
March 2023 March 2023: Iap Executive Committee - 2023
March 2023 March 2023: Iap Executive Committee - 2023
You might also like
- Independent Investigation Into UCT Governance Final ReportDocument179 pagesIndependent Investigation Into UCT Governance Final ReportKrash King100% (4)
- 2 - Liberty Karaoke - All Songs by ArtistDocument78 pages2 - Liberty Karaoke - All Songs by ArtistAlanFowlerNo ratings yet
- Prosiding Faperta 2018 Fix PDFDocument676 pagesProsiding Faperta 2018 Fix PDFAgus Kaspun100% (1)
- Dixie General StoreDocument6 pagesDixie General StoreJoneceNo ratings yet
- Child India NewsletterDocument65 pagesChild India NewsletterAnsu MaliyakalNo ratings yet
- Child India March 2021Document35 pagesChild India March 2021suheena.CNo ratings yet
- Child India June 2022 - 220706 - 220739Document71 pagesChild India June 2022 - 220706 - 220739Harshavardhan VaikartanaNo ratings yet
- JwolnQgOHuGCN2F - ANNUAL REPORT 2022 IAPDocument80 pagesJwolnQgOHuGCN2F - ANNUAL REPORT 2022 IAPrahuhaldNo ratings yet
- Annual Report 2020-21 Insolvency and Bankruptcy Board of IndiaDocument144 pagesAnnual Report 2020-21 Insolvency and Bankruptcy Board of IndiaRheaNo ratings yet
- Volume 14 02Document611 pagesVolume 14 02අපේ පොත් එකතුවNo ratings yet
- Class 4 Maths Work Book Sem2 PDFDocument100 pagesClass 4 Maths Work Book Sem2 PDFaradhana avinashNo ratings yet
- Nepalese Journal On Geo-Informatics Number 2Document87 pagesNepalese Journal On Geo-Informatics Number 2Tri Dev AcharyaNo ratings yet
- Ej June15Document48 pagesEj June15SherNo ratings yet
- Avifauna of Ankodiya Village Pond, Vadodara District, GujaratDocument51 pagesAvifauna of Ankodiya Village Pond, Vadodara District, Gujaratsmodi_92No ratings yet
- 01 1 PDFDocument8 pages01 1 PDFpravikumar1989No ratings yet
- Class 3 Maths Sem 1 TM emDocument92 pagesClass 3 Maths Sem 1 TM emKalpana AttadaNo ratings yet
- DEP UdaipurDocument150 pagesDEP Udaipurkritikasinghk20No ratings yet
- Jurnal Equilibrium 2017 OkDocument184 pagesJurnal Equilibrium 2017 OkDeni Indra Purnama KotoNo ratings yet
- Acaademic Fest 2023 Final BrochureDocument10 pagesAcaademic Fest 2023 Final Brochuredrbishalchowdhury13No ratings yet
- Class 5 Maths Work Book Sem2 PDFDocument120 pagesClass 5 Maths Work Book Sem2 PDFaradhana avinash100% (1)
- Volume 09Document520 pagesVolume 09අපේ පොත් එකතුවNo ratings yet
- Class 2 Maths TM em Sem1Document96 pagesClass 2 Maths TM em Sem1Praneeth JohnNo ratings yet
- MIND MATTERS April 2023Document4 pagesMIND MATTERS April 2023Scholars HubNo ratings yet
- Imams-Mahima Jan13 PDFDocument64 pagesImams-Mahima Jan13 PDFAbhishek KumarNo ratings yet
- Office-Holders in Government of India PDFDocument6 pagesOffice-Holders in Government of India PDFGHAPRC RUDRAPURNo ratings yet
- 12th ATA Program Guide Final PDFDocument39 pages12th ATA Program Guide Final PDFjadigeetaNo ratings yet
- Mapping Key Populations For HIV Prevention in Sri LAnkaDocument53 pagesMapping Key Populations For HIV Prevention in Sri LAnkaDamith ChandimalNo ratings yet
- Draft Task Force Report On Promoting Affordable HousingDocument100 pagesDraft Task Force Report On Promoting Affordable HousingSonali NathNo ratings yet
- 1 NNMB Third Repeat Rural Survey Technicl Report 26 PDFDocument322 pages1 NNMB Third Repeat Rural Survey Technicl Report 26 PDFkoppinenipraneethNo ratings yet
- Ap Current Affairs - 2022Document39 pagesAp Current Affairs - 2022Manu GNo ratings yet
- Yog Sandesh Sep-09 EnglishDocument60 pagesYog Sandesh Sep-09 EnglishManmohan Gupta100% (2)
- PRAGYA BROCHURE AMRITSAR 27-28th DEC 2023Document5 pagesPRAGYA BROCHURE AMRITSAR 27-28th DEC 2023Anas KhanNo ratings yet
- India VaccineDocument59 pagesIndia VaccinefresitoNo ratings yet
- Pmrdfs Inaguration ReportDocument14 pagesPmrdfs Inaguration ReportSasha Vikas JainNo ratings yet
- PSC - RS - Exprot of Organic ProductsDocument88 pagesPSC - RS - Exprot of Organic Productsmansavi bihaniNo ratings yet
- E Annual ReportDocument54 pagesE Annual ReportAmit SharmaNo ratings yet
- 717Document423 pages717SAI SRIRAMNo ratings yet
- Odisha Review MagazineDocument116 pagesOdisha Review MagazineShantiswarup MahapatraNo ratings yet
- Fortune Select Grand Ridge HotelDocument6 pagesFortune Select Grand Ridge HotelMohammad NasirNo ratings yet
- Final Mission Sustainable India Volume-2Document113 pagesFinal Mission Sustainable India Volume-2Jeddie HapaniNo ratings yet
- Sujok Global MagazineDocument52 pagesSujok Global MagazineNidhi ShahNo ratings yet
- Isampe National Conference On Composites (Inccom 17)Document2 pagesIsampe National Conference On Composites (Inccom 17)Prashanth RajannaNo ratings yet
- TF April 22Document20 pagesTF April 22Ansh Singh100% (1)
- Modified District Monitor and District Observer of WbvaaDocument1 pageModified District Monitor and District Observer of WbvaaSamik PaulNo ratings yet
- "uq S"PQ - "qZO"o: ""Veda N Da Sarit''Document4 pages"uq S"PQ - "qZO"o: ""Veda N Da Sarit''SanthoshKumarNo ratings yet
- Bombay High Court Judgement On Fake Caste Certificate and Termination of ServiceDocument32 pagesBombay High Court Judgement On Fake Caste Certificate and Termination of ServiceVilas_123No ratings yet
- Minda Matters Issue 25 Lite Blue and WhiteDocument4 pagesMinda Matters Issue 25 Lite Blue and WhiteScholars HubNo ratings yet
- 99th AGM AR WEB 16 07 2018 PDFDocument184 pages99th AGM AR WEB 16 07 2018 PDFpks009No ratings yet
- Post of Nomination Name: President ElectDocument10 pagesPost of Nomination Name: President ElectMainak RoyNo ratings yet
- 28 MARCH Duty ChartDocument2 pages28 MARCH Duty ChartATUL PANDEYNo ratings yet
- Volume 17 02Document573 pagesVolume 17 02අපේ පොත් එකතුවNo ratings yet
- CHRIST DEEMED UNIVERSITY InterviewDocument20 pagesCHRIST DEEMED UNIVERSITY InterviewAchyuth AnandNo ratings yet
- NurseryDocument192 pagesNurserysameerpattnayak297No ratings yet
- VolXXI IssII Jan2020Document76 pagesVolXXI IssII Jan2020drsanthoshdeepaNo ratings yet
- Sonneratia 1Document16 pagesSonneratia 1Sailee Joshi-Gupte, Mangrove FoundationNo ratings yet
- Rainfall Atlas of Karnataka-2019Document196 pagesRainfall Atlas of Karnataka-2019vngsasNo ratings yet
- Swarajya Dec 23Document57 pagesSwarajya Dec 23Pramod KumarNo ratings yet
- Edited Swachha Bharat DocumentDocument12 pagesEdited Swachha Bharat DocumentĒ Vì LNo ratings yet
- 7th Class SocialDocument184 pages7th Class SocialRoshan GladstonNo ratings yet
- IMD KJ Choupal InvitationDocument1 pageIMD KJ Choupal InvitationAnika BassiNo ratings yet
- Voice & DysphagiaDocument8 pagesVoice & DysphagiaarpitaNo ratings yet
- Keerthi Question BankDocument65 pagesKeerthi Question BankKeerthanaNo ratings yet
- Department of Education: Schools Division of Ozamiz CityDocument3 pagesDepartment of Education: Schools Division of Ozamiz CityDoone Heart Santander Cabuguas100% (1)
- Tos Language Programs and Policies in Multilingual SocietiesDocument2 pagesTos Language Programs and Policies in Multilingual SocietiesBernadette Barro Gomez100% (1)
- November 2023Document1 pageNovember 2023innoozokoNo ratings yet
- 3 Chapter 3 Part 1 Foundations.Document40 pages3 Chapter 3 Part 1 Foundations.Enanye AragawNo ratings yet
- Return Service Accomplishment ReportDocument2 pagesReturn Service Accomplishment ReportJp TibayNo ratings yet
- Falta DatabaseDocument72 pagesFalta DatabaseTENDER AWADH GROUPNo ratings yet
- SG20KTL Data SheetDocument2 pagesSG20KTL Data SheetPaulo Cesar M CostaNo ratings yet
- Characteristics: AppearanceDocument2 pagesCharacteristics: AppearanceDimpleMakwanaNo ratings yet
- Application Form: Personal Secondary EducationDocument3 pagesApplication Form: Personal Secondary EducationRed PalustreNo ratings yet
- Pcol MnemonicsDocument12 pagesPcol MnemonicsJustine Rubillete Mendoza MarianoNo ratings yet
- Energy Efficiency Frameworks A Literature OverviewDocument10 pagesEnergy Efficiency Frameworks A Literature OverviewM VlogNo ratings yet
- Solutions Manual and Test Bank Operations and Supply Chain Management 3rd Edition JacobsDocument5 pagesSolutions Manual and Test Bank Operations and Supply Chain Management 3rd Edition Jacobsanie0% (1)
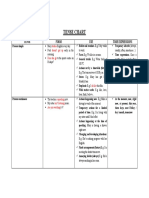
- TENSE CHART (Present Simple Vs Present Continuous)Document1 pageTENSE CHART (Present Simple Vs Present Continuous)Fmga GaNo ratings yet
- Sequencing of EventsDocument19 pagesSequencing of EventsGleen PayotNo ratings yet
- BISCI Chapter 14 TelecommunicationsDocument56 pagesBISCI Chapter 14 TelecommunicationsRod DevilleNo ratings yet
- FRB13089887411Document4 pagesFRB13089887411MAHA KAALNo ratings yet
- Nervous System Exam-Style Questions (+ Mark Scheme)Document20 pagesNervous System Exam-Style Questions (+ Mark Scheme)shakeel shahulNo ratings yet
- Dhan Allyn Romero 11 Saturn ABM EAPPDocument7 pagesDhan Allyn Romero 11 Saturn ABM EAPPJhevie RanileNo ratings yet
- Application Petition For Bail SampleDocument3 pagesApplication Petition For Bail SampleZed AbantasNo ratings yet
- Futuro (Will-Going To - P.C.)Document1 pageFuturo (Will-Going To - P.C.)carolina herreraNo ratings yet
- DPP - (19) 13th IOC - (E) - WADocument1 pageDPP - (19) 13th IOC - (E) - WAassadfNo ratings yet
- Chapter 2 PolynomialsDocument39 pagesChapter 2 PolynomialsRamesh RathoreNo ratings yet
- As An Employee of The Foreign Exchange Department For A LargeDocument1 pageAs An Employee of The Foreign Exchange Department For A Largetrilocksp SinghNo ratings yet
- NeutraceuticalsDocument36 pagesNeutraceuticalsMir ImranNo ratings yet
- Unit - V: PowerDocument32 pagesUnit - V: PowerVaira PerumalNo ratings yet
- P1-E (7-09) - Personnel InductionDocument4 pagesP1-E (7-09) - Personnel InductionDhotNo ratings yet
- Collins Sentence MemoDocument17 pagesCollins Sentence MemoRoy S. JohnsonNo ratings yet



















































































Download as pdf or txt
You might also like
- Independent Investigation Into UCT Governance Final ReportDocument179 pagesIndependent Investigation Into UCT Governance Final ReportKrash King100% (4)
- 2 - Liberty Karaoke - All Songs by ArtistDocument78 pages2 - Liberty Karaoke - All Songs by ArtistAlanFowlerNo ratings yet
- Prosiding Faperta 2018 Fix PDFDocument676 pagesProsiding Faperta 2018 Fix PDFAgus Kaspun100% (1)
- Dixie General StoreDocument6 pagesDixie General StoreJoneceNo ratings yet
- Child India NewsletterDocument65 pagesChild India NewsletterAnsu MaliyakalNo ratings yet
- Child India March 2021Document35 pagesChild India March 2021suheena.CNo ratings yet
- Child India June 2022 - 220706 - 220739Document71 pagesChild India June 2022 - 220706 - 220739Harshavardhan VaikartanaNo ratings yet
- JwolnQgOHuGCN2F - ANNUAL REPORT 2022 IAPDocument80 pagesJwolnQgOHuGCN2F - ANNUAL REPORT 2022 IAPrahuhaldNo ratings yet
- Annual Report 2020-21 Insolvency and Bankruptcy Board of IndiaDocument144 pagesAnnual Report 2020-21 Insolvency and Bankruptcy Board of IndiaRheaNo ratings yet
- Volume 14 02Document611 pagesVolume 14 02අපේ පොත් එකතුවNo ratings yet
- Class 4 Maths Work Book Sem2 PDFDocument100 pagesClass 4 Maths Work Book Sem2 PDFaradhana avinashNo ratings yet
- Nepalese Journal On Geo-Informatics Number 2Document87 pagesNepalese Journal On Geo-Informatics Number 2Tri Dev AcharyaNo ratings yet
- Ej June15Document48 pagesEj June15SherNo ratings yet
- Avifauna of Ankodiya Village Pond, Vadodara District, GujaratDocument51 pagesAvifauna of Ankodiya Village Pond, Vadodara District, Gujaratsmodi_92No ratings yet
- 01 1 PDFDocument8 pages01 1 PDFpravikumar1989No ratings yet
- Class 3 Maths Sem 1 TM emDocument92 pagesClass 3 Maths Sem 1 TM emKalpana AttadaNo ratings yet
- DEP UdaipurDocument150 pagesDEP Udaipurkritikasinghk20No ratings yet
- Jurnal Equilibrium 2017 OkDocument184 pagesJurnal Equilibrium 2017 OkDeni Indra Purnama KotoNo ratings yet
- Acaademic Fest 2023 Final BrochureDocument10 pagesAcaademic Fest 2023 Final Brochuredrbishalchowdhury13No ratings yet
- Class 5 Maths Work Book Sem2 PDFDocument120 pagesClass 5 Maths Work Book Sem2 PDFaradhana avinash100% (1)
- Volume 09Document520 pagesVolume 09අපේ පොත් එකතුවNo ratings yet
- Class 2 Maths TM em Sem1Document96 pagesClass 2 Maths TM em Sem1Praneeth JohnNo ratings yet
- MIND MATTERS April 2023Document4 pagesMIND MATTERS April 2023Scholars HubNo ratings yet
- Imams-Mahima Jan13 PDFDocument64 pagesImams-Mahima Jan13 PDFAbhishek KumarNo ratings yet
- Office-Holders in Government of India PDFDocument6 pagesOffice-Holders in Government of India PDFGHAPRC RUDRAPURNo ratings yet
- 12th ATA Program Guide Final PDFDocument39 pages12th ATA Program Guide Final PDFjadigeetaNo ratings yet
- Mapping Key Populations For HIV Prevention in Sri LAnkaDocument53 pagesMapping Key Populations For HIV Prevention in Sri LAnkaDamith ChandimalNo ratings yet
- Draft Task Force Report On Promoting Affordable HousingDocument100 pagesDraft Task Force Report On Promoting Affordable HousingSonali NathNo ratings yet
- 1 NNMB Third Repeat Rural Survey Technicl Report 26 PDFDocument322 pages1 NNMB Third Repeat Rural Survey Technicl Report 26 PDFkoppinenipraneethNo ratings yet
- Ap Current Affairs - 2022Document39 pagesAp Current Affairs - 2022Manu GNo ratings yet
- Yog Sandesh Sep-09 EnglishDocument60 pagesYog Sandesh Sep-09 EnglishManmohan Gupta100% (2)
- PRAGYA BROCHURE AMRITSAR 27-28th DEC 2023Document5 pagesPRAGYA BROCHURE AMRITSAR 27-28th DEC 2023Anas KhanNo ratings yet
- India VaccineDocument59 pagesIndia VaccinefresitoNo ratings yet
- Pmrdfs Inaguration ReportDocument14 pagesPmrdfs Inaguration ReportSasha Vikas JainNo ratings yet
- PSC - RS - Exprot of Organic ProductsDocument88 pagesPSC - RS - Exprot of Organic Productsmansavi bihaniNo ratings yet
- E Annual ReportDocument54 pagesE Annual ReportAmit SharmaNo ratings yet
- 717Document423 pages717SAI SRIRAMNo ratings yet
- Odisha Review MagazineDocument116 pagesOdisha Review MagazineShantiswarup MahapatraNo ratings yet
- Fortune Select Grand Ridge HotelDocument6 pagesFortune Select Grand Ridge HotelMohammad NasirNo ratings yet
- Final Mission Sustainable India Volume-2Document113 pagesFinal Mission Sustainable India Volume-2Jeddie HapaniNo ratings yet
- Sujok Global MagazineDocument52 pagesSujok Global MagazineNidhi ShahNo ratings yet
- Isampe National Conference On Composites (Inccom 17)Document2 pagesIsampe National Conference On Composites (Inccom 17)Prashanth RajannaNo ratings yet
- TF April 22Document20 pagesTF April 22Ansh Singh100% (1)
- Modified District Monitor and District Observer of WbvaaDocument1 pageModified District Monitor and District Observer of WbvaaSamik PaulNo ratings yet
- "uq S"PQ - "qZO"o: ""Veda N Da Sarit''Document4 pages"uq S"PQ - "qZO"o: ""Veda N Da Sarit''SanthoshKumarNo ratings yet
- Bombay High Court Judgement On Fake Caste Certificate and Termination of ServiceDocument32 pagesBombay High Court Judgement On Fake Caste Certificate and Termination of ServiceVilas_123No ratings yet
- Minda Matters Issue 25 Lite Blue and WhiteDocument4 pagesMinda Matters Issue 25 Lite Blue and WhiteScholars HubNo ratings yet
- 99th AGM AR WEB 16 07 2018 PDFDocument184 pages99th AGM AR WEB 16 07 2018 PDFpks009No ratings yet
- Post of Nomination Name: President ElectDocument10 pagesPost of Nomination Name: President ElectMainak RoyNo ratings yet
- 28 MARCH Duty ChartDocument2 pages28 MARCH Duty ChartATUL PANDEYNo ratings yet
- Volume 17 02Document573 pagesVolume 17 02අපේ පොත් එකතුවNo ratings yet
- CHRIST DEEMED UNIVERSITY InterviewDocument20 pagesCHRIST DEEMED UNIVERSITY InterviewAchyuth AnandNo ratings yet
- NurseryDocument192 pagesNurserysameerpattnayak297No ratings yet
- VolXXI IssII Jan2020Document76 pagesVolXXI IssII Jan2020drsanthoshdeepaNo ratings yet
- Sonneratia 1Document16 pagesSonneratia 1Sailee Joshi-Gupte, Mangrove FoundationNo ratings yet
- Rainfall Atlas of Karnataka-2019Document196 pagesRainfall Atlas of Karnataka-2019vngsasNo ratings yet
- Swarajya Dec 23Document57 pagesSwarajya Dec 23Pramod KumarNo ratings yet
- Edited Swachha Bharat DocumentDocument12 pagesEdited Swachha Bharat DocumentĒ Vì LNo ratings yet
- 7th Class SocialDocument184 pages7th Class SocialRoshan GladstonNo ratings yet
- IMD KJ Choupal InvitationDocument1 pageIMD KJ Choupal InvitationAnika BassiNo ratings yet
- Voice & DysphagiaDocument8 pagesVoice & DysphagiaarpitaNo ratings yet
- Keerthi Question BankDocument65 pagesKeerthi Question BankKeerthanaNo ratings yet
- Department of Education: Schools Division of Ozamiz CityDocument3 pagesDepartment of Education: Schools Division of Ozamiz CityDoone Heart Santander Cabuguas100% (1)
- Tos Language Programs and Policies in Multilingual SocietiesDocument2 pagesTos Language Programs and Policies in Multilingual SocietiesBernadette Barro Gomez100% (1)
- November 2023Document1 pageNovember 2023innoozokoNo ratings yet
- 3 Chapter 3 Part 1 Foundations.Document40 pages3 Chapter 3 Part 1 Foundations.Enanye AragawNo ratings yet
- Return Service Accomplishment ReportDocument2 pagesReturn Service Accomplishment ReportJp TibayNo ratings yet
- Falta DatabaseDocument72 pagesFalta DatabaseTENDER AWADH GROUPNo ratings yet
- SG20KTL Data SheetDocument2 pagesSG20KTL Data SheetPaulo Cesar M CostaNo ratings yet
- Characteristics: AppearanceDocument2 pagesCharacteristics: AppearanceDimpleMakwanaNo ratings yet
- Application Form: Personal Secondary EducationDocument3 pagesApplication Form: Personal Secondary EducationRed PalustreNo ratings yet
- Pcol MnemonicsDocument12 pagesPcol MnemonicsJustine Rubillete Mendoza MarianoNo ratings yet
- Energy Efficiency Frameworks A Literature OverviewDocument10 pagesEnergy Efficiency Frameworks A Literature OverviewM VlogNo ratings yet
- Solutions Manual and Test Bank Operations and Supply Chain Management 3rd Edition JacobsDocument5 pagesSolutions Manual and Test Bank Operations and Supply Chain Management 3rd Edition Jacobsanie0% (1)
- TENSE CHART (Present Simple Vs Present Continuous)Document1 pageTENSE CHART (Present Simple Vs Present Continuous)Fmga GaNo ratings yet
- Sequencing of EventsDocument19 pagesSequencing of EventsGleen PayotNo ratings yet
- BISCI Chapter 14 TelecommunicationsDocument56 pagesBISCI Chapter 14 TelecommunicationsRod DevilleNo ratings yet
- FRB13089887411Document4 pagesFRB13089887411MAHA KAALNo ratings yet
- Nervous System Exam-Style Questions (+ Mark Scheme)Document20 pagesNervous System Exam-Style Questions (+ Mark Scheme)shakeel shahulNo ratings yet
- Dhan Allyn Romero 11 Saturn ABM EAPPDocument7 pagesDhan Allyn Romero 11 Saturn ABM EAPPJhevie RanileNo ratings yet
- Application Petition For Bail SampleDocument3 pagesApplication Petition For Bail SampleZed AbantasNo ratings yet
- Futuro (Will-Going To - P.C.)Document1 pageFuturo (Will-Going To - P.C.)carolina herreraNo ratings yet
- DPP - (19) 13th IOC - (E) - WADocument1 pageDPP - (19) 13th IOC - (E) - WAassadfNo ratings yet
- Chapter 2 PolynomialsDocument39 pagesChapter 2 PolynomialsRamesh RathoreNo ratings yet
- As An Employee of The Foreign Exchange Department For A LargeDocument1 pageAs An Employee of The Foreign Exchange Department For A Largetrilocksp SinghNo ratings yet
- NeutraceuticalsDocument36 pagesNeutraceuticalsMir ImranNo ratings yet
- Unit - V: PowerDocument32 pagesUnit - V: PowerVaira PerumalNo ratings yet
- P1-E (7-09) - Personnel InductionDocument4 pagesP1-E (7-09) - Personnel InductionDhotNo ratings yet
- Collins Sentence MemoDocument17 pagesCollins Sentence MemoRoy S. JohnsonNo ratings yet