
Targeting Inflammatory Pathways in Axial Spondyloarthritis
Targeting Inflammatory Pathways in Axial Spondyloarthritis
You might also like
- Voruganti and Bowness 2020 - New Developments in Our Understanding of Ankylosing Spondylitis Patho-AnnotatedDocument9 pagesVoruganti and Bowness 2020 - New Developments in Our Understanding of Ankylosing Spondylitis Patho-AnnotatedmuamarrayNo ratings yet
- Ni Hms 825760Document13 pagesNi Hms 825760Dea MustikaNo ratings yet
- BMS-CRR-2021-5-Final[45404]Document13 pagesBMS-CRR-2021-5-Final[45404]Prasham ShahNo ratings yet
- Vecellio Et Al. 2020 - The IL-17 - IL-23 Axis and Its Genetic Contribution To Psoriatic Arthritis-AnnotatedDocument10 pagesVecellio Et Al. 2020 - The IL-17 - IL-23 Axis and Its Genetic Contribution To Psoriatic Arthritis-AnnotatedmuamarrayNo ratings yet
- Update ON Psoriatic Arthritis: Epidemiology, Pathogenesis, Clinical Assessment and TreatmentDocument35 pagesUpdate ON Psoriatic Arthritis: Epidemiology, Pathogenesis, Clinical Assessment and TreatmentSudeesh KumarNo ratings yet
- Biomedicines 11 02998Document48 pagesBiomedicines 11 02998erni manikNo ratings yet
- Pathophysiology of Peripheral Arterial Disease (PAD) : A Review On Oxidative DisordersDocument14 pagesPathophysiology of Peripheral Arterial Disease (PAD) : A Review On Oxidative DisordersDurga BasnetNo ratings yet
- Editorial: Editorial Current Drug Targets, 2007, Vol. 8, No. 4 491Document76 pagesEditorial: Editorial Current Drug Targets, 2007, Vol. 8, No. 4 491laraalvarenga5832No ratings yet
- 1 s2.0 S204908012101027X Main 1Document10 pages1 s2.0 S204908012101027X Main 1Amirah FaridahNo ratings yet
- JRD 30 4 220Document14 pagesJRD 30 4 220Muhammad RijalNo ratings yet
- Old and New Therapeutic Strategies in Systemic SclerosisDocument6 pagesOld and New Therapeutic Strategies in Systemic SclerosisJosé Javier Morales NúñezNo ratings yet
- Author: Section Editor: Deputy Editor:: Pathogenesis of Systemic Sclerosis (Scleroderma)Document24 pagesAuthor: Section Editor: Deputy Editor:: Pathogenesis of Systemic Sclerosis (Scleroderma)zakiNo ratings yet
- Molecular Mechanism RADocument2 pagesMolecular Mechanism RA7120Mantiqa Syafa Duvadillan GusrinNo ratings yet
- JurnalDocument7 pagesJurnalIntan Mega PratidianaNo ratings yet
- Endotel Disfungsi PDFDocument26 pagesEndotel Disfungsi PDFAgus SyaifudinNo ratings yet
- The Complexity of Molecular Processes in Osteoarthritis of The Knee JointDocument10 pagesThe Complexity of Molecular Processes in Osteoarthritis of The Knee JointRita DiabNo ratings yet
- SS and Vascular DamageDocument9 pagesSS and Vascular DamageSergio CerpaNo ratings yet
- Defining The Phenotype, Pathogenesis and Treatment of Crohn'sDocument12 pagesDefining The Phenotype, Pathogenesis and Treatment of Crohn'sJEAN CERNA SOLISNo ratings yet
- Structural Disease Modification in Axial Spondyloarthritis 2023Document12 pagesStructural Disease Modification in Axial Spondyloarthritis 2023yokotoyNo ratings yet
- FulltextDocument7 pagesFulltextmohamedNo ratings yet
- In Ammation and Atherosclerosis: Signaling Pathways and Therapeutic InterventionDocument24 pagesIn Ammation and Atherosclerosis: Signaling Pathways and Therapeutic InterventionZahroNo ratings yet
- Cardioprotective role of GTS-21 by attenuating the TLR4/NF-κB pathway in streptozotocin-induced diabetic cardiomyopathy in ratsDocument21 pagesCardioprotective role of GTS-21 by attenuating the TLR4/NF-κB pathway in streptozotocin-induced diabetic cardiomyopathy in ratsvtrang0310No ratings yet
- Yjbm 92 4 629Document12 pagesYjbm 92 4 629Alfonso Ga MaNo ratings yet
- 5-Current Vascular Pharmacology - 2015 - 13 (6) 749-58 - Parenti Et AlDocument10 pages5-Current Vascular Pharmacology - 2015 - 13 (6) 749-58 - Parenti Et AlSara PaccosiNo ratings yet
- s13075 018 1624 XDocument15 pagess13075 018 1624 XDaniel Andrés Bulla GarcíaNo ratings yet
- JCM 11 06013Document12 pagesJCM 11 06013ryanNo ratings yet
- OsteoarthritisDocument14 pagesOsteoarthritisAssasination ClassroomNo ratings yet
- Ijms 23 01566 v3Document23 pagesIjms 23 01566 v3gck85fj8pnNo ratings yet
- Axial Psoriatic Arthritis An UpdateDocument10 pagesAxial Psoriatic Arthritis An Updateproject zoroNo ratings yet
- Review Injeksi Intraartikular Pada OA LututDocument12 pagesReview Injeksi Intraartikular Pada OA LututUmmu Qonitah AfnidawatiNo ratings yet
- Plantas Medicinales y Artrosis - ArtritisDocument8 pagesPlantas Medicinales y Artrosis - ArtritisSilvia Adriana Romero DiazNo ratings yet
- 2019 Tuft Cells ArthritisDocument21 pages2019 Tuft Cells Arthritispankaj27dataNo ratings yet
- Journal Pone 0252116Document16 pagesJournal Pone 0252116canhtung1989No ratings yet
- Biochemistry and Biophysics Reports: SciencedirectDocument7 pagesBiochemistry and Biophysics Reports: Sciencedirectedlinkusuma131No ratings yet
- Ankylosing SpondylitisDocument14 pagesAnkylosing SpondylitisJoao MinhoNo ratings yet
- 2019 Article 369 PDFDocument10 pages2019 Article 369 PDFAziir 'arNo ratings yet
- 2021 - Brazilian Society of Rheumatology 2020 Guidelines For Psoriatic ArthritisDocument27 pages2021 - Brazilian Society of Rheumatology 2020 Guidelines For Psoriatic ArthritisGustavo ResendeNo ratings yet
- Sjogren ReviewDocument11 pagesSjogren ReviewMariano AlbertalNo ratings yet
- Wright Et Al. 2016 - Ankylosing Spondylitis Patients Display Altered Den ... Hogenic Roles For The-AnnotatedDocument13 pagesWright Et Al. 2016 - Ankylosing Spondylitis Patients Display Altered Den ... Hogenic Roles For The-AnnotatedmuamarrayNo ratings yet
- Systemic Inflammatory Response SyndromeDocument16 pagesSystemic Inflammatory Response SyndromeRas RosarioNo ratings yet
- Bir RellDocument12 pagesBir RellGaudeamus IgiturNo ratings yet
- McInnes y Schett - 2017 - Pathogenetic Insights From The Treatment of RheumaDocument20 pagesMcInnes y Schett - 2017 - Pathogenetic Insights From The Treatment of Rheumabarrera2001No ratings yet
- Psoriatic Arthritis Nature ReviewDocument17 pagesPsoriatic Arthritis Nature ReviewJose Shaid Delgado OlveraNo ratings yet
- Ap 1Document7 pagesAp 1donkeyendutNo ratings yet
- Influence of Non-Steroid Anti-Inflammatory Drugs On The Hemostasis System in Patients With Rheumatoid ArthritisDocument7 pagesInfluence of Non-Steroid Anti-Inflammatory Drugs On The Hemostasis System in Patients With Rheumatoid Arthritisindex PubNo ratings yet
- Antibiotics 13 00046Document38 pagesAntibiotics 13 00046FatiaNo ratings yet
- Apnea and InflammationDocument19 pagesApnea and Inflammationarcm1949No ratings yet
- 1. inflamacion sinovial y progresionDocument41 pages1. inflamacion sinovial y progresionWilliams Nuñez EspetiaNo ratings yet
- Plebańczyk2019 Article DifferentSecretoryActivityOfArDocument12 pagesPlebańczyk2019 Article DifferentSecretoryActivityOfArasmaNo ratings yet
- Pathogenesis of Systemic Sclerosis Scleroderma UpToDateDocument27 pagesPathogenesis of Systemic Sclerosis Scleroderma UpToDateLê Hạ Long HảiNo ratings yet
- Novel Immune Cell Phenotypes in Spondyloarthritis PathogenesisDocument13 pagesNovel Immune Cell Phenotypes in Spondyloarthritis Pathogenesishendarto ArifNo ratings yet
- 2028 Full PDFDocument8 pages2028 Full PDFdhineyNo ratings yet
- 2021 - Brazilian Recomendations For The Use of NSAID in Axial SpondyloarthritisDocument21 pages2021 - Brazilian Recomendations For The Use of NSAID in Axial SpondyloarthritisGustavo ResendeNo ratings yet
- 2015 Update On MSCT LupusDocument9 pages2015 Update On MSCT LupusLily ChandraNo ratings yet
- Yashwanth Chinthapatla ReasearchDocument7 pagesYashwanth Chinthapatla Reasearchcapc9539No ratings yet
- Jurnal 2Document10 pagesJurnal 2abdi syahputraNo ratings yet
- Literature Review OsteoarthritisDocument10 pagesLiterature Review Osteoarthritisafdtbbhtz100% (1)
- Ankylosing SpondylitesDocument16 pagesAnkylosing SpondylitesJyotirmayeeNo ratings yet
- 10 3389-Fphys 2022 1011407-CitationDocument1 page10 3389-Fphys 2022 1011407-CitationlucaslevyalmoraesNo ratings yet
- Ankylosing SpondylitesDocument16 pagesAnkylosing SpondylitesJyotirmayeeNo ratings yet
- S94 - Harish Kumar Rao Manav Chowk Cc-Sahyogi Juneja Towers, 716, Rattangarh Road, Manav Chowk, Ambala CITY, PH-9996006678Document3 pagesS94 - Harish Kumar Rao Manav Chowk Cc-Sahyogi Juneja Towers, 716, Rattangarh Road, Manav Chowk, Ambala CITY, PH-9996006678EduNo ratings yet
- Treating Reactive Arthritis: Insights For The Clinician: John D. CarterDocument10 pagesTreating Reactive Arthritis: Insights For The Clinician: John D. CarterHoussam ElhousniNo ratings yet
- Dreams e Homoeo - 10th IssueDocument5 pagesDreams e Homoeo - 10th IssueSaurav AroraNo ratings yet
- 4ndzvyovxipmju1rfmhykayfDocument3 pages4ndzvyovxipmju1rfmhykayfKunal GuptaNo ratings yet
- Hypopyon UveitisDocument18 pagesHypopyon UveitisjochigNo ratings yet
- DR Adrian Jones - Seronegative SpondyloarthropathiesDocument38 pagesDR Adrian Jones - Seronegative SpondyloarthropathiesMaryam ShahbazNo ratings yet
- 233-Article Text-355-1-10-20200213Document17 pages233-Article Text-355-1-10-20200213Kristina ParasNo ratings yet
- Ankylosing SpondylitisDocument18 pagesAnkylosing SpondylitisIzni Fatihah100% (1)
- Spondiloartritis Diagnosis 2017 222234456Document40 pagesSpondiloartritis Diagnosis 2017 222234456Alexandra BalanNo ratings yet
- 1998 Does Knuckle Cracking Lead To Arthritis of The Fingers PDFDocument2 pages1998 Does Knuckle Cracking Lead To Arthritis of The Fingers PDFMatías RamírezNo ratings yet
- Diagnosis and Management of SpADocument65 pagesDiagnosis and Management of SpAishaan kharbandaNo ratings yet
- 1-CV Payeli 2023Document3 pages1-CV Payeli 2023shobhitbhargava39No ratings yet
- AS ContentServerDocument10 pagesAS ContentServerPurple CrystalNo ratings yet
- Spondyloarthritis ResidentDocument70 pagesSpondyloarthritis Residentviraaj pawar100% (1)
- Max2report PrintDocument6 pagesMax2report Printdevender0yadavNo ratings yet
- Ankylosing SpondylitisDocument12 pagesAnkylosing SpondylitisAnnette ChavezNo ratings yet
- Hla B27Document5 pagesHla B27Madhu Kunchi100% (1)
- Poligen & MultifaktorDocument49 pagesPoligen & MultifaktorLovina Falendini AndriNo ratings yet
- Ankylosing SpondylitisDocument30 pagesAnkylosing SpondylitisMohd ArifNo ratings yet
- Lec 2 Seronegative Spondarthritis (Slides)Document66 pagesLec 2 Seronegative Spondarthritis (Slides)amereNo ratings yet
- Hla B 27 SopDocument12 pagesHla B 27 SopRajeev PareekNo ratings yet
- Treating The Top Five Chronic Conditions Chris KresserDocument85 pagesTreating The Top Five Chronic Conditions Chris Kresserlamag100% (1)
- Chapter 65:: Psoriatic Arthritis and Reactive Arthritis:: Ana-Maria Orbai & John A. FlynnDocument12 pagesChapter 65:: Psoriatic Arthritis and Reactive Arthritis:: Ana-Maria Orbai & John A. FlynnDeb100% (1)
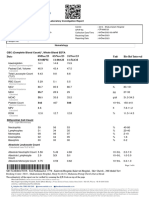
- DR Lal Pathlabs: LPL - Lpl-Rohini (National Reference Lab) Sector - 18, Block - E Rohini Delhi 110085Document2 pagesDR Lal Pathlabs: LPL - Lpl-Rohini (National Reference Lab) Sector - 18, Block - E Rohini Delhi 110085Vivek PatelNo ratings yet
- Enteropathic Spondyloarthritis: From Diagnosis To Treatment: Clinical and Developmental Immunology January 2013Document13 pagesEnteropathic Spondyloarthritis: From Diagnosis To Treatment: Clinical and Developmental Immunology January 2013Miki MausNo ratings yet
- SpondyloarthritisDocument17 pagesSpondyloarthritisla_vayettezNo ratings yet
- Himanshu EdtedDocument6 pagesHimanshu Edteddevender0yadavNo ratings yet
- Anesthetic Considerations in Patients Posted For Surgery With Ankylosing SpondylitisDocument43 pagesAnesthetic Considerations in Patients Posted For Surgery With Ankylosing Spondylitisanuk_1129No ratings yet
- ITD77731 - CPL DiagnosticDocument1 pageITD77731 - CPL Diagnosticdhananjay chaudharyNo ratings yet


![BMS-CRR-2021-5-Final[45404]](https://imgv2-1-f.scribdassets.com/img/document/749653184/149x198/233a68edfc/1720698524?v=1)




















































































Download as pdf or txt
You might also like
- Voruganti and Bowness 2020 - New Developments in Our Understanding of Ankylosing Spondylitis Patho-AnnotatedDocument9 pagesVoruganti and Bowness 2020 - New Developments in Our Understanding of Ankylosing Spondylitis Patho-AnnotatedmuamarrayNo ratings yet
- Ni Hms 825760Document13 pagesNi Hms 825760Dea MustikaNo ratings yet
- BMS-CRR-2021-5-Final[45404]Document13 pagesBMS-CRR-2021-5-Final[45404]Prasham ShahNo ratings yet
- Vecellio Et Al. 2020 - The IL-17 - IL-23 Axis and Its Genetic Contribution To Psoriatic Arthritis-AnnotatedDocument10 pagesVecellio Et Al. 2020 - The IL-17 - IL-23 Axis and Its Genetic Contribution To Psoriatic Arthritis-AnnotatedmuamarrayNo ratings yet
- Update ON Psoriatic Arthritis: Epidemiology, Pathogenesis, Clinical Assessment and TreatmentDocument35 pagesUpdate ON Psoriatic Arthritis: Epidemiology, Pathogenesis, Clinical Assessment and TreatmentSudeesh KumarNo ratings yet
- Biomedicines 11 02998Document48 pagesBiomedicines 11 02998erni manikNo ratings yet
- Pathophysiology of Peripheral Arterial Disease (PAD) : A Review On Oxidative DisordersDocument14 pagesPathophysiology of Peripheral Arterial Disease (PAD) : A Review On Oxidative DisordersDurga BasnetNo ratings yet
- Editorial: Editorial Current Drug Targets, 2007, Vol. 8, No. 4 491Document76 pagesEditorial: Editorial Current Drug Targets, 2007, Vol. 8, No. 4 491laraalvarenga5832No ratings yet
- 1 s2.0 S204908012101027X Main 1Document10 pages1 s2.0 S204908012101027X Main 1Amirah FaridahNo ratings yet
- JRD 30 4 220Document14 pagesJRD 30 4 220Muhammad RijalNo ratings yet
- Old and New Therapeutic Strategies in Systemic SclerosisDocument6 pagesOld and New Therapeutic Strategies in Systemic SclerosisJosé Javier Morales NúñezNo ratings yet
- Author: Section Editor: Deputy Editor:: Pathogenesis of Systemic Sclerosis (Scleroderma)Document24 pagesAuthor: Section Editor: Deputy Editor:: Pathogenesis of Systemic Sclerosis (Scleroderma)zakiNo ratings yet
- Molecular Mechanism RADocument2 pagesMolecular Mechanism RA7120Mantiqa Syafa Duvadillan GusrinNo ratings yet
- JurnalDocument7 pagesJurnalIntan Mega PratidianaNo ratings yet
- Endotel Disfungsi PDFDocument26 pagesEndotel Disfungsi PDFAgus SyaifudinNo ratings yet
- The Complexity of Molecular Processes in Osteoarthritis of The Knee JointDocument10 pagesThe Complexity of Molecular Processes in Osteoarthritis of The Knee JointRita DiabNo ratings yet
- SS and Vascular DamageDocument9 pagesSS and Vascular DamageSergio CerpaNo ratings yet
- Defining The Phenotype, Pathogenesis and Treatment of Crohn'sDocument12 pagesDefining The Phenotype, Pathogenesis and Treatment of Crohn'sJEAN CERNA SOLISNo ratings yet
- Structural Disease Modification in Axial Spondyloarthritis 2023Document12 pagesStructural Disease Modification in Axial Spondyloarthritis 2023yokotoyNo ratings yet
- FulltextDocument7 pagesFulltextmohamedNo ratings yet
- In Ammation and Atherosclerosis: Signaling Pathways and Therapeutic InterventionDocument24 pagesIn Ammation and Atherosclerosis: Signaling Pathways and Therapeutic InterventionZahroNo ratings yet
- Cardioprotective role of GTS-21 by attenuating the TLR4/NF-κB pathway in streptozotocin-induced diabetic cardiomyopathy in ratsDocument21 pagesCardioprotective role of GTS-21 by attenuating the TLR4/NF-κB pathway in streptozotocin-induced diabetic cardiomyopathy in ratsvtrang0310No ratings yet
- Yjbm 92 4 629Document12 pagesYjbm 92 4 629Alfonso Ga MaNo ratings yet
- 5-Current Vascular Pharmacology - 2015 - 13 (6) 749-58 - Parenti Et AlDocument10 pages5-Current Vascular Pharmacology - 2015 - 13 (6) 749-58 - Parenti Et AlSara PaccosiNo ratings yet
- s13075 018 1624 XDocument15 pagess13075 018 1624 XDaniel Andrés Bulla GarcíaNo ratings yet
- JCM 11 06013Document12 pagesJCM 11 06013ryanNo ratings yet
- OsteoarthritisDocument14 pagesOsteoarthritisAssasination ClassroomNo ratings yet
- Ijms 23 01566 v3Document23 pagesIjms 23 01566 v3gck85fj8pnNo ratings yet
- Axial Psoriatic Arthritis An UpdateDocument10 pagesAxial Psoriatic Arthritis An Updateproject zoroNo ratings yet
- Review Injeksi Intraartikular Pada OA LututDocument12 pagesReview Injeksi Intraartikular Pada OA LututUmmu Qonitah AfnidawatiNo ratings yet
- Plantas Medicinales y Artrosis - ArtritisDocument8 pagesPlantas Medicinales y Artrosis - ArtritisSilvia Adriana Romero DiazNo ratings yet
- 2019 Tuft Cells ArthritisDocument21 pages2019 Tuft Cells Arthritispankaj27dataNo ratings yet
- Journal Pone 0252116Document16 pagesJournal Pone 0252116canhtung1989No ratings yet
- Biochemistry and Biophysics Reports: SciencedirectDocument7 pagesBiochemistry and Biophysics Reports: Sciencedirectedlinkusuma131No ratings yet
- Ankylosing SpondylitisDocument14 pagesAnkylosing SpondylitisJoao MinhoNo ratings yet
- 2019 Article 369 PDFDocument10 pages2019 Article 369 PDFAziir 'arNo ratings yet
- 2021 - Brazilian Society of Rheumatology 2020 Guidelines For Psoriatic ArthritisDocument27 pages2021 - Brazilian Society of Rheumatology 2020 Guidelines For Psoriatic ArthritisGustavo ResendeNo ratings yet
- Sjogren ReviewDocument11 pagesSjogren ReviewMariano AlbertalNo ratings yet
- Wright Et Al. 2016 - Ankylosing Spondylitis Patients Display Altered Den ... Hogenic Roles For The-AnnotatedDocument13 pagesWright Et Al. 2016 - Ankylosing Spondylitis Patients Display Altered Den ... Hogenic Roles For The-AnnotatedmuamarrayNo ratings yet
- Systemic Inflammatory Response SyndromeDocument16 pagesSystemic Inflammatory Response SyndromeRas RosarioNo ratings yet
- Bir RellDocument12 pagesBir RellGaudeamus IgiturNo ratings yet
- McInnes y Schett - 2017 - Pathogenetic Insights From The Treatment of RheumaDocument20 pagesMcInnes y Schett - 2017 - Pathogenetic Insights From The Treatment of Rheumabarrera2001No ratings yet
- Psoriatic Arthritis Nature ReviewDocument17 pagesPsoriatic Arthritis Nature ReviewJose Shaid Delgado OlveraNo ratings yet
- Ap 1Document7 pagesAp 1donkeyendutNo ratings yet
- Influence of Non-Steroid Anti-Inflammatory Drugs On The Hemostasis System in Patients With Rheumatoid ArthritisDocument7 pagesInfluence of Non-Steroid Anti-Inflammatory Drugs On The Hemostasis System in Patients With Rheumatoid Arthritisindex PubNo ratings yet
- Antibiotics 13 00046Document38 pagesAntibiotics 13 00046FatiaNo ratings yet
- Apnea and InflammationDocument19 pagesApnea and Inflammationarcm1949No ratings yet
- 1. inflamacion sinovial y progresionDocument41 pages1. inflamacion sinovial y progresionWilliams Nuñez EspetiaNo ratings yet
- Plebańczyk2019 Article DifferentSecretoryActivityOfArDocument12 pagesPlebańczyk2019 Article DifferentSecretoryActivityOfArasmaNo ratings yet
- Pathogenesis of Systemic Sclerosis Scleroderma UpToDateDocument27 pagesPathogenesis of Systemic Sclerosis Scleroderma UpToDateLê Hạ Long HảiNo ratings yet
- Novel Immune Cell Phenotypes in Spondyloarthritis PathogenesisDocument13 pagesNovel Immune Cell Phenotypes in Spondyloarthritis Pathogenesishendarto ArifNo ratings yet
- 2028 Full PDFDocument8 pages2028 Full PDFdhineyNo ratings yet
- 2021 - Brazilian Recomendations For The Use of NSAID in Axial SpondyloarthritisDocument21 pages2021 - Brazilian Recomendations For The Use of NSAID in Axial SpondyloarthritisGustavo ResendeNo ratings yet
- 2015 Update On MSCT LupusDocument9 pages2015 Update On MSCT LupusLily ChandraNo ratings yet
- Yashwanth Chinthapatla ReasearchDocument7 pagesYashwanth Chinthapatla Reasearchcapc9539No ratings yet
- Jurnal 2Document10 pagesJurnal 2abdi syahputraNo ratings yet
- Literature Review OsteoarthritisDocument10 pagesLiterature Review Osteoarthritisafdtbbhtz100% (1)
- Ankylosing SpondylitesDocument16 pagesAnkylosing SpondylitesJyotirmayeeNo ratings yet
- 10 3389-Fphys 2022 1011407-CitationDocument1 page10 3389-Fphys 2022 1011407-CitationlucaslevyalmoraesNo ratings yet
- Ankylosing SpondylitesDocument16 pagesAnkylosing SpondylitesJyotirmayeeNo ratings yet
- S94 - Harish Kumar Rao Manav Chowk Cc-Sahyogi Juneja Towers, 716, Rattangarh Road, Manav Chowk, Ambala CITY, PH-9996006678Document3 pagesS94 - Harish Kumar Rao Manav Chowk Cc-Sahyogi Juneja Towers, 716, Rattangarh Road, Manav Chowk, Ambala CITY, PH-9996006678EduNo ratings yet
- Treating Reactive Arthritis: Insights For The Clinician: John D. CarterDocument10 pagesTreating Reactive Arthritis: Insights For The Clinician: John D. CarterHoussam ElhousniNo ratings yet
- Dreams e Homoeo - 10th IssueDocument5 pagesDreams e Homoeo - 10th IssueSaurav AroraNo ratings yet
- 4ndzvyovxipmju1rfmhykayfDocument3 pages4ndzvyovxipmju1rfmhykayfKunal GuptaNo ratings yet
- Hypopyon UveitisDocument18 pagesHypopyon UveitisjochigNo ratings yet
- DR Adrian Jones - Seronegative SpondyloarthropathiesDocument38 pagesDR Adrian Jones - Seronegative SpondyloarthropathiesMaryam ShahbazNo ratings yet
- 233-Article Text-355-1-10-20200213Document17 pages233-Article Text-355-1-10-20200213Kristina ParasNo ratings yet
- Ankylosing SpondylitisDocument18 pagesAnkylosing SpondylitisIzni Fatihah100% (1)
- Spondiloartritis Diagnosis 2017 222234456Document40 pagesSpondiloartritis Diagnosis 2017 222234456Alexandra BalanNo ratings yet
- 1998 Does Knuckle Cracking Lead To Arthritis of The Fingers PDFDocument2 pages1998 Does Knuckle Cracking Lead To Arthritis of The Fingers PDFMatías RamírezNo ratings yet
- Diagnosis and Management of SpADocument65 pagesDiagnosis and Management of SpAishaan kharbandaNo ratings yet
- 1-CV Payeli 2023Document3 pages1-CV Payeli 2023shobhitbhargava39No ratings yet
- AS ContentServerDocument10 pagesAS ContentServerPurple CrystalNo ratings yet
- Spondyloarthritis ResidentDocument70 pagesSpondyloarthritis Residentviraaj pawar100% (1)
- Max2report PrintDocument6 pagesMax2report Printdevender0yadavNo ratings yet
- Ankylosing SpondylitisDocument12 pagesAnkylosing SpondylitisAnnette ChavezNo ratings yet
- Hla B27Document5 pagesHla B27Madhu Kunchi100% (1)
- Poligen & MultifaktorDocument49 pagesPoligen & MultifaktorLovina Falendini AndriNo ratings yet
- Ankylosing SpondylitisDocument30 pagesAnkylosing SpondylitisMohd ArifNo ratings yet
- Lec 2 Seronegative Spondarthritis (Slides)Document66 pagesLec 2 Seronegative Spondarthritis (Slides)amereNo ratings yet
- Hla B 27 SopDocument12 pagesHla B 27 SopRajeev PareekNo ratings yet
- Treating The Top Five Chronic Conditions Chris KresserDocument85 pagesTreating The Top Five Chronic Conditions Chris Kresserlamag100% (1)
- Chapter 65:: Psoriatic Arthritis and Reactive Arthritis:: Ana-Maria Orbai & John A. FlynnDocument12 pagesChapter 65:: Psoriatic Arthritis and Reactive Arthritis:: Ana-Maria Orbai & John A. FlynnDeb100% (1)
- DR Lal Pathlabs: LPL - Lpl-Rohini (National Reference Lab) Sector - 18, Block - E Rohini Delhi 110085Document2 pagesDR Lal Pathlabs: LPL - Lpl-Rohini (National Reference Lab) Sector - 18, Block - E Rohini Delhi 110085Vivek PatelNo ratings yet
- Enteropathic Spondyloarthritis: From Diagnosis To Treatment: Clinical and Developmental Immunology January 2013Document13 pagesEnteropathic Spondyloarthritis: From Diagnosis To Treatment: Clinical and Developmental Immunology January 2013Miki MausNo ratings yet
- SpondyloarthritisDocument17 pagesSpondyloarthritisla_vayettezNo ratings yet
- Himanshu EdtedDocument6 pagesHimanshu Edteddevender0yadavNo ratings yet
- Anesthetic Considerations in Patients Posted For Surgery With Ankylosing SpondylitisDocument43 pagesAnesthetic Considerations in Patients Posted For Surgery With Ankylosing Spondylitisanuk_1129No ratings yet
- ITD77731 - CPL DiagnosticDocument1 pageITD77731 - CPL Diagnosticdhananjay chaudharyNo ratings yet