Download as docx, pdf, or txt
You might also like
- HOPE Spiritual AssessmentDocument1 pageHOPE Spiritual AssessmentisrofahNo ratings yet
- Spirituality and ReligiosityDocument2 pagesSpirituality and ReligiosityRegine A. AnsongNo ratings yet
- Spirituality and ReligiousDocument29 pagesSpirituality and ReligiousMarissa ObmañaNo ratings yet
- Day 3 - Common Session 1 - Spirituality - DR VidyaDocument25 pagesDay 3 - Common Session 1 - Spirituality - DR Vidyam debNo ratings yet
- NCP Spiritual DistressDocument3 pagesNCP Spiritual DistressAngelo ArabejoNo ratings yet
- Hodge, D. R. (2013) - Assessing Spirituality and Religion in The Context of Counseling and Psychotherapy.Document31 pagesHodge, D. R. (2013) - Assessing Spirituality and Religion in The Context of Counseling and Psychotherapy.cassaNo ratings yet
- 10 Mental Wellness - Social and Emotional HealthDocument6 pages10 Mental Wellness - Social and Emotional HealthElvis Gonzalez-PerezNo ratings yet
- NCP Aug26Document2 pagesNCP Aug26adrelaiNo ratings yet
- Week 12Document4 pagesWeek 12Sal MiahNo ratings yet
- Spiritual & Psychosocial Issues in CareDocument3 pagesSpiritual & Psychosocial Issues in CareAlec Xavier Miranda100% (1)
- Distress SpiritualDocument13 pagesDistress SpiritualAdhit Nak BanjarmasinNo ratings yet
- Elective 11 ST Hand OutDocument2 pagesElective 11 ST Hand OuthahahahaaaaaaaNo ratings yet
- Gen 017 Lesson 9Document4 pagesGen 017 Lesson 9Carissa Mae Tapec EstradaNo ratings yet
- Gen 017 Lesson 9Document4 pagesGen 017 Lesson 9Carissa Mae Tapec EstradaNo ratings yet
- Introduction To Philosophy Module 2Document3 pagesIntroduction To Philosophy Module 2Allison DayNo ratings yet
- Spirituality: Spirituality and Related Concepts DescribedDocument8 pagesSpirituality: Spirituality and Related Concepts DescribedThea Cruz-AcantiladoNo ratings yet
- WEBINAR PPT - The Link Between Spirituality and Mental HealthDocument16 pagesWEBINAR PPT - The Link Between Spirituality and Mental HealthChannellMagluyanNo ratings yet
- GSelf - Midterms THE SPIRITUAL SELFDocument2 pagesGSelf - Midterms THE SPIRITUAL SELFJunfel ZablanNo ratings yet
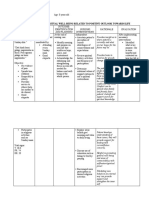
- Nursing Care Plan: Spiritual DistressDocument1 pageNursing Care Plan: Spiritual DistressRosalinda SalvadorNo ratings yet
- UTSDocument2 pagesUTStdv7f2y8mwNo ratings yet
- (D.0082) Distres SpiritualDocument3 pages(D.0082) Distres SpiritualRifky FaishalNo ratings yet
- Nursing Assessment of Spiritual NeedsDocument5 pagesNursing Assessment of Spiritual NeedsMarimiel PagulayanNo ratings yet
- Terapi Spiritual Dalam Praktis KlinikalDocument35 pagesTerapi Spiritual Dalam Praktis KlinikalYenie YenNo ratings yet
- Terapi Spiritual Dalam Praktis KlinikalDocument35 pagesTerapi Spiritual Dalam Praktis KlinikalYenie YenNo ratings yet
- IWRBS Module #2 Religion - Blessing and CurseDocument23 pagesIWRBS Module #2 Religion - Blessing and CurseLuigi ChristianNo ratings yet
- GeSocSci1 m5 7Document9 pagesGeSocSci1 m5 7Shells ChannelNo ratings yet
- Perdev Development As A WholeDocument2 pagesPerdev Development As A WholeGelay Gerlie Cadiente PitpitNo ratings yet
- NCM 114 Care For Older Adults MODULE 7Document5 pagesNCM 114 Care For Older Adults MODULE 7Meryville JacildoNo ratings yet
- 2016 DSRIP OneSheets SPA Spiritual Distress 1485449434Document2 pages2016 DSRIP OneSheets SPA Spiritual Distress 1485449434Victor Pariona aronaNo ratings yet
- Gulipardo Fidelity (Trifolds)Document3 pagesGulipardo Fidelity (Trifolds)Felicity Mae GulipardoNo ratings yet
- The Spiritual SelfDocument8 pagesThe Spiritual SelfJAY CEE SACRO100% (1)
- WhWhat Is The Stop MethodDocument2 pagesWhWhat Is The Stop Methodajcasillas29No ratings yet
- Depth and Transpersonal PsychologyDocument10 pagesDepth and Transpersonal PsychologyKelvinNo ratings yet
- 9 The Spiritual SelfDocument14 pages9 The Spiritual SelfCRUZ, ANNA MARIELLENo ratings yet
- C - Caple & Schub - 2020 - Spiritual Care - Providing To Children and Their FamiliesDocument5 pagesC - Caple & Schub - 2020 - Spiritual Care - Providing To Children and Their FamiliesDaniela AfonsoNo ratings yet
- CHAPTER 3-Developing The Whole PersonDocument13 pagesCHAPTER 3-Developing The Whole PersonJAMIE LEE TUAZONNo ratings yet
- Spiritual Care For Palliative PatientsDocument39 pagesSpiritual Care For Palliative PatientsDewi RosaNo ratings yet
- Article Review Christian ClientsDocument15 pagesArticle Review Christian ClientsCoco GuerreroNo ratings yet
- The Act and Moral CourageDocument29 pagesThe Act and Moral CourageEric KolimlimNo ratings yet
- PMSD NotesDocument2 pagesPMSD Noteschio0809No ratings yet
- THE SPIRITUAL SELF Uts6Document1 pageTHE SPIRITUAL SELF Uts6Kristel Grace OgtipNo ratings yet
- The Experience of Loss, Death and GriefDocument14 pagesThe Experience of Loss, Death and GriefAries Gulle MacalamNo ratings yet
- God Rest Our Hearts: Religiosity and Cognitive ReappraisalDocument11 pagesGod Rest Our Hearts: Religiosity and Cognitive ReappraisalPetrutaNo ratings yet
- Spiritual SelfDocument1 pageSpiritual SelfHannah MondillaNo ratings yet
- Francisco - PRELIM TASK - Spirituality & SexualityDocument2 pagesFrancisco - PRELIM TASK - Spirituality & SexualityKlara Jerica FranciscoNo ratings yet
- 8 The Spiritual SelfDocument4 pages8 The Spiritual SelfMicsjadeCastilloNo ratings yet
- B2 FHN InfographicDocument1 pageB2 FHN InfographicALDREIN JUDE SANTOSNo ratings yet
- Simpson Expo Poster - Ahmadu SimpsonDocument1 pageSimpson Expo Poster - Ahmadu SimpsonnurjNo ratings yet
- Uself - FinalsDocument7 pagesUself - Finals2022300913No ratings yet
- MM Psychosocial-Cultural Aspects in Nursing and Health ProfessionalsDocument1 pageMM Psychosocial-Cultural Aspects in Nursing and Health Professionalsptriw nigsihNo ratings yet
- Spirituality and ReligiosityDocument3 pagesSpirituality and ReligiosityJustineChloeNo ratings yet
- Pastoral Care Midterm TransDocument6 pagesPastoral Care Midterm Transset.b.rleNo ratings yet
- Advances in The Conceptualization and Measurement of Religion and SpiritualityDocument11 pagesAdvances in The Conceptualization and Measurement of Religion and SpiritualityfaouziaNo ratings yet
- Spirituality in Palliative Care - Byrne 2007Document7 pagesSpirituality in Palliative Care - Byrne 2007Mércia FiuzaNo ratings yet
- Life Stories of Recent MBADocument14 pagesLife Stories of Recent MBAMona Sahoo100% (1)
- Psychiatr Y and Spirituali TY: Moderator-Dr M Pravallika MAM Presenter - DR Yashwanth G Imh HyderabadDocument48 pagesPsychiatr Y and Spirituali TY: Moderator-Dr M Pravallika MAM Presenter - DR Yashwanth G Imh HyderabadRaviNo ratings yet
- Psychiatry and SpiritualityDocument48 pagesPsychiatry and SpiritualityRaviNo ratings yet
- AP Psychology - THERAPEUTIC APPROACHES TableDocument3 pagesAP Psychology - THERAPEUTIC APPROACHES TableneelNo ratings yet
- GE 1 Week 6 7 PPT From Sir Nikko 2Document28 pagesGE 1 Week 6 7 PPT From Sir Nikko 2Fake SilverNo ratings yet
- Demolishing Ancestral, Witchcraft, Evil Altar And Strongholds: 120 Prayers For Deliverance From Demons & Spirits, Blessings & BreakthroughFrom EverandDemolishing Ancestral, Witchcraft, Evil Altar And Strongholds: 120 Prayers For Deliverance From Demons & Spirits, Blessings & BreakthroughNo ratings yet
- Communication For Various PurposesDocument29 pagesCommunication For Various PurposesKristine PunzalanNo ratings yet
- Imtiaz C.BDocument22 pagesImtiaz C.BMohd ImtiazNo ratings yet
- Annals of The New York Academy of Sciences - 2021 - PellizzoniDocument13 pagesAnnals of The New York Academy of Sciences - 2021 - PellizzoniInes DuarteNo ratings yet
- Resume Chapter 7: Creating and Managing Organizational CultureDocument11 pagesResume Chapter 7: Creating and Managing Organizational CultureDelfian NurfauzanNo ratings yet
- UNIT 1 PlayDocument7 pagesUNIT 1 Playleneportugal0225No ratings yet
- Binge EatingDocument18 pagesBinge EatingIuliana IgnatNo ratings yet
- DLL Diss Week 6Document1 pageDLL Diss Week 6Judz SalibsNo ratings yet
- Selective Attention Improves Under Stress: Implications For Theories of Social CognitionDocument18 pagesSelective Attention Improves Under Stress: Implications For Theories of Social CognitionJing HuangNo ratings yet
- Learning Journal Examples Ey PDFDocument9 pagesLearning Journal Examples Ey PDFGagan Deep SinghNo ratings yet
- The Single Greatest Life Challenge. How Late Midlife Adults Construct Narratives of Significant Personal ChallengesDocument12 pagesThe Single Greatest Life Challenge. How Late Midlife Adults Construct Narratives of Significant Personal ChallengesRukmini SariNo ratings yet
- Rica Reflection Competency 3Document2 pagesRica Reflection Competency 3api-296624078No ratings yet
- Jose, Ana Katrina R. Gonzales, Mylene M. Doria, Ashley Joei B. Resuello, Mary Rose C. Rosario, Camila Andrei C. Garcia, Jomarie ADocument54 pagesJose, Ana Katrina R. Gonzales, Mylene M. Doria, Ashley Joei B. Resuello, Mary Rose C. Rosario, Camila Andrei C. Garcia, Jomarie ALysander GarciaNo ratings yet
- m2 ObjectiveDocument4 pagesm2 ObjectiveHải Trà NguyễnNo ratings yet
- 014lli Cruz NTDocument6 pages014lli Cruz NTedward9marcos9ortiz9No ratings yet
- Media Richness Theory SummaryDocument5 pagesMedia Richness Theory SummaryMatthewos HaileNo ratings yet
- 10 DOs and DONTs For Teaching Superflex 2015Document7 pages10 DOs and DONTs For Teaching Superflex 2015filipamaltez100% (2)
- Clinical Field Expereince DDocument5 pagesClinical Field Expereince Dapi-475628631100% (2)
- Module 1Document17 pagesModule 1Analyn Lisondra JuanitezNo ratings yet
- Eden Et Al. Action Research For Management Research. British Journal of Management. 1996Document12 pagesEden Et Al. Action Research For Management Research. British Journal of Management. 1996anapaulasoareslimaNo ratings yet
- Tourist Satisfaction and Repeat VisitationToward A New Comprehensive ModelDocument8 pagesTourist Satisfaction and Repeat VisitationToward A New Comprehensive ModeldfsdadNo ratings yet
- I410-Ecn-0199-2022-001-000168447 I410-Ecn-0199-2022-001-000168432Document20 pagesI410-Ecn-0199-2022-001-000168447 I410-Ecn-0199-2022-001-000168432pkrcgkpcm7No ratings yet
- Documented Reflection On Practice Arising From A Professional Discussion With A ColleagueDocument2 pagesDocumented Reflection On Practice Arising From A Professional Discussion With A Colleagueapi-530415478No ratings yet
- CHAPTER 4 - How Society Is OrganizedDocument12 pagesCHAPTER 4 - How Society Is Organizedkenthjoseph dahangNo ratings yet
- Language LabDocument3 pagesLanguage LabRishabh sikariaNo ratings yet
- Rorty - Kripke Versus KantDocument6 pagesRorty - Kripke Versus KantJavierNo ratings yet
- Fish in A Tree Vocabulary Lesson: Ccss - Ela-Literacy.L.6.6Document5 pagesFish in A Tree Vocabulary Lesson: Ccss - Ela-Literacy.L.6.6api-486620840No ratings yet
- Impact of Cross-Dressing in Determining Self-Objectification and Self-Esteem Among LGBT Community MembersDocument5 pagesImpact of Cross-Dressing in Determining Self-Objectification and Self-Esteem Among LGBT Community MembersDCRUZNo ratings yet
- DIT Clinician GuideDocument14 pagesDIT Clinician GuideVimal Singh ChauhanNo ratings yet
- 4 Ways To Improve Your Strategic Thinking SkillsDocument3 pages4 Ways To Improve Your Strategic Thinking SkillsJyothi MallyaNo ratings yet
- Why Focus Is Important?: Do You Often Ask YourselfDocument2 pagesWhy Focus Is Important?: Do You Often Ask YourselfSYED SOHAILNo ratings yet