
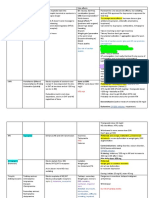
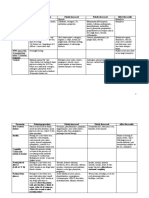
Antidepressants: Classification
Antidepressants: Classification
You might also like
- Antidepressant ChartDocument7 pagesAntidepressant Chartinher1tance100% (4)
- Study Checklist For Passing NCLEX-RN - AllnursesDocument2 pagesStudy Checklist For Passing NCLEX-RN - Allnursesbeingfired100% (1)
- CHT Psyc AntidepressantDocument3 pagesCHT Psyc AntidepressantRicardo Lugon ArantesNo ratings yet
- AntipsychoticsDocument4 pagesAntipsychoticsbala indurthiNo ratings yet
- A. Stahl - STAHL's, Essential PharmacologyDocument53 pagesA. Stahl - STAHL's, Essential PharmacologyDaniel De los SantosNo ratings yet
- Antidepressant Use in Adults With Chronic Kidney DiseaseDocument1 pageAntidepressant Use in Adults With Chronic Kidney DiseaseAzhar Ali100% (1)
- Dipiro 9 (268-286) KontrasepsiDocument5 pagesDipiro 9 (268-286) KontrasepsiNingrumSindayaniNo ratings yet
- PK's Antidepressant Notes (Pharm)Document9 pagesPK's Antidepressant Notes (Pharm)pattykNo ratings yet
- Hiv Current Trend in The Use of HaartDocument19 pagesHiv Current Trend in The Use of Haartapi-3705046No ratings yet
- Antidepressant DrugsDocument19 pagesAntidepressant DrugsUMESH KANDELNo ratings yet
- NH Protocol For Covid Management FinalDocument7 pagesNH Protocol For Covid Management FinalhoneyworksNo ratings yet
- PharmaDocument1 pagePharmaPrinceNo ratings yet
- Alcohol Withdrawal PathwayDocument1 pageAlcohol Withdrawal Pathwaymguo123No ratings yet
- Medication Worksheet: Citrus College Associate Degree NursingDocument5 pagesMedication Worksheet: Citrus College Associate Degree NursingRhonnie De GuzmanNo ratings yet
- ArthritisDocument69 pagesArthritisKavya sriNo ratings yet
- Drug StudyDocument2 pagesDrug StudyGrace CadawasNo ratings yet
- N335 RM 13A: C Ceftriaxone SodiumDocument2 pagesN335 RM 13A: C Ceftriaxone SodiumsukebebeNo ratings yet
- Anxiety Disorders - TreatmentDocument16 pagesAnxiety Disorders - TreatmentFAMED RESIDENTS CESMEDNo ratings yet
- LevetiracetamDocument3 pagesLevetiracetamGwyn Rosales100% (2)
- Table: Aed Summary: Older AedsDocument3 pagesTable: Aed Summary: Older AedsAmit PatelNo ratings yet
- AntiepilepticiDocument29 pagesAntiepilepticiIskraNo ratings yet
- Pharmacology Chart 3Document2 pagesPharmacology Chart 3Omar ClorNo ratings yet
- Min Lect PK - 1Document3 pagesMin Lect PK - 1fandi_cah_ganteng3367No ratings yet
- Drug StudyDocument3 pagesDrug StudySoniaMarieBalanayNo ratings yet
- Nuvastatic Practitioner Only Information 12.5.20Document8 pagesNuvastatic Practitioner Only Information 12.5.20Jamall EllisNo ratings yet
- Birth Control Made Simple 2010Document5 pagesBirth Control Made Simple 2010Richard WahlNo ratings yet
- 1: Adhd: Scientific Name Dose CommentsDocument4 pages1: Adhd: Scientific Name Dose CommentsSadiq Abdo92No ratings yet
- Antiseizure Agents & EffectsDocument23 pagesAntiseizure Agents & EffectsPrakash GontiNo ratings yet
- Neurobiology of Aggression and Violence: Systems, Intervention, and ImpactDocument34 pagesNeurobiology of Aggression and Violence: Systems, Intervention, and ImpactMsc CBDCNo ratings yet
- Did Seizures QN 1Document31 pagesDid Seizures QN 1api-608647584No ratings yet
- Israel PantojaDocument26 pagesIsrael PantojaJuan FernandoNo ratings yet
- Drug StudyDocument4 pagesDrug StudyDean Angelo BarrientosNo ratings yet
- Drugs Used For Hyperthyroidism - Sunga, Saara Paula BiancaDocument6 pagesDrugs Used For Hyperthyroidism - Sunga, Saara Paula BiancaBea SungaNo ratings yet
- F4) P-Rheumatoid ArthritisDocument11 pagesF4) P-Rheumatoid Arthritisstella.gillesania.chenNo ratings yet
- Anti-Depressant Drugs: Presented by L.Nithish Shankar Ii Year Mbbs KGMCDocument17 pagesAnti-Depressant Drugs: Presented by L.Nithish Shankar Ii Year Mbbs KGMCÑiťhišh Śhankąŕ LóganáthánNo ratings yet
- Type of Pain Examples MechanismsDocument3 pagesType of Pain Examples MechanismsStella ApaNo ratings yet
- Pallia Note1Document3 pagesPallia Note1Stella ApaNo ratings yet
- 1) Selective Serotonin Reuptic Inhepetor (SSRI) - Xetine: Fluoxetine, Paroxetine, Sertraline, DoluexitineDocument13 pages1) Selective Serotonin Reuptic Inhepetor (SSRI) - Xetine: Fluoxetine, Paroxetine, Sertraline, DoluexitineSEIYADU IBRAHIM KNo ratings yet
- Dopamine HypothesisDocument2 pagesDopamine HypothesisBo123456100% (3)
- Therapeutic Drug Monitoring in Adults at NUH2011 FinalDocument2 pagesTherapeutic Drug Monitoring in Adults at NUH2011 FinalStacey WoodsNo ratings yet
- Oncology Cheat Sheets - 1Document5 pagesOncology Cheat Sheets - 1abdallahmaurice94No ratings yet
- Drug-Drug: DecreasedDocument10 pagesDrug-Drug: DecreasedMelodia Turqueza GandezaNo ratings yet
- Week 7Document4 pagesWeek 7Joanna BakNo ratings yet
- Product List: by Daehan New Pharm Co., LTDDocument9 pagesProduct List: by Daehan New Pharm Co., LTDasgar meilindaNo ratings yet
- UntitledDocument42 pagesUntitledVivek KumarNo ratings yet
- Classification of InfectiousDocument3 pagesClassification of InfectiousabubakarNo ratings yet
- ANTIDEPRESAN RevisiDocument46 pagesANTIDEPRESAN RevisiRereNo ratings yet
- "Antiepileptic Drugs": Clinical Chemistry 3Document2 pages"Antiepileptic Drugs": Clinical Chemistry 3Maam ShaNo ratings yet
- BPH and EdDocument1 pageBPH and EdWAN SUMAIYAH BINTI WAN HUSINNo ratings yet
- Pharmacotherapy of Epilepsy: Nandit P BDocument53 pagesPharmacotherapy of Epilepsy: Nandit P BNandit BanawalikarNo ratings yet
- 3.2 Medication Histories of Ascities: Table 3.2aDocument9 pages3.2 Medication Histories of Ascities: Table 3.2ab_rahman2k39603No ratings yet
- Long Term Pharmacotherapy For Alcohol Dependence: Centre of Addiction Medicine NIMHANS, BangaloreDocument55 pagesLong Term Pharmacotherapy For Alcohol Dependence: Centre of Addiction Medicine NIMHANS, BangaloreGirish NagarNo ratings yet
- Management of Extravasation of Antineoplastic Agents: Maryna RubachDocument8 pagesManagement of Extravasation of Antineoplastic Agents: Maryna RubachBedah UnhasNo ratings yet
- DrugDocument10 pagesDrugMelodia Turqueza GandezaNo ratings yet
- Drug-Drug: DecreasedDocument10 pagesDrug-Drug: DecreasedMelodia Turqueza GandezaNo ratings yet
- Epilepsy Is Due To Sudden, Excessive Depolarization Of: Some or All Cerebral NeuronsDocument19 pagesEpilepsy Is Due To Sudden, Excessive Depolarization Of: Some or All Cerebral NeuronsMourian AmanNo ratings yet
- Cerenia InjectableDocument2 pagesCerenia InjectableRue BensonNo ratings yet
- Sympathomimetics: Noradrenaline Adrenaline Dopamine Isoprenaline DobutamineDocument4 pagesSympathomimetics: Noradrenaline Adrenaline Dopamine Isoprenaline DobutamineTomNo ratings yet
- Drug Study PDFDocument7 pagesDrug Study PDFMarissa AsimNo ratings yet
- Clinical Enquiry Comment/Case ManagementDocument7 pagesClinical Enquiry Comment/Case ManagementIzzah AhsanNo ratings yet
- Yoga and Pranayama During High-Risk PregnancyDocument7 pagesYoga and Pranayama During High-Risk PregnancyAdvanced Research PublicationsNo ratings yet
- GlaucomaDocument3 pagesGlaucomaAgustinus BethaNo ratings yet
- Hypertension: Alemwosen T. (MD, Asst Prof in Pathology)Document46 pagesHypertension: Alemwosen T. (MD, Asst Prof in Pathology)Amanuel MaruNo ratings yet
- WORKSHEET For Unit 14 On PEDIATRIC MUSCULOSKELETAL DISORDERSDocument14 pagesWORKSHEET For Unit 14 On PEDIATRIC MUSCULOSKELETAL DISORDERScorisNo ratings yet
- 8 TCCC Scenarios IgDocument35 pages8 TCCC Scenarios Igherbert rogan0% (1)
- AO2020-0043 Guidelines On Ensuring The Affordability of Essential Medicines in DOH Facilities Through The Regulation of Price Mark-Ups (09-11)Document11 pagesAO2020-0043 Guidelines On Ensuring The Affordability of Essential Medicines in DOH Facilities Through The Regulation of Price Mark-Ups (09-11)Leah Rose Figueroa ParasNo ratings yet
- Disease: Renal (Dialysis) : Martínez Montes de Oca Jessica. Reyes Del Angel NaimeDocument6 pagesDisease: Renal (Dialysis) : Martínez Montes de Oca Jessica. Reyes Del Angel NaimeOmar De LeonNo ratings yet
- Rubi Li Vs Soliman, GR No. 165279Document1 pageRubi Li Vs Soliman, GR No. 165279El G. Se Cheng100% (1)
- Postnatal ExcerciseDocument9 pagesPostnatal ExcercisePadma75% (4)
- Iwj 15 971Document7 pagesIwj 15 971Francisco Castillo VázquezNo ratings yet
- Pe 4 Week 5 and 6 Module q4Document7 pagesPe 4 Week 5 and 6 Module q4Stephanie TamayuzaNo ratings yet
- The Importance of Risk Factors in The Etiology of Arterial HypertensionDocument4 pagesThe Importance of Risk Factors in The Etiology of Arterial HypertensionAcademic JournalNo ratings yet
- Glory of Christ Church Medical Mission ProposalDocument13 pagesGlory of Christ Church Medical Mission Proposalschaf ugandaNo ratings yet
- 2 Bipolar DisorderDocument9 pages2 Bipolar DisorderJuan Carlos Veloso RetamalNo ratings yet
- Managing A Patient With Open-Angle Glaucoma: A Case StudyDocument3 pagesManaging A Patient With Open-Angle Glaucoma: A Case StudyDimpi DeviNo ratings yet
- Alteration in Immune ResponseDocument29 pagesAlteration in Immune ResponsePachita AlexandruNo ratings yet
- Hinoguin, Jocelyn Patana 1851114785Document3 pagesHinoguin, Jocelyn Patana 1851114785Paulline Joyce HinoguinNo ratings yet
- Final Synopsis PHDDocument13 pagesFinal Synopsis PHDKishor KanaseNo ratings yet
- Radiographic Aids in The Diagnosis of Periodontal Diseases: Presented By: DR: Abdullah AliDocument27 pagesRadiographic Aids in The Diagnosis of Periodontal Diseases: Presented By: DR: Abdullah AliMugahed Abdo Al-gahdariNo ratings yet
- 3.9. Angiotensins''Document44 pages3.9. Angiotensins''Garry LasagaNo ratings yet
- Colorectal Cancer: What Is Colorectal Carcinoma?Document4 pagesColorectal Cancer: What Is Colorectal Carcinoma?Ryana Fitriana IINo ratings yet
- Icd 10 MataDocument3 pagesIcd 10 MataApakau WehNo ratings yet
- LiverCirr 2011Document303 pagesLiverCirr 2011EnderNo ratings yet
- Contact Dermatitis ModuleDocument68 pagesContact Dermatitis Moduletimvrghs123No ratings yet
- 1 - FMGE Dec GH VersionDocument14 pages1 - FMGE Dec GH VersionHarshit SharmaNo ratings yet
- Health India TPA - Pre Auth FormDocument5 pagesHealth India TPA - Pre Auth FormBOOKREADER_NOW100% (1)
- Sciatic AdviceDocument3 pagesSciatic AdviceJohn Fightakis100% (2)
- PG 577Document2 pagesPG 577Michu VuNo ratings yet
- Patient Assistance Reimbursement Guide 2019Document93 pagesPatient Assistance Reimbursement Guide 2019Matthias Lee-Hifler100% (1)




















































































Download as pdf or txt
You might also like
- Antidepressant ChartDocument7 pagesAntidepressant Chartinher1tance100% (4)
- Study Checklist For Passing NCLEX-RN - AllnursesDocument2 pagesStudy Checklist For Passing NCLEX-RN - Allnursesbeingfired100% (1)
- CHT Psyc AntidepressantDocument3 pagesCHT Psyc AntidepressantRicardo Lugon ArantesNo ratings yet
- AntipsychoticsDocument4 pagesAntipsychoticsbala indurthiNo ratings yet
- A. Stahl - STAHL's, Essential PharmacologyDocument53 pagesA. Stahl - STAHL's, Essential PharmacologyDaniel De los SantosNo ratings yet
- Antidepressant Use in Adults With Chronic Kidney DiseaseDocument1 pageAntidepressant Use in Adults With Chronic Kidney DiseaseAzhar Ali100% (1)
- Dipiro 9 (268-286) KontrasepsiDocument5 pagesDipiro 9 (268-286) KontrasepsiNingrumSindayaniNo ratings yet
- PK's Antidepressant Notes (Pharm)Document9 pagesPK's Antidepressant Notes (Pharm)pattykNo ratings yet
- Hiv Current Trend in The Use of HaartDocument19 pagesHiv Current Trend in The Use of Haartapi-3705046No ratings yet
- Antidepressant DrugsDocument19 pagesAntidepressant DrugsUMESH KANDELNo ratings yet
- NH Protocol For Covid Management FinalDocument7 pagesNH Protocol For Covid Management FinalhoneyworksNo ratings yet
- PharmaDocument1 pagePharmaPrinceNo ratings yet
- Alcohol Withdrawal PathwayDocument1 pageAlcohol Withdrawal Pathwaymguo123No ratings yet
- Medication Worksheet: Citrus College Associate Degree NursingDocument5 pagesMedication Worksheet: Citrus College Associate Degree NursingRhonnie De GuzmanNo ratings yet
- ArthritisDocument69 pagesArthritisKavya sriNo ratings yet
- Drug StudyDocument2 pagesDrug StudyGrace CadawasNo ratings yet
- N335 RM 13A: C Ceftriaxone SodiumDocument2 pagesN335 RM 13A: C Ceftriaxone SodiumsukebebeNo ratings yet
- Anxiety Disorders - TreatmentDocument16 pagesAnxiety Disorders - TreatmentFAMED RESIDENTS CESMEDNo ratings yet
- LevetiracetamDocument3 pagesLevetiracetamGwyn Rosales100% (2)
- Table: Aed Summary: Older AedsDocument3 pagesTable: Aed Summary: Older AedsAmit PatelNo ratings yet
- AntiepilepticiDocument29 pagesAntiepilepticiIskraNo ratings yet
- Pharmacology Chart 3Document2 pagesPharmacology Chart 3Omar ClorNo ratings yet
- Min Lect PK - 1Document3 pagesMin Lect PK - 1fandi_cah_ganteng3367No ratings yet
- Drug StudyDocument3 pagesDrug StudySoniaMarieBalanayNo ratings yet
- Nuvastatic Practitioner Only Information 12.5.20Document8 pagesNuvastatic Practitioner Only Information 12.5.20Jamall EllisNo ratings yet
- Birth Control Made Simple 2010Document5 pagesBirth Control Made Simple 2010Richard WahlNo ratings yet
- 1: Adhd: Scientific Name Dose CommentsDocument4 pages1: Adhd: Scientific Name Dose CommentsSadiq Abdo92No ratings yet
- Antiseizure Agents & EffectsDocument23 pagesAntiseizure Agents & EffectsPrakash GontiNo ratings yet
- Neurobiology of Aggression and Violence: Systems, Intervention, and ImpactDocument34 pagesNeurobiology of Aggression and Violence: Systems, Intervention, and ImpactMsc CBDCNo ratings yet
- Did Seizures QN 1Document31 pagesDid Seizures QN 1api-608647584No ratings yet
- Israel PantojaDocument26 pagesIsrael PantojaJuan FernandoNo ratings yet
- Drug StudyDocument4 pagesDrug StudyDean Angelo BarrientosNo ratings yet
- Drugs Used For Hyperthyroidism - Sunga, Saara Paula BiancaDocument6 pagesDrugs Used For Hyperthyroidism - Sunga, Saara Paula BiancaBea SungaNo ratings yet
- F4) P-Rheumatoid ArthritisDocument11 pagesF4) P-Rheumatoid Arthritisstella.gillesania.chenNo ratings yet
- Anti-Depressant Drugs: Presented by L.Nithish Shankar Ii Year Mbbs KGMCDocument17 pagesAnti-Depressant Drugs: Presented by L.Nithish Shankar Ii Year Mbbs KGMCÑiťhišh Śhankąŕ LóganáthánNo ratings yet
- Type of Pain Examples MechanismsDocument3 pagesType of Pain Examples MechanismsStella ApaNo ratings yet
- Pallia Note1Document3 pagesPallia Note1Stella ApaNo ratings yet
- 1) Selective Serotonin Reuptic Inhepetor (SSRI) - Xetine: Fluoxetine, Paroxetine, Sertraline, DoluexitineDocument13 pages1) Selective Serotonin Reuptic Inhepetor (SSRI) - Xetine: Fluoxetine, Paroxetine, Sertraline, DoluexitineSEIYADU IBRAHIM KNo ratings yet
- Dopamine HypothesisDocument2 pagesDopamine HypothesisBo123456100% (3)
- Therapeutic Drug Monitoring in Adults at NUH2011 FinalDocument2 pagesTherapeutic Drug Monitoring in Adults at NUH2011 FinalStacey WoodsNo ratings yet
- Oncology Cheat Sheets - 1Document5 pagesOncology Cheat Sheets - 1abdallahmaurice94No ratings yet
- Drug-Drug: DecreasedDocument10 pagesDrug-Drug: DecreasedMelodia Turqueza GandezaNo ratings yet
- Week 7Document4 pagesWeek 7Joanna BakNo ratings yet
- Product List: by Daehan New Pharm Co., LTDDocument9 pagesProduct List: by Daehan New Pharm Co., LTDasgar meilindaNo ratings yet
- UntitledDocument42 pagesUntitledVivek KumarNo ratings yet
- Classification of InfectiousDocument3 pagesClassification of InfectiousabubakarNo ratings yet
- ANTIDEPRESAN RevisiDocument46 pagesANTIDEPRESAN RevisiRereNo ratings yet
- "Antiepileptic Drugs": Clinical Chemistry 3Document2 pages"Antiepileptic Drugs": Clinical Chemistry 3Maam ShaNo ratings yet
- BPH and EdDocument1 pageBPH and EdWAN SUMAIYAH BINTI WAN HUSINNo ratings yet
- Pharmacotherapy of Epilepsy: Nandit P BDocument53 pagesPharmacotherapy of Epilepsy: Nandit P BNandit BanawalikarNo ratings yet
- 3.2 Medication Histories of Ascities: Table 3.2aDocument9 pages3.2 Medication Histories of Ascities: Table 3.2ab_rahman2k39603No ratings yet
- Long Term Pharmacotherapy For Alcohol Dependence: Centre of Addiction Medicine NIMHANS, BangaloreDocument55 pagesLong Term Pharmacotherapy For Alcohol Dependence: Centre of Addiction Medicine NIMHANS, BangaloreGirish NagarNo ratings yet
- Management of Extravasation of Antineoplastic Agents: Maryna RubachDocument8 pagesManagement of Extravasation of Antineoplastic Agents: Maryna RubachBedah UnhasNo ratings yet
- DrugDocument10 pagesDrugMelodia Turqueza GandezaNo ratings yet
- Drug-Drug: DecreasedDocument10 pagesDrug-Drug: DecreasedMelodia Turqueza GandezaNo ratings yet
- Epilepsy Is Due To Sudden, Excessive Depolarization Of: Some or All Cerebral NeuronsDocument19 pagesEpilepsy Is Due To Sudden, Excessive Depolarization Of: Some or All Cerebral NeuronsMourian AmanNo ratings yet
- Cerenia InjectableDocument2 pagesCerenia InjectableRue BensonNo ratings yet
- Sympathomimetics: Noradrenaline Adrenaline Dopamine Isoprenaline DobutamineDocument4 pagesSympathomimetics: Noradrenaline Adrenaline Dopamine Isoprenaline DobutamineTomNo ratings yet
- Drug Study PDFDocument7 pagesDrug Study PDFMarissa AsimNo ratings yet
- Clinical Enquiry Comment/Case ManagementDocument7 pagesClinical Enquiry Comment/Case ManagementIzzah AhsanNo ratings yet
- Yoga and Pranayama During High-Risk PregnancyDocument7 pagesYoga and Pranayama During High-Risk PregnancyAdvanced Research PublicationsNo ratings yet
- GlaucomaDocument3 pagesGlaucomaAgustinus BethaNo ratings yet
- Hypertension: Alemwosen T. (MD, Asst Prof in Pathology)Document46 pagesHypertension: Alemwosen T. (MD, Asst Prof in Pathology)Amanuel MaruNo ratings yet
- WORKSHEET For Unit 14 On PEDIATRIC MUSCULOSKELETAL DISORDERSDocument14 pagesWORKSHEET For Unit 14 On PEDIATRIC MUSCULOSKELETAL DISORDERScorisNo ratings yet
- 8 TCCC Scenarios IgDocument35 pages8 TCCC Scenarios Igherbert rogan0% (1)
- AO2020-0043 Guidelines On Ensuring The Affordability of Essential Medicines in DOH Facilities Through The Regulation of Price Mark-Ups (09-11)Document11 pagesAO2020-0043 Guidelines On Ensuring The Affordability of Essential Medicines in DOH Facilities Through The Regulation of Price Mark-Ups (09-11)Leah Rose Figueroa ParasNo ratings yet
- Disease: Renal (Dialysis) : Martínez Montes de Oca Jessica. Reyes Del Angel NaimeDocument6 pagesDisease: Renal (Dialysis) : Martínez Montes de Oca Jessica. Reyes Del Angel NaimeOmar De LeonNo ratings yet
- Rubi Li Vs Soliman, GR No. 165279Document1 pageRubi Li Vs Soliman, GR No. 165279El G. Se Cheng100% (1)
- Postnatal ExcerciseDocument9 pagesPostnatal ExcercisePadma75% (4)
- Iwj 15 971Document7 pagesIwj 15 971Francisco Castillo VázquezNo ratings yet
- Pe 4 Week 5 and 6 Module q4Document7 pagesPe 4 Week 5 and 6 Module q4Stephanie TamayuzaNo ratings yet
- The Importance of Risk Factors in The Etiology of Arterial HypertensionDocument4 pagesThe Importance of Risk Factors in The Etiology of Arterial HypertensionAcademic JournalNo ratings yet
- Glory of Christ Church Medical Mission ProposalDocument13 pagesGlory of Christ Church Medical Mission Proposalschaf ugandaNo ratings yet
- 2 Bipolar DisorderDocument9 pages2 Bipolar DisorderJuan Carlos Veloso RetamalNo ratings yet
- Managing A Patient With Open-Angle Glaucoma: A Case StudyDocument3 pagesManaging A Patient With Open-Angle Glaucoma: A Case StudyDimpi DeviNo ratings yet
- Alteration in Immune ResponseDocument29 pagesAlteration in Immune ResponsePachita AlexandruNo ratings yet
- Hinoguin, Jocelyn Patana 1851114785Document3 pagesHinoguin, Jocelyn Patana 1851114785Paulline Joyce HinoguinNo ratings yet
- Final Synopsis PHDDocument13 pagesFinal Synopsis PHDKishor KanaseNo ratings yet
- Radiographic Aids in The Diagnosis of Periodontal Diseases: Presented By: DR: Abdullah AliDocument27 pagesRadiographic Aids in The Diagnosis of Periodontal Diseases: Presented By: DR: Abdullah AliMugahed Abdo Al-gahdariNo ratings yet
- 3.9. Angiotensins''Document44 pages3.9. Angiotensins''Garry LasagaNo ratings yet
- Colorectal Cancer: What Is Colorectal Carcinoma?Document4 pagesColorectal Cancer: What Is Colorectal Carcinoma?Ryana Fitriana IINo ratings yet
- Icd 10 MataDocument3 pagesIcd 10 MataApakau WehNo ratings yet
- LiverCirr 2011Document303 pagesLiverCirr 2011EnderNo ratings yet
- Contact Dermatitis ModuleDocument68 pagesContact Dermatitis Moduletimvrghs123No ratings yet
- 1 - FMGE Dec GH VersionDocument14 pages1 - FMGE Dec GH VersionHarshit SharmaNo ratings yet
- Health India TPA - Pre Auth FormDocument5 pagesHealth India TPA - Pre Auth FormBOOKREADER_NOW100% (1)
- Sciatic AdviceDocument3 pagesSciatic AdviceJohn Fightakis100% (2)
- PG 577Document2 pagesPG 577Michu VuNo ratings yet
- Patient Assistance Reimbursement Guide 2019Document93 pagesPatient Assistance Reimbursement Guide 2019Matthias Lee-Hifler100% (1)