 291Siska HarapanNo ratings yet
- Eliminación Ayunas Precontraste IVDocument61 pagesEliminación Ayunas Precontraste IVcpastorsNo ratings yet
- Usg Gastritis PDFDocument6 pagesUsg Gastritis PDFtambamanuellaNo ratings yet
- Sellick ManeuverDocument5 pagesSellick ManeuverJulianda EpriantiNo ratings yet
- Effects of Tracheostomy Tube On SwallowingDocument21 pagesEffects of Tracheostomy Tube On SwallowingPaola A. MartinezNo ratings yet
- Flank PainDocument4 pagesFlank PainErlin IrawatiNo ratings yet
- Stricture EsofagealDocument11 pagesStricture EsofagealInes Camilla PutriNo ratings yet
- Pryor 2015Document7 pagesPryor 2015cinthya zambranoNo ratings yet
- Delays in Imaging Diagnosis of Acute Abdominal PainDocument7 pagesDelays in Imaging Diagnosis of Acute Abdominal PainWillie VanegasNo ratings yet
- Atlas of Laparoscopic Gastrectomy for Gastric Cancer: High Resolution Image for New Surgical TechniqueFrom EverandAtlas of Laparoscopic Gastrectomy for Gastric Cancer: High Resolution Image for New Surgical TechniqueNo ratings yet
- Esophageal Preservation and Replacement in ChildrenFrom EverandEsophageal Preservation and Replacement in ChildrenAshwin PimpalwarNo ratings yet
- Trauma CERVICAL-Radiol Clin N.A.2012Document14 pagesTrauma CERVICAL-Radiol Clin N.A.2012Pepe pepe pepeNo ratings yet
- Trauma AORTICO-Radiol Clin N.A.2012Document19 pagesTrauma AORTICO-Radiol Clin N.A.2012Pepe pepe pepeNo ratings yet
- An Evidence Based Blunt Trauma ProtocolDocument7 pagesAn Evidence Based Blunt Trauma ProtocolPepe pepe pepeNo ratings yet
- 2015 - Improving Outcomes PolitraumaDocument18 pages2015 - Improving Outcomes PolitraumaPepe pepe pepeNo ratings yet
- Valentini 2016Document7 pagesValentini 2016Pepe pepe pepeNo ratings yet
- Radiographics 10 6 2259761Document25 pagesRadiographics 10 6 2259761Pepe pepe pepeNo ratings yet
- Ajr 10 5540Document9 pagesAjr 10 5540Pepe pepe pepeNo ratings yet
- Radiographics.22.suppl 1.g02oc16s231Document16 pagesRadiographics.22.suppl 1.g02oc16s231Pepe pepe pepeNo ratings yet
- BWB BrochureDocument5 pagesBWB BrochureUswatul HasanahNo ratings yet
- TheDocument12 pagesTheVictor PileggiNo ratings yet
- Asus T12C (X51C) Motherboard Schematic DiagramDocument94 pagesAsus T12C (X51C) Motherboard Schematic DiagramYblis100% (1)
- Hus3-C M8 Bolt For Brick WallDocument22 pagesHus3-C M8 Bolt For Brick WallANGEL MUÑOZNo ratings yet
- Fil-Chin Engineering: To: Limketkai Attn: Mr. Eduard Oh Re: Heat ExchangerDocument6 pagesFil-Chin Engineering: To: Limketkai Attn: Mr. Eduard Oh Re: Heat ExchangerKeith Henrich M. ChuaNo ratings yet
- Park Tool - Torque Specifications and ConceptsDocument9 pagesPark Tool - Torque Specifications and ConceptszuberNo ratings yet
- SAMPLE of Moon Time by Lucy H. Pearce, Womancraft PublishingDocument33 pagesSAMPLE of Moon Time by Lucy H. Pearce, Womancraft PublishingWomancraft PublishingNo ratings yet
- Metasploit FrameworkDocument1 pageMetasploit FrameworkPAUL VINCENT FAJARDONo ratings yet
- 1.1 India and Its Rich Culture: Socio-Cultural CentreDocument102 pages1.1 India and Its Rich Culture: Socio-Cultural CentrePrarthana GhoshNo ratings yet
- BusDocument24 pagesBusSyed Noman AhmedNo ratings yet
- Urinary SystemDocument9 pagesUrinary SystemMary Joyce RamosNo ratings yet
- Controllers and Controller StationsDocument65 pagesControllers and Controller StationsLucian ChorusNo ratings yet
- Our Own English High School, Sharjah Look Who'S Answering Quiz Club Group I (Grade 1) Question Bank - MAY 2019Document3 pagesOur Own English High School, Sharjah Look Who'S Answering Quiz Club Group I (Grade 1) Question Bank - MAY 2019Abimanyu ShenilNo ratings yet
- P2 Chp2 Section 2.1ADocument3 pagesP2 Chp2 Section 2.1APaing Khant KyawNo ratings yet
- EN ISO 13503-2 (2006) (E) CodifiedDocument8 pagesEN ISO 13503-2 (2006) (E) CodifiedEzgi PelitNo ratings yet
- TechNote CableModellingDocument12 pagesTechNote CableModellingLeonardo LeonNo ratings yet
- Wee1964 N001Document9 pagesWee1964 N001Oliver RubioNo ratings yet
- ARTS7 Q3 Week6Document7 pagesARTS7 Q3 Week6Samantha Nicole CarlotoNo ratings yet
- Worksheet - Orbital Diagrams - TeacherDocument2 pagesWorksheet - Orbital Diagrams - Teacherdela2100% (3)
- Three Dimensional GeometryDocument3 pagesThree Dimensional GeometryTaqi IsmailNo ratings yet
- c1Document7 pagesc1Ingrid Garcia de JaureguiNo ratings yet
- Quinone-Based Molecular Electrochemistry and Their Contributions To Medicinal Chemistry: A Look at The Present and FutureDocument9 pagesQuinone-Based Molecular Electrochemistry and Their Contributions To Medicinal Chemistry: A Look at The Present and FutureSanti Osorio DiezNo ratings yet
- ASTM D1654 Standard Test Method For Evaluation of Painted or Coated Specimens Subjected To Corrosive EnvironmentsDocument4 pagesASTM D1654 Standard Test Method For Evaluation of Painted or Coated Specimens Subjected To Corrosive EnvironmentsDavid VegaNo ratings yet
- Modding For Ysflight - Scenery EditorDocument92 pagesModding For Ysflight - Scenery Editordecaff_42No ratings yet
- Logicalreasoning MockDocument11 pagesLogicalreasoning MockTarun GaurNo ratings yet
- STT Lincoln Electric PDFDocument30 pagesSTT Lincoln Electric PDFbkprodhNo ratings yet
- Direction TestDocument3 pagesDirection TestprascribdNo ratings yet
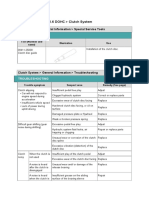
- 06.clutch SystemDocument24 pages06.clutch SystemTony D'AngeloNo ratings yet
- Lynx SpecificationsDocument2 pagesLynx Specificationsengine wangNo ratings yet