Download as pdf or txt
You might also like
- UK Guidelines Iron Deficiency in Pregnancy PDFDocument34 pagesUK Guidelines Iron Deficiency in Pregnancy PDFYoga Rhamada SiregarNo ratings yet
- Joo Sten 2017Document7 pagesJoo Sten 2017langit rizki yuditamaNo ratings yet
- Diagnosis of Iron Deficiency and Iron Overload Nov 06Document8 pagesDiagnosis of Iron Deficiency and Iron Overload Nov 06Danielcc LeeNo ratings yet
- Iron Deficiency Without AnemiaDocument7 pagesIron Deficiency Without AnemiaLevente BalázsNo ratings yet
- Anemia Pathophysiology 1Document34 pagesAnemia Pathophysiology 1ScribdTranslationsNo ratings yet
- Elevated Ferritin What Should GP KnowDocument5 pagesElevated Ferritin What Should GP KnowDanielcc LeeNo ratings yet
- Sucrosomial Iron: A New Generation Iron For Improving Oral SupplementationDocument23 pagesSucrosomial Iron: A New Generation Iron For Improving Oral SupplementationЛеонид ГречишкоNo ratings yet
- Soluble Transferrin Receptor As A Diagnostic Laboratory Test For Detection of Iron Deficiency Anemia in Acute Illness of Hospitalized PatientsDocument3 pagesSoluble Transferrin Receptor As A Diagnostic Laboratory Test For Detection of Iron Deficiency Anemia in Acute Illness of Hospitalized PatientsAldila VidyaNo ratings yet
- Anemia HomeworkDocument3 pagesAnemia HomeworkShanon LimNo ratings yet
- ArticlesDocument6 pagesArticlesbedahfkumiNo ratings yet
- Iron Deficiency Anemia PathoDocument6 pagesIron Deficiency Anemia PathoENo ratings yet
- Iron Deficiency AnemiaDocument28 pagesIron Deficiency AnemiaKashan SiddiquiNo ratings yet
- Anemia of Chronic DiseaseDocument2 pagesAnemia of Chronic DiseasejuanabNo ratings yet
- RL-2 Anormalidades Serie Roja 1 Anemia of InflammationDocument11 pagesRL-2 Anormalidades Serie Roja 1 Anemia of InflammationEliNo ratings yet
- Iron DeficiencyDocument9 pagesIron DeficiencyJohn TorresNo ratings yet
- Jurding IDADocument14 pagesJurding IDAivo afianiNo ratings yet
- Approached in Diagnosis of AnemiaDocument41 pagesApproached in Diagnosis of AnemiaAlqodri SetiawanNo ratings yet
- Pharmacy Oncology Pharmacology OutlineDocument39 pagesPharmacy Oncology Pharmacology OutlineMatthew Lei100% (1)
- Hematology 2015 CamaschellaDocument6 pagesHematology 2015 CamaschellachameleonNo ratings yet
- Guidelines & Protocols: Advisory CommitteeDocument9 pagesGuidelines & Protocols: Advisory CommitteeeddcitoNo ratings yet
- Iron OverloadDocument9 pagesIron OverloadMentari Indah SariNo ratings yet
- Anemia Inflamación CrónicaDocument11 pagesAnemia Inflamación CrónicaCarlos MorenoNo ratings yet
- Give The Name of Different Forms of Anemia With TreatmentDocument6 pagesGive The Name of Different Forms of Anemia With TreatmentRaju DasNo ratings yet
- Iron Deficiency Anemia in Chronic Liver Disease: Etiopathogenesis, Diagnosis and TreatmentDocument9 pagesIron Deficiency Anemia in Chronic Liver Disease: Etiopathogenesis, Diagnosis and TreatmentOcha24 TupamahuNo ratings yet
- Amiodarone-Induced Hypothyroidism With EPO-resistant Anemia in A Patient With Chronic Renal FailureDocument3 pagesAmiodarone-Induced Hypothyroidism With EPO-resistant Anemia in A Patient With Chronic Renal Failureeki_megaraniNo ratings yet
- Diagnosis and Treatment of Iron Deficiency Anemia (IDA)Document7 pagesDiagnosis and Treatment of Iron Deficiency Anemia (IDA)Abdullah EssaNo ratings yet
- CAC Score PaperDocument3 pagesCAC Score PaperLeo AramburuNo ratings yet
- Transfusional Iron Overload and Chelation Therapy With Deferoxamine and Deferiprone (L1)Document13 pagesTransfusional Iron Overload and Chelation Therapy With Deferoxamine and Deferiprone (L1)anrihmNo ratings yet
- Anemia of InflammationDocument12 pagesAnemia of InflammationValentina Oviedo ValdesNo ratings yet
- Iron Deficiency AnemiaDocument12 pagesIron Deficiency AnemiaMargarita TorresNo ratings yet
- Iron Deficiency Anemia & ManagementDocument60 pagesIron Deficiency Anemia & Managementswap58war100% (1)
- Uk Guidelines Iron Deficiency in PregnancyDocument34 pagesUk Guidelines Iron Deficiency in PregnancyFirdaus AzinunNo ratings yet
- Intravenous Irons: From Basic Science To Clinical Practice: PharmaceuticalsDocument20 pagesIntravenous Irons: From Basic Science To Clinical Practice: Pharmaceuticalsisabel pangNo ratings yet
- Anemia Def Fe 2015Document20 pagesAnemia Def Fe 2015ChingHuaNo ratings yet
- A Short Study On Iron Deficiency in Hostels Using Data Collection FormDocument4 pagesA Short Study On Iron Deficiency in Hostels Using Data Collection FormInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Diagnosis of Case: 1. Blood LossDocument9 pagesDiagnosis of Case: 1. Blood LossGarrett SimpsonNo ratings yet
- Estacion, England Dan C. - AnemiasDocument17 pagesEstacion, England Dan C. - AnemiasEngland Dan EstacionNo ratings yet
- HHS Public Access: The Role of Iron Repletion in Adult Iron Deficiency Anemia and Other DiseasesDocument18 pagesHHS Public Access: The Role of Iron Repletion in Adult Iron Deficiency Anemia and Other DiseasesKingPasta88 premiereDesignVIDEONo ratings yet
- Anemia FerropenicaDocument8 pagesAnemia FerropenicaDiego AguilarNo ratings yet
- Management of Iron de Ficiency: Shuoyan Ning and Michelle P. ZellerDocument8 pagesManagement of Iron de Ficiency: Shuoyan Ning and Michelle P. ZellerGeorgina Aguilar GallardoNo ratings yet
- 857 1857 1 PBDocument4 pages857 1857 1 PBJesselle LasernaNo ratings yet
- Guidelines For The Management of Iron Deficiency AnaemiaDocument8 pagesGuidelines For The Management of Iron Deficiency AnaemiaAndrésGuarnizoNo ratings yet
- Ferritin Reference Range, Interpretation, Collection and PanelsDocument3 pagesFerritin Reference Range, Interpretation, Collection and Panelson miniNo ratings yet
- Investigating Microcytic AnemiaDocument7 pagesInvestigating Microcytic AnemiaBariša KiršnerNo ratings yet
- Management of Preoperative Anemia: Laura Mendez-Pino,, Andrés Zorrilla-Vaca,, David L. HepnerDocument9 pagesManagement of Preoperative Anemia: Laura Mendez-Pino,, Andrés Zorrilla-Vaca,, David L. HepneryenuginNo ratings yet
- Iron Deficiency Anaemia Armando HasudunganDocument1 pageIron Deficiency Anaemia Armando HasudunganhiNo ratings yet
- Disorders of Iron MetabolismDocument42 pagesDisorders of Iron MetabolismFatima Zuhra100% (1)
- Anemia Ferropenica Rev2019Document18 pagesAnemia Ferropenica Rev2019Albamis MojicaNo ratings yet
- Intravenous Iron Use in The Care of Patients With Kidney DiseaseDocument3 pagesIntravenous Iron Use in The Care of Patients With Kidney DiseaseAntika CahyatiNo ratings yet
- Anemia y Tracto GiDocument5 pagesAnemia y Tracto GiCarlos MichasNo ratings yet
- Blood Disorders in GeriatricDocument29 pagesBlood Disorders in GeriatricdheaNo ratings yet
- Contoh Artikel Ilmiah 2Document31 pagesContoh Artikel Ilmiah 2Bejo orang pintarNo ratings yet
- IDA HOMEWORK (2016510024-Putri Nurhisiyah Madya Jamil)Document9 pagesIDA HOMEWORK (2016510024-Putri Nurhisiyah Madya Jamil)Shanon LimNo ratings yet
- Camaschella 2017Document9 pagesCamaschella 2017Walter Jhon Delgadillo Arone0% (1)
- Iron Deficiency in CKD PatientsDocument49 pagesIron Deficiency in CKD Patientsswap58warNo ratings yet
- Iron DeficiencyDocument16 pagesIron DeficiencyBobby Faisyal RakhmanNo ratings yet
- J1-T5 Anemia FerropénicaDocument12 pagesJ1-T5 Anemia FerropénicaGoblin HunterNo ratings yet
- Nutrion Terapi of AnemiaDocument4 pagesNutrion Terapi of AnemiaRian LianNo ratings yet
- Iron Deficiency Anemia in Chronic Kidney Disease: ReviewDocument7 pagesIron Deficiency Anemia in Chronic Kidney Disease: ReviewSundas Ejaz100% (1)
- Complementary and Alternative Medical Lab Testing Part 16: HematologyFrom EverandComplementary and Alternative Medical Lab Testing Part 16: HematologyNo ratings yet
- FT Onduleur TS906S TS9010S 6KVDocument3 pagesFT Onduleur TS906S TS9010S 6KVdr_joe23No ratings yet
- Analisis ClinicosDocument6 pagesAnalisis Clinicosdr_joe23No ratings yet
- AnemiaDocument2 pagesAnemiadr_joe23No ratings yet
- OL Support MatrixDocument14 pagesOL Support Matrixdr_joe23No ratings yet
- Plants 11 02359Document17 pagesPlants 11 02359dr_joe23No ratings yet
- 02 571-572-575 FIBRIPHEN v4 2021-01Document2 pages02 571-572-575 FIBRIPHEN v4 2021-01dr_joe23No ratings yet
- Mdbsis04 Bili T-Dmso 2017Document4 pagesMdbsis04 Bili T-Dmso 2017dr_joe23No ratings yet
- Blood Research and DisordersDocument5 pagesBlood Research and Disordersdr_joe23No ratings yet
- At 13450Document2 pagesAt 13450dr_joe23No ratings yet
- At 13660Document2 pagesAt 13660dr_joe23No ratings yet
- At 13704Document2 pagesAt 13704dr_joe23No ratings yet
- CDC Reports Two Cases of Hiv Transmission in Household SettingDocument1 pageCDC Reports Two Cases of Hiv Transmission in Household Settingdr_joe23No ratings yet
- 3 5 barracudaDS1900 14 2007US en - CADocument3 pages3 5 barracudaDS1900 14 2007US en - CAdr_joe23No ratings yet
- EJMCM - Volume 8 - Issue 3 - Pages 2605-2615Document11 pagesEJMCM - Volume 8 - Issue 3 - Pages 2605-2615dr_joe23No ratings yet
- SD Biosensor F COVID 19 Antigen TestDocument1 pageSD Biosensor F COVID 19 Antigen Testdr_joe23No ratings yet
- Liste Tests Antigeniques Cle81c29b-1Document4 pagesListe Tests Antigeniques Cle81c29b-1dr_joe23No ratings yet
- Westgard Control QualityDocument9 pagesWestgard Control Qualitydr_joe23No ratings yet
- Hereditary Hemochromatosis and Iron MetabolismDocument8 pagesHereditary Hemochromatosis and Iron MetabolismVienne Yuen Wing YanNo ratings yet
- Plasma ProteinDocument102 pagesPlasma ProteinazeemNo ratings yet
- A Toxicity Study On Kantha ChendrumDocument99 pagesA Toxicity Study On Kantha Chendrumjmanuel108yahoo.co.ukNo ratings yet
- Shady 11Document96 pagesShady 11Amal AlameenNo ratings yet
- Iron Deficiency and Congestive Heart FailureDocument3 pagesIron Deficiency and Congestive Heart FailureEnzoNo ratings yet
- HEMATOLOGY Chapter 20 Rodaks Hematology, 5E (2016)Document14 pagesHEMATOLOGY Chapter 20 Rodaks Hematology, 5E (2016)Sachi Xandria de LaraNo ratings yet
- Clsi H17 ADocument59 pagesClsi H17 ACristian Gutiérrez VeraNo ratings yet
- Access Fast Fact 2019Document46 pagesAccess Fast Fact 2019see naaNo ratings yet
- Pediatric Fever of Unknown Origin: Educational GapDocument14 pagesPediatric Fever of Unknown Origin: Educational GapPiegl-Gulácsy VeraNo ratings yet
- Basic - Haematology Notes - Updated AnggelosDocument123 pagesBasic - Haematology Notes - Updated AnggelosLorenz SmallNo ratings yet
- Synthesis of NanomaterialsDocument55 pagesSynthesis of Nanomaterialsusama chaudhryNo ratings yet
- Plasma ChonDocument41 pagesPlasma ChonTwinkle SalongaNo ratings yet
- Seizure: Soheila Zareifar, Hamid Reza Hosseinzadeh, Nader CohanDocument3 pagesSeizure: Soheila Zareifar, Hamid Reza Hosseinzadeh, Nader CohanFirda PotterNo ratings yet
- Anemia FerropenicaDocument14 pagesAnemia Ferropenicajuliana hernandez herreraNo ratings yet
- Fasting Blood GlucoseDocument7 pagesFasting Blood GlucosegoddeyNo ratings yet
- Ferritin Lab PDFDocument6 pagesFerritin Lab PDFPoetri Iermayani100% (2)
- Minerals: From Essentials of Medical Biochemistry by R.C. GuptaDocument245 pagesMinerals: From Essentials of Medical Biochemistry by R.C. GuptaMalliga SundareshanNo ratings yet
- Diagnostic HemoglobinopathiesLaboratory Methods and Case StudiesDocument479 pagesDiagnostic HemoglobinopathiesLaboratory Methods and Case StudiesZia Uddin100% (2)
- 130201001M Ferritin 028120523 V1.0 EN 20120906Document4 pages130201001M Ferritin 028120523 V1.0 EN 20120906Nurhadi KebluksNo ratings yet
- 30 411 Vidas Ferritin: Summary and Explanation PrincipleDocument7 pages30 411 Vidas Ferritin: Summary and Explanation PrincipleIsti RismaNo ratings yet
- Anemia of Chronic Disease PDFDocument14 pagesAnemia of Chronic Disease PDFSuci PurnamaNo ratings yet
- Thyroid Symptom HackerDocument18 pagesThyroid Symptom HackerozergyalmoNo ratings yet
- Anemia InsomniaaaDocument4 pagesAnemia InsomniaaaBalqis SafariNo ratings yet
- Exogenous and Endogenous Pigment.....Document30 pagesExogenous and Endogenous Pigment.....Mohan ChoudharyNo ratings yet
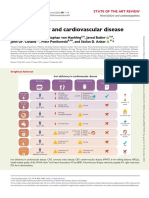
- Iron Deficiency and Cardiovascular DiseaseDocument14 pagesIron Deficiency and Cardiovascular DiseasemiguelalmenarezNo ratings yet
- Intravenous Iron UKDocument5 pagesIntravenous Iron UKmadimadi11No ratings yet
- Ferritin-Turbilatex: Store at 2 - 8ºCDocument4 pagesFerritin-Turbilatex: Store at 2 - 8ºCluisoft88No ratings yet
- Hyperferritinemia in Severe Dengue Infection .13Document8 pagesHyperferritinemia in Severe Dengue Infection .13rsthsn6z8xNo ratings yet
- Iron Deficiency Anaemia (IDA) Diagnosis: Dr. Saifeldein M. A. ElimamDocument33 pagesIron Deficiency Anaemia (IDA) Diagnosis: Dr. Saifeldein M. A. ElimamSaifeldein ElimamNo ratings yet
- Ferric Carboxymaltose (Hemojet) : Md. Arafat Hossain Brand Executive, SBMD, 01713354512Document5 pagesFerric Carboxymaltose (Hemojet) : Md. Arafat Hossain Brand Executive, SBMD, 01713354512Heranmoy Kumar Bijon100% (1)