Download as pdf or txt
You might also like
- Rhinologic and Sleep Apnea Surgical Techniques 1st Ed 2007 SDocument427 pagesRhinologic and Sleep Apnea Surgical Techniques 1st Ed 2007 SKarolina RamirezNo ratings yet
- Adult Infectious Disease Bulletpoints HandbookFrom EverandAdult Infectious Disease Bulletpoints HandbookRating: 4.5 out of 5 stars4.5/5 (9)
- Pharmacology Chapter 42 p-2Document11 pagesPharmacology Chapter 42 p-2sho bartNo ratings yet
- HubermanDocument2 pagesHubermanMilojko0% (1)
- Anti Viral Drugs: Dr. Yani Mulyani, M.Si, AptDocument47 pagesAnti Viral Drugs: Dr. Yani Mulyani, M.Si, AptYani MulyaniNo ratings yet
- Antiviral Drugs: Ana Khusnul Faizah Farmasi FK Uht 2020Document24 pagesAntiviral Drugs: Ana Khusnul Faizah Farmasi FK Uht 2020Muhammad Iqbal DarmansyahNo ratings yet
- Antiviral p1Document4 pagesAntiviral p1N Gv FcNo ratings yet
- AntiviralDocument14 pagesAntiviralshehranNo ratings yet
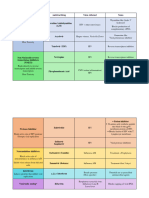
- Antivirals: Drug Clinical Use Drug Type Action Side Effect Drug Interaction Pharmacokinetic S Other DetailsDocument10 pagesAntivirals: Drug Clinical Use Drug Type Action Side Effect Drug Interaction Pharmacokinetic S Other DetailshectorNo ratings yet
- Tatalaksana Hepatitis B Kronik: Nurul Nadifa Erza 1610211084Document18 pagesTatalaksana Hepatitis B Kronik: Nurul Nadifa Erza 1610211084Putri KNo ratings yet
- Antivirals Pharma Activity 08may23Document17 pagesAntivirals Pharma Activity 08may23Adrian CaballesNo ratings yet
- Anti Viral TableDocument8 pagesAnti Viral TablekvmNo ratings yet
- Antiretrovirals: MOA/ Metabolism Patient Considerations SE ResistanceDocument3 pagesAntiretrovirals: MOA/ Metabolism Patient Considerations SE ResistanceshinbiNo ratings yet
- Antiviral Agents: Jillian H. Davis Dept. of Pharmacology March 31, 2004Document63 pagesAntiviral Agents: Jillian H. Davis Dept. of Pharmacology March 31, 2004mishra_nidhiNo ratings yet
- Pharma NotesDocument9 pagesPharma NotesMayya FirdousNo ratings yet
- Antiviral AgentsDocument14 pagesAntiviral AgentsKate MendozaNo ratings yet
- Nrtis: (Nucleoside/ Nucleotide Reverse Transcriptase) : "Eatz LSD"Document3 pagesNrtis: (Nucleoside/ Nucleotide Reverse Transcriptase) : "Eatz LSD"Mohammad KatatoNo ratings yet
- B1M4L2-Anti Viral TherapyDocument8 pagesB1M4L2-Anti Viral TherapyRalph de la TorreNo ratings yet
- Anti Viral DrugsDocument3 pagesAnti Viral Drugsbilal ahmadNo ratings yet
- Antiretroviral Agents 2017Document38 pagesAntiretroviral Agents 2017Iman SaksoukNo ratings yet
- Antiviral Drugs TableDocument16 pagesAntiviral Drugs TableJennifer HerediaNo ratings yet
- Drug Name Mechanism of Action Indication Contraindications Side Effects/Adverse Effects Nursing ConsiderationDocument5 pagesDrug Name Mechanism of Action Indication Contraindications Side Effects/Adverse Effects Nursing ConsiderationWyeth Earl Padar EndrianoNo ratings yet
- AntihepatitisDocument38 pagesAntihepatitismariamanoNo ratings yet
- Slide - K-27 - Farmakologi AntivirusDocument36 pagesSlide - K-27 - Farmakologi AntivirusFaisal AlhasNo ratings yet
- 5 Antiviral1Document34 pages5 Antiviral1Amr KhayyalNo ratings yet
- Antiviral AgentsDocument61 pagesAntiviral AgentsTES SENNo ratings yet
- Antivirals (Katzung)Document6 pagesAntivirals (Katzung)sarguss1467% (3)
- Antiviral DrugsDocument12 pagesAntiviral DrugsRisal DidinNo ratings yet
- Summary of Antiviral DrugsDocument2 pagesSummary of Antiviral DrugsKate Sarah GabasaNo ratings yet
- Antiviral DrugsDocument5 pagesAntiviral DrugsSajid AliNo ratings yet
- Antiviral DrugsDocument12 pagesAntiviral DrugsAmelia RumiNo ratings yet
- Internal Medicine Long Case 5Document7 pagesInternal Medicine Long Case 5RoshilNo ratings yet
- Mechanism Resistance of Antiviral - VeroDocument32 pagesMechanism Resistance of Antiviral - VeroHanung PujanggaNo ratings yet
- Antihsv-Vzv AgentsDocument35 pagesAntihsv-Vzv AgentsAulia Rahma NoviastutiNo ratings yet
- Antiviral DrugsDocument44 pagesAntiviral DrugsMohammed WasimNo ratings yet
- Antiviral DrugsDocument44 pagesAntiviral DrugsMohammed WasimNo ratings yet
- Depart. of Farmacology, Medical Faculty, Moslem University: WisudawanDocument12 pagesDepart. of Farmacology, Medical Faculty, Moslem University: Wisudawansuyudi kimikoNo ratings yet
- Antiviral DrugsDocument2 pagesAntiviral DrugsGuy SebNo ratings yet
- Pcol Antiviral Agents - de La Cruz, M - Gangoso, K..Document101 pagesPcol Antiviral Agents - de La Cruz, M - Gangoso, K..Marienelle De La CruzNo ratings yet
- Metronidazole: Mechanism of Antibacterial Action Is Unclear, But NeedsDocument60 pagesMetronidazole: Mechanism of Antibacterial Action Is Unclear, But NeedsmmydungNo ratings yet
- EtravirineDocument3 pagesEtravirineRosher Deliman JanoyanNo ratings yet
- Presentation: Anti Viral DrugsDocument29 pagesPresentation: Anti Viral DrugsUmama WarrichNo ratings yet
- Antiviral Drugs2Document47 pagesAntiviral Drugs2Kunal JaatNo ratings yet
- ZOOL 143 Topic 8 Management of HIV and AIDS InfectionsDocument18 pagesZOOL 143 Topic 8 Management of HIV and AIDS InfectionsnattydreadfathelahNo ratings yet
- Antivirusni LekoviDocument45 pagesAntivirusni LekoviPavle NastasicNo ratings yet
- Antiviral, Myco DentDocument13 pagesAntiviral, Myco Dentmohsen mirdamadiNo ratings yet
- Farmacologia AntiviraisDocument24 pagesFarmacologia AntiviraisHumberto Santoro CardosoNo ratings yet
- Antiviral DrugsDocument25 pagesAntiviral Drugss.k. kubraNo ratings yet
- 6 Antiviral Drugs PDFDocument68 pages6 Antiviral Drugs PDFIman SaksoukNo ratings yet
- Anti-Viral DrugsDocument53 pagesAnti-Viral DrugsClaudia SunshieNo ratings yet
- Chemotherapy - 2Document90 pagesChemotherapy - 2shNo ratings yet
- Pharmacology Chapter 49 - AntiviralsDocument4 pagesPharmacology Chapter 49 - AntiviralsAlexAnneNo ratings yet
- Common Antiviral-1Document25 pagesCommon Antiviral-1emmanuelmkibuniNo ratings yet
- Human VirusesDocument7 pagesHuman VirusesMakesh RamuNo ratings yet
- HAART ASSIGNMENT. 2docxDocument2 pagesHAART ASSIGNMENT. 2docxssemhbi8943No ratings yet
- Inhibition of Intracellular Synthesis byDocument1 pageInhibition of Intracellular Synthesis byFalaq2No ratings yet
- 9) AntiretroviralDocument79 pages9) AntiretroviralOkot ChristopherNo ratings yet
- Drug Study HRZEDocument4 pagesDrug Study HRZEChristine Gold Apduhan AguilarNo ratings yet
- Pasco AntiviralsDocument2 pagesPasco AntiviralsNicole ObispoNo ratings yet
- RetrovirusDocument5 pagesRetrovirusferdudz schneiderNo ratings yet
- Hepatitis B Virus and Liver DiseaseFrom EverandHepatitis B Virus and Liver DiseaseJia-Horng KaoNo ratings yet
- Biology for Students: The Only Biology Study Guide You'll Ever Need to Ace Your CourseFrom EverandBiology for Students: The Only Biology Study Guide You'll Ever Need to Ace Your CourseNo ratings yet
- Biochemical Energy Production: Type I Multiple-Choice QuestionsDocument12 pagesBiochemical Energy Production: Type I Multiple-Choice QuestionsKevin Dacatimbang100% (1)
- Pathophysiology of HypertensionDocument11 pagesPathophysiology of HypertensionThenmozhi SureshNo ratings yet
- Kamus AnatomiDocument42 pagesKamus AnatomiAbdul Al-hadiNo ratings yet
- Secretion From The Pineal GlandDocument8 pagesSecretion From The Pineal GlandVince Laurence BlancaflorNo ratings yet
- Essentials of Oral Histology and Embryology. James Avery, 2 EditionDocument29 pagesEssentials of Oral Histology and Embryology. James Avery, 2 EditionAde Dian KaruniaNo ratings yet
- 1 - Back PPT AauDocument44 pages1 - Back PPT Aauahmed mohammedNo ratings yet
- Lesson 7 - Nervous, Endocrine, Reproductive, Urinary SystemDocument37 pagesLesson 7 - Nervous, Endocrine, Reproductive, Urinary SystemAlejandro GuerreroNo ratings yet
- ChickenDocument9 pagesChickenJefferson TanNo ratings yet
- Advanced Practicetest 7Document8 pagesAdvanced Practicetest 7phươngNo ratings yet
- Summative 7Document4 pagesSummative 7SPEILBERG LUMBAYNo ratings yet
- Modification of ProteinsDocument39 pagesModification of ProteinsAmit Kr GodaraNo ratings yet
- Phys 2S12 General Senses 1Document9 pagesPhys 2S12 General Senses 1adnilsallyNo ratings yet
- The Role of Himsradya Taila Nasya in Primary HypothyroidismDocument4 pagesThe Role of Himsradya Taila Nasya in Primary HypothyroidismResearch ParkNo ratings yet
- Hustle CultureDocument1 pageHustle CultureAnirudh Kar 1912705No ratings yet
- Link Download Ebook Anatomy and PhysiologyDocument87 pagesLink Download Ebook Anatomy and Physiologyarif100% (1)
- In2Med HaematologyDocument30 pagesIn2Med Haematologye148659No ratings yet
- 6.6 Hormones & HomeostasisDocument1 page6.6 Hormones & HomeostasisNaomi BoesonoNo ratings yet
- AUBF Amniotic FluidDocument6 pagesAUBF Amniotic FluidRichelyn Grace B. VenusNo ratings yet
- HemoglobinDocument33 pagesHemoglobinAkash JaatNo ratings yet
- Description of Reproductive System of Indian Water Scorpion, Laccotrephes Maculatus Fabr. (Hemiptera, Heteroptera: Nepidae)Document13 pagesDescription of Reproductive System of Indian Water Scorpion, Laccotrephes Maculatus Fabr. (Hemiptera, Heteroptera: Nepidae)Kanhiya MahourNo ratings yet
- Practice TESTS NephrologyDocument56 pagesPractice TESTS NephrologyFabiola AlonsoNo ratings yet
- Unit Organogenesis of Eye And: StructureDocument40 pagesUnit Organogenesis of Eye And: Structurekaladhar reddyNo ratings yet
- Ali, Benkhalifa, Miron 2006 - In-Vitro Maturation of Oocytes Biological AspectsDocument10 pagesAli, Benkhalifa, Miron 2006 - In-Vitro Maturation of Oocytes Biological AspectsRimas Prathita AgustinNo ratings yet
- A - Glucagon: Abdulmajeed Rabe3Document56 pagesA - Glucagon: Abdulmajeed Rabe3MONFOLANo ratings yet
- Pex 09 03Document4 pagesPex 09 03Marcela Anco Sotomayor50% (4)
- Mechanisms of Hemostasis - Contributions of Platelets, Coagulation Factors, and The Vessel WallDocument25 pagesMechanisms of Hemostasis - Contributions of Platelets, Coagulation Factors, and The Vessel WallelhierofanteNo ratings yet
- B-Cell DevelopmentDocument85 pagesB-Cell Developmentعلي عايد عبدالشهيدNo ratings yet