
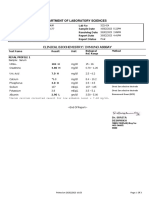
Laboratory Investigation Report: Haematology
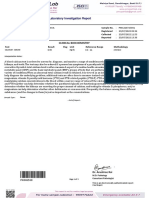
Laboratory Investigation Report: Haematology
You might also like
- Mrs Anar DeviDocument14 pagesMrs Anar DeviM.DNo ratings yet
- Xdue6378 2Document2 pagesXdue6378 2S Abedi50% (2)
- Essentials of Medical Laboratory Practice - Lieseke, Constance L. (SRG)Document564 pagesEssentials of Medical Laboratory Practice - Lieseke, Constance L. (SRG)Kaan Halici89% (36)
- Test Report: Complete Blood Count (CBC)Document3 pagesTest Report: Complete Blood Count (CBC)WSC ALMANo ratings yet
- 1-Dengue IgG & IgM - PO2709736085-377Document12 pages1-Dengue IgG & IgM - PO2709736085-377TV UNITNo ratings yet
- 1-Complete Blood Count - PO1106326185-399Document8 pages1-Complete Blood Count - PO1106326185-399Arup KumarNo ratings yet
- Department of Hematology Test Name Result Unit Bio. Ref. IntervalDocument3 pagesDepartment of Hematology Test Name Result Unit Bio. Ref. Intervalaf dNo ratings yet
- Design and Spatial BehaviorDocument24 pagesDesign and Spatial BehaviorHuiyiChang100% (1)
- Kinesiotape Durante El EmbarazoDocument3 pagesKinesiotape Durante El EmbarazoNostrum Sport100% (2)
- Medical Laboratory Report: Haemoglobin Total Leucocyte Count Total Erythrocyte Count Platelet Count MPV PCT PDWDocument4 pagesMedical Laboratory Report: Haemoglobin Total Leucocyte Count Total Erythrocyte Count Platelet Count MPV PCT PDWdhavalNo ratings yet
- Saniya Fathima (7G28Jy) :::: Patient Age / Sex 26 Y / Female BranchDocument3 pagesSaniya Fathima (7G28Jy) :::: Patient Age / Sex 26 Y / Female BranchShah FaisalNo ratings yet
- Kidney FunctionDocument19 pagesKidney FunctionFarooq Bin MahfoozNo ratings yet
- Medical Laboratory Report: Haemoglobin Total Leucocyte Count Total Erythrocyte Count Platelet Count MPV PCT PDWDocument4 pagesMedical Laboratory Report: Haemoglobin Total Leucocyte Count Total Erythrocyte Count Platelet Count MPV PCT PDWdhavalNo ratings yet
- Report 0bd39992Document8 pagesReport 0bd39992NEETFIXNo ratings yet
- Report 3f90266bDocument18 pagesReport 3f90266bSK TacNo ratings yet
- Ssumangarg@gmail - Com 20220825193722Document13 pagesSsumangarg@gmail - Com 20220825193722Suman GargNo ratings yet
- PRAVEEN Y (ID - 8167522) :::: Patient Age / Sex 32 Y / MaleDocument5 pagesPRAVEEN Y (ID - 8167522) :::: Patient Age / Sex 32 Y / Malepraveen yNo ratings yet
- 1-Senior Citizen Basic Package - PO3248534977-432Document16 pages1-Senior Citizen Basic Package - PO3248534977-432Krishna Nand RaiNo ratings yet
- Department of Hematology Test Name Result Unit Bio. Ref. IntervalDocument3 pagesDepartment of Hematology Test Name Result Unit Bio. Ref. Intervalaf dNo ratings yet
- Report of Mr. RAJA PDFDocument3 pagesReport of Mr. RAJA PDFraja.tyagi2125No ratings yet
- Method: Calculated: Page 1 of 9 07-Sep-2022 08:54 PMDocument10 pagesMethod: Calculated: Page 1 of 9 07-Sep-2022 08:54 PMburela_naveenNo ratings yet
- ReportDocument2 pagesReportIshikaNo ratings yet
- Don't Know Love - 1004584Document14 pagesDon't Know Love - 1004584baapj39No ratings yet
- Haematology: Investigation Observed Value Unit Biological Reference IntervalDocument5 pagesHaematology: Investigation Observed Value Unit Biological Reference Intervalshivanand.n ShivanandNo ratings yet
- LabTest 03jul2023Document5 pagesLabTest 03jul2023jkgupta0003No ratings yet
- Mirza Kayesh Begg - 250274290 - CompleteReportDocument12 pagesMirza Kayesh Begg - 250274290 - CompleteReportSYEDA MYSHA ALINo ratings yet
- Department of Hematology Comprehensive Full Body Checkup Test Name Result Unit Bio. Ref. IntervalDocument11 pagesDepartment of Hematology Comprehensive Full Body Checkup Test Name Result Unit Bio. Ref. IntervalshyamNo ratings yet
- Anjali Khapare - 23071171Document3 pagesAnjali Khapare - 23071171dr.menganeNo ratings yet
- Archana Lab ReportDocument10 pagesArchana Lab Reportprabalsoni125No ratings yet
- Lab ResultDocument7 pagesLab ResultAanshika RaizadaNo ratings yet
- Fully Automated Lab Accurate Reports Reports Verified by PathologistDocument11 pagesFully Automated Lab Accurate Reports Reports Verified by PathologistBathri NathanNo ratings yet
- Test Results Units Biological Reference Range Hematology:::::: Ms. Farha MemonDocument5 pagesTest Results Units Biological Reference Range Hematology:::::: Ms. Farha MemonKM GASTRO CENTERNo ratings yet
- Report 89594e5fDocument10 pagesReport 89594e5fNaresh SrikakolapuNo ratings yet
- 1-Senior Citizen Advanced Package - PO3427386675-856Document18 pages1-Senior Citizen Advanced Package - PO3427386675-856Ravi PrakashNo ratings yet
- Test Reports 2Document2 pagesTest Reports 2Chandrasekhara Reddy TNo ratings yet
- 8000000936: Patient ID 80001350 Sid No Nehru Nagar Branch Mr. Vasanth NDocument3 pages8000000936: Patient ID 80001350 Sid No Nehru Nagar Branch Mr. Vasanth NSudha SaravananNo ratings yet
- Medical Laboratory Report: Haemoglobin Total Leucocyte Count Total Erythrocyte Count Platelet Count MPV PCT PDWDocument4 pagesMedical Laboratory Report: Haemoglobin Total Leucocyte Count Total Erythrocyte Count Platelet Count MPV PCT PDWdhavalNo ratings yet
- Sunita NepalDocument5 pagesSunita NepalPrajay NepalNo ratings yet
- Aman CBCDocument1 pageAman CBCAman RathoreNo ratings yet
- Department of Hematology Test Name Result Unit Bio. Ref. IntervalDocument5 pagesDepartment of Hematology Test Name Result Unit Bio. Ref. IntervalHarishNo ratings yet
- Haematology: Investigation Observed Value Unit Biological Reference IntervalDocument2 pagesHaematology: Investigation Observed Value Unit Biological Reference IntervalVivek RadhakrishnanNo ratings yet
- MR Shashidhar Kulkarni 29 04 2023 02 35 25 PMDocument2 pagesMR Shashidhar Kulkarni 29 04 2023 02 35 25 PMagaymashashi2906No ratings yet
- Report 28340c20Document10 pagesReport 28340c20Rahul ChaudhariNo ratings yet
- Labreportnew - 2023-02-17T141822.094Document8 pagesLabreportnew - 2023-02-17T141822.094pavanimatteguntaNo ratings yet
- BloodDocument18 pagesBloodPriyanshu GuptaNo ratings yet
- Labreportnew - 2023-10-17T102750.286Document2 pagesLabreportnew - 2023-10-17T102750.286sidlab202No ratings yet
- 1-Good Health Premium Package - PO1065281239-651Document19 pages1-Good Health Premium Package - PO1065281239-651Renu ChoudharyNo ratings yet
- Haematology Haematology Haematology HaematologyDocument3 pagesHaematology Haematology Haematology HaematologyGopinandan PandeyNo ratings yet
- Jyoti Singh ReportsDocument5 pagesJyoti Singh ReportsRaghujyotisNo ratings yet
- Department of Hematology Test Name Result Unit Bio. Ref. IntervalDocument6 pagesDepartment of Hematology Test Name Result Unit Bio. Ref. IntervalHarishNo ratings yet
- Haematology: Investigation Observed Value Unit Biological Reference IntervalDocument6 pagesHaematology: Investigation Observed Value Unit Biological Reference IntervalumeshlpsNo ratings yet
- R Selvi:::: Patient Age / Sex 56 Y / Female BranchDocument7 pagesR Selvi:::: Patient Age / Sex 56 Y / Female Branchop nNo ratings yet
- LabReportNew - 2024-03-22T202901.640Document8 pagesLabReportNew - 2024-03-22T202901.640alex taylorNo ratings yet
- Department of Laboratory Sciences: Clinical Biochemistry/ Immuno AsssayDocument3 pagesDepartment of Laboratory Sciences: Clinical Biochemistry/ Immuno AsssayKavyaleen KaurNo ratings yet
- Fully Automated Lab Accurate Reports Reports Verified by PathologistDocument14 pagesFully Automated Lab Accurate Reports Reports Verified by PathologistRavindranatha AnNo ratings yet
- PathkindDocument5 pagesPathkindgovt.job4692No ratings yet
- Hematology: KongamdanaDocument1 pageHematology: KongamdanaShariqNo ratings yet
- Hematology: KongamdanaDocument1 pageHematology: KongamdanaShariqNo ratings yet
- IT217236 Report 1Document2 pagesIT217236 Report 1NamithaNo ratings yet
- Complete Blood Count (CBC) : Department of Haematology and Clinical PathologyDocument2 pagesComplete Blood Count (CBC) : Department of Haematology and Clinical PathologyNamithaNo ratings yet
- SR8188385Document2 pagesSR8188385mohanchowdhury1948No ratings yet
- MrsSANGEETASAHU 45Y FemaleDocument6 pagesMrsSANGEETASAHU 45Y FemalesayyedatfatmaNo ratings yet
- Clinical Biochemistry Diageasy All Health Check-Up: End of ReportDocument11 pagesClinical Biochemistry Diageasy All Health Check-Up: End of ReportHarshitNo ratings yet
- Final Report: ArsenazoDocument2 pagesFinal Report: ArsenazoHarshitNo ratings yet
- Laboratory Investigation Report: Clinical BiochemistryDocument4 pagesLaboratory Investigation Report: Clinical BiochemistryHarshitNo ratings yet
- This Is An Electronically Authorized Prescription, Hence Does Not Require A Signature. Reference Number: MH279307Document1 pageThis Is An Electronically Authorized Prescription, Hence Does Not Require A Signature. Reference Number: MH279307HarshitNo ratings yet
- N1 Soil ReportDocument20 pagesN1 Soil ReportMunjedNo ratings yet
- Test BillDocument6 pagesTest BillWaseem AhmadNo ratings yet
- Curriculum Vitae Kelly WaltersDocument8 pagesCurriculum Vitae Kelly Waltersapi-311907685No ratings yet
- Cell Culture Media - A ReviewDocument29 pagesCell Culture Media - A ReviewFarhana Anuar100% (1)
- The Organic Nature of The StateDocument15 pagesThe Organic Nature of The Statedivyanshu sharmaNo ratings yet
- Microbiology and Parasitology #1Document11 pagesMicrobiology and Parasitology #1Judy BaguiwenNo ratings yet
- Energy Flow in Ecosystems PDFDocument34 pagesEnergy Flow in Ecosystems PDFMARTINA MENIENo ratings yet
- Types of Plant DiseasesDocument14 pagesTypes of Plant DiseasesMuqadas NoorNo ratings yet
- Science - Levels of OrganizationDocument4 pagesScience - Levels of OrganizationAlexNo ratings yet
- Radiation Protection Bushong Study GuideDocument6 pagesRadiation Protection Bushong Study GuideAsha6842100% (1)
- The Biomedical Engineering Handbook: Second EditionDocument13 pagesThe Biomedical Engineering Handbook: Second EditionEng-Mugahed AlmansorNo ratings yet
- Pharm - Common Lab Values For NCLEX Kaplan 2013Document2 pagesPharm - Common Lab Values For NCLEX Kaplan 2013sarahpierre10No ratings yet
- Australian Birdkeeper October-November 2018Document60 pagesAustralian Birdkeeper October-November 2018Gábor Deák100% (1)
- OCR AS-Level Biology June 2023 Mark Scheme 1Document23 pagesOCR AS-Level Biology June 2023 Mark Scheme 1FatimaNo ratings yet
- 211 Mitosis LabDocument5 pages211 Mitosis LabadekNo ratings yet
- Full Download PDF of (Ebook PDF) Conservation Biology by Bradley J. Cardinale All ChapterDocument43 pagesFull Download PDF of (Ebook PDF) Conservation Biology by Bradley J. Cardinale All Chapteryadielnasraa100% (4)
- Jaka Index6 PDFDocument85 pagesJaka Index6 PDFFábio Origuela de LiraNo ratings yet
- Brain Myths ExposedDocument10 pagesBrain Myths ExposedSiva Nesh100% (1)
- Polish - English TaskDocument5 pagesPolish - English TaskdaranNo ratings yet
- DLP-L01.1 - Introduction To Personal DevelopmentDocument2 pagesDLP-L01.1 - Introduction To Personal DevelopmentDenise Nicole T. LopezNo ratings yet
- Bitw ProductdirectoryDocument89 pagesBitw ProductdirectorySHIVANINo ratings yet
- Science: BiologyDocument22 pagesScience: BiologyMike RollideNo ratings yet
- Self and Brain - What Is Self-Related Processing PDFDocument2 pagesSelf and Brain - What Is Self-Related Processing PDFhimkeraditya100% (1)
- Middle AdulthoodDocument27 pagesMiddle AdulthoodgopikaNo ratings yet
- Notes: Huberman Lab Podcast: Episode 1: How Your Nervous System Works & ChangesDocument5 pagesNotes: Huberman Lab Podcast: Episode 1: How Your Nervous System Works & ChangesMihaela CenușeNo ratings yet
- 230 - Respiratory Physiology) External Respiration - Ventilation Perfusion CouplingDocument4 pages230 - Respiratory Physiology) External Respiration - Ventilation Perfusion Couplingyoussef magdyNo ratings yet
- Biology Form4 Chapter9Document8 pagesBiology Form4 Chapter9Wei EnNo ratings yet























































































Download as pdf or txt
You might also like
- Mrs Anar DeviDocument14 pagesMrs Anar DeviM.DNo ratings yet
- Xdue6378 2Document2 pagesXdue6378 2S Abedi50% (2)
- Essentials of Medical Laboratory Practice - Lieseke, Constance L. (SRG)Document564 pagesEssentials of Medical Laboratory Practice - Lieseke, Constance L. (SRG)Kaan Halici89% (36)
- Test Report: Complete Blood Count (CBC)Document3 pagesTest Report: Complete Blood Count (CBC)WSC ALMANo ratings yet
- 1-Dengue IgG & IgM - PO2709736085-377Document12 pages1-Dengue IgG & IgM - PO2709736085-377TV UNITNo ratings yet
- 1-Complete Blood Count - PO1106326185-399Document8 pages1-Complete Blood Count - PO1106326185-399Arup KumarNo ratings yet
- Department of Hematology Test Name Result Unit Bio. Ref. IntervalDocument3 pagesDepartment of Hematology Test Name Result Unit Bio. Ref. Intervalaf dNo ratings yet
- Design and Spatial BehaviorDocument24 pagesDesign and Spatial BehaviorHuiyiChang100% (1)
- Kinesiotape Durante El EmbarazoDocument3 pagesKinesiotape Durante El EmbarazoNostrum Sport100% (2)
- Medical Laboratory Report: Haemoglobin Total Leucocyte Count Total Erythrocyte Count Platelet Count MPV PCT PDWDocument4 pagesMedical Laboratory Report: Haemoglobin Total Leucocyte Count Total Erythrocyte Count Platelet Count MPV PCT PDWdhavalNo ratings yet
- Saniya Fathima (7G28Jy) :::: Patient Age / Sex 26 Y / Female BranchDocument3 pagesSaniya Fathima (7G28Jy) :::: Patient Age / Sex 26 Y / Female BranchShah FaisalNo ratings yet
- Kidney FunctionDocument19 pagesKidney FunctionFarooq Bin MahfoozNo ratings yet
- Medical Laboratory Report: Haemoglobin Total Leucocyte Count Total Erythrocyte Count Platelet Count MPV PCT PDWDocument4 pagesMedical Laboratory Report: Haemoglobin Total Leucocyte Count Total Erythrocyte Count Platelet Count MPV PCT PDWdhavalNo ratings yet
- Report 0bd39992Document8 pagesReport 0bd39992NEETFIXNo ratings yet
- Report 3f90266bDocument18 pagesReport 3f90266bSK TacNo ratings yet
- Ssumangarg@gmail - Com 20220825193722Document13 pagesSsumangarg@gmail - Com 20220825193722Suman GargNo ratings yet
- PRAVEEN Y (ID - 8167522) :::: Patient Age / Sex 32 Y / MaleDocument5 pagesPRAVEEN Y (ID - 8167522) :::: Patient Age / Sex 32 Y / Malepraveen yNo ratings yet
- 1-Senior Citizen Basic Package - PO3248534977-432Document16 pages1-Senior Citizen Basic Package - PO3248534977-432Krishna Nand RaiNo ratings yet
- Department of Hematology Test Name Result Unit Bio. Ref. IntervalDocument3 pagesDepartment of Hematology Test Name Result Unit Bio. Ref. Intervalaf dNo ratings yet
- Report of Mr. RAJA PDFDocument3 pagesReport of Mr. RAJA PDFraja.tyagi2125No ratings yet
- Method: Calculated: Page 1 of 9 07-Sep-2022 08:54 PMDocument10 pagesMethod: Calculated: Page 1 of 9 07-Sep-2022 08:54 PMburela_naveenNo ratings yet
- ReportDocument2 pagesReportIshikaNo ratings yet
- Don't Know Love - 1004584Document14 pagesDon't Know Love - 1004584baapj39No ratings yet
- Haematology: Investigation Observed Value Unit Biological Reference IntervalDocument5 pagesHaematology: Investigation Observed Value Unit Biological Reference Intervalshivanand.n ShivanandNo ratings yet
- LabTest 03jul2023Document5 pagesLabTest 03jul2023jkgupta0003No ratings yet
- Mirza Kayesh Begg - 250274290 - CompleteReportDocument12 pagesMirza Kayesh Begg - 250274290 - CompleteReportSYEDA MYSHA ALINo ratings yet
- Department of Hematology Comprehensive Full Body Checkup Test Name Result Unit Bio. Ref. IntervalDocument11 pagesDepartment of Hematology Comprehensive Full Body Checkup Test Name Result Unit Bio. Ref. IntervalshyamNo ratings yet
- Anjali Khapare - 23071171Document3 pagesAnjali Khapare - 23071171dr.menganeNo ratings yet
- Archana Lab ReportDocument10 pagesArchana Lab Reportprabalsoni125No ratings yet
- Lab ResultDocument7 pagesLab ResultAanshika RaizadaNo ratings yet
- Fully Automated Lab Accurate Reports Reports Verified by PathologistDocument11 pagesFully Automated Lab Accurate Reports Reports Verified by PathologistBathri NathanNo ratings yet
- Test Results Units Biological Reference Range Hematology:::::: Ms. Farha MemonDocument5 pagesTest Results Units Biological Reference Range Hematology:::::: Ms. Farha MemonKM GASTRO CENTERNo ratings yet
- Report 89594e5fDocument10 pagesReport 89594e5fNaresh SrikakolapuNo ratings yet
- 1-Senior Citizen Advanced Package - PO3427386675-856Document18 pages1-Senior Citizen Advanced Package - PO3427386675-856Ravi PrakashNo ratings yet
- Test Reports 2Document2 pagesTest Reports 2Chandrasekhara Reddy TNo ratings yet
- 8000000936: Patient ID 80001350 Sid No Nehru Nagar Branch Mr. Vasanth NDocument3 pages8000000936: Patient ID 80001350 Sid No Nehru Nagar Branch Mr. Vasanth NSudha SaravananNo ratings yet
- Medical Laboratory Report: Haemoglobin Total Leucocyte Count Total Erythrocyte Count Platelet Count MPV PCT PDWDocument4 pagesMedical Laboratory Report: Haemoglobin Total Leucocyte Count Total Erythrocyte Count Platelet Count MPV PCT PDWdhavalNo ratings yet
- Sunita NepalDocument5 pagesSunita NepalPrajay NepalNo ratings yet
- Aman CBCDocument1 pageAman CBCAman RathoreNo ratings yet
- Department of Hematology Test Name Result Unit Bio. Ref. IntervalDocument5 pagesDepartment of Hematology Test Name Result Unit Bio. Ref. IntervalHarishNo ratings yet
- Haematology: Investigation Observed Value Unit Biological Reference IntervalDocument2 pagesHaematology: Investigation Observed Value Unit Biological Reference IntervalVivek RadhakrishnanNo ratings yet
- MR Shashidhar Kulkarni 29 04 2023 02 35 25 PMDocument2 pagesMR Shashidhar Kulkarni 29 04 2023 02 35 25 PMagaymashashi2906No ratings yet
- Report 28340c20Document10 pagesReport 28340c20Rahul ChaudhariNo ratings yet
- Labreportnew - 2023-02-17T141822.094Document8 pagesLabreportnew - 2023-02-17T141822.094pavanimatteguntaNo ratings yet
- BloodDocument18 pagesBloodPriyanshu GuptaNo ratings yet
- Labreportnew - 2023-10-17T102750.286Document2 pagesLabreportnew - 2023-10-17T102750.286sidlab202No ratings yet
- 1-Good Health Premium Package - PO1065281239-651Document19 pages1-Good Health Premium Package - PO1065281239-651Renu ChoudharyNo ratings yet
- Haematology Haematology Haematology HaematologyDocument3 pagesHaematology Haematology Haematology HaematologyGopinandan PandeyNo ratings yet
- Jyoti Singh ReportsDocument5 pagesJyoti Singh ReportsRaghujyotisNo ratings yet
- Department of Hematology Test Name Result Unit Bio. Ref. IntervalDocument6 pagesDepartment of Hematology Test Name Result Unit Bio. Ref. IntervalHarishNo ratings yet
- Haematology: Investigation Observed Value Unit Biological Reference IntervalDocument6 pagesHaematology: Investigation Observed Value Unit Biological Reference IntervalumeshlpsNo ratings yet
- R Selvi:::: Patient Age / Sex 56 Y / Female BranchDocument7 pagesR Selvi:::: Patient Age / Sex 56 Y / Female Branchop nNo ratings yet
- LabReportNew - 2024-03-22T202901.640Document8 pagesLabReportNew - 2024-03-22T202901.640alex taylorNo ratings yet
- Department of Laboratory Sciences: Clinical Biochemistry/ Immuno AsssayDocument3 pagesDepartment of Laboratory Sciences: Clinical Biochemistry/ Immuno AsssayKavyaleen KaurNo ratings yet
- Fully Automated Lab Accurate Reports Reports Verified by PathologistDocument14 pagesFully Automated Lab Accurate Reports Reports Verified by PathologistRavindranatha AnNo ratings yet
- PathkindDocument5 pagesPathkindgovt.job4692No ratings yet
- Hematology: KongamdanaDocument1 pageHematology: KongamdanaShariqNo ratings yet
- Hematology: KongamdanaDocument1 pageHematology: KongamdanaShariqNo ratings yet
- IT217236 Report 1Document2 pagesIT217236 Report 1NamithaNo ratings yet
- Complete Blood Count (CBC) : Department of Haematology and Clinical PathologyDocument2 pagesComplete Blood Count (CBC) : Department of Haematology and Clinical PathologyNamithaNo ratings yet
- SR8188385Document2 pagesSR8188385mohanchowdhury1948No ratings yet
- MrsSANGEETASAHU 45Y FemaleDocument6 pagesMrsSANGEETASAHU 45Y FemalesayyedatfatmaNo ratings yet
- Clinical Biochemistry Diageasy All Health Check-Up: End of ReportDocument11 pagesClinical Biochemistry Diageasy All Health Check-Up: End of ReportHarshitNo ratings yet
- Final Report: ArsenazoDocument2 pagesFinal Report: ArsenazoHarshitNo ratings yet
- Laboratory Investigation Report: Clinical BiochemistryDocument4 pagesLaboratory Investigation Report: Clinical BiochemistryHarshitNo ratings yet
- This Is An Electronically Authorized Prescription, Hence Does Not Require A Signature. Reference Number: MH279307Document1 pageThis Is An Electronically Authorized Prescription, Hence Does Not Require A Signature. Reference Number: MH279307HarshitNo ratings yet
- N1 Soil ReportDocument20 pagesN1 Soil ReportMunjedNo ratings yet
- Test BillDocument6 pagesTest BillWaseem AhmadNo ratings yet
- Curriculum Vitae Kelly WaltersDocument8 pagesCurriculum Vitae Kelly Waltersapi-311907685No ratings yet
- Cell Culture Media - A ReviewDocument29 pagesCell Culture Media - A ReviewFarhana Anuar100% (1)
- The Organic Nature of The StateDocument15 pagesThe Organic Nature of The Statedivyanshu sharmaNo ratings yet
- Microbiology and Parasitology #1Document11 pagesMicrobiology and Parasitology #1Judy BaguiwenNo ratings yet
- Energy Flow in Ecosystems PDFDocument34 pagesEnergy Flow in Ecosystems PDFMARTINA MENIENo ratings yet
- Types of Plant DiseasesDocument14 pagesTypes of Plant DiseasesMuqadas NoorNo ratings yet
- Science - Levels of OrganizationDocument4 pagesScience - Levels of OrganizationAlexNo ratings yet
- Radiation Protection Bushong Study GuideDocument6 pagesRadiation Protection Bushong Study GuideAsha6842100% (1)
- The Biomedical Engineering Handbook: Second EditionDocument13 pagesThe Biomedical Engineering Handbook: Second EditionEng-Mugahed AlmansorNo ratings yet
- Pharm - Common Lab Values For NCLEX Kaplan 2013Document2 pagesPharm - Common Lab Values For NCLEX Kaplan 2013sarahpierre10No ratings yet
- Australian Birdkeeper October-November 2018Document60 pagesAustralian Birdkeeper October-November 2018Gábor Deák100% (1)
- OCR AS-Level Biology June 2023 Mark Scheme 1Document23 pagesOCR AS-Level Biology June 2023 Mark Scheme 1FatimaNo ratings yet
- 211 Mitosis LabDocument5 pages211 Mitosis LabadekNo ratings yet
- Full Download PDF of (Ebook PDF) Conservation Biology by Bradley J. Cardinale All ChapterDocument43 pagesFull Download PDF of (Ebook PDF) Conservation Biology by Bradley J. Cardinale All Chapteryadielnasraa100% (4)
- Jaka Index6 PDFDocument85 pagesJaka Index6 PDFFábio Origuela de LiraNo ratings yet
- Brain Myths ExposedDocument10 pagesBrain Myths ExposedSiva Nesh100% (1)
- Polish - English TaskDocument5 pagesPolish - English TaskdaranNo ratings yet
- DLP-L01.1 - Introduction To Personal DevelopmentDocument2 pagesDLP-L01.1 - Introduction To Personal DevelopmentDenise Nicole T. LopezNo ratings yet
- Bitw ProductdirectoryDocument89 pagesBitw ProductdirectorySHIVANINo ratings yet
- Science: BiologyDocument22 pagesScience: BiologyMike RollideNo ratings yet
- Self and Brain - What Is Self-Related Processing PDFDocument2 pagesSelf and Brain - What Is Self-Related Processing PDFhimkeraditya100% (1)
- Middle AdulthoodDocument27 pagesMiddle AdulthoodgopikaNo ratings yet
- Notes: Huberman Lab Podcast: Episode 1: How Your Nervous System Works & ChangesDocument5 pagesNotes: Huberman Lab Podcast: Episode 1: How Your Nervous System Works & ChangesMihaela CenușeNo ratings yet
- 230 - Respiratory Physiology) External Respiration - Ventilation Perfusion CouplingDocument4 pages230 - Respiratory Physiology) External Respiration - Ventilation Perfusion Couplingyoussef magdyNo ratings yet
- Biology Form4 Chapter9Document8 pagesBiology Form4 Chapter9Wei EnNo ratings yet