Download as pdf or txt
You might also like
- Change On The Rise: Transcribed by David LiuDocument7 pagesChange On The Rise: Transcribed by David Liuveromejhdo57% (7)
- Rubber Burn Test SpecsDocument1 pageRubber Burn Test SpecsTushar BagdeNo ratings yet
- An Introduction To Neonatal EEGDocument8 pagesAn Introduction To Neonatal EEGfilzahnur joharNo ratings yet
- 01 ElectroencephalographyDocument3 pages01 ElectroencephalographyAdrianFrateaNo ratings yet
- EEG and Epilepsy Monitoring.10Document25 pagesEEG and Epilepsy Monitoring.10mhd.mamdohNo ratings yet
- Electroencephalography in Pediatric EpilepsyDocument12 pagesElectroencephalography in Pediatric EpilepsyPrankur PandeyNo ratings yet
- (Electroencephalogra M) : Intro. To Biomedical Engineering Presentation #1 - EegDocument21 pages(Electroencephalogra M) : Intro. To Biomedical Engineering Presentation #1 - EegArif IzzatNo ratings yet
- Wavelet Preprocessing For Automated Neural Network Detection of EEG SpikesDocument7 pagesWavelet Preprocessing For Automated Neural Network Detection of EEG SpikesSantiago Flores AlonsoNo ratings yet
- Project Report On EEG MachineDocument26 pagesProject Report On EEG Machineneetubansal60% (5)
- Crisis en Eega de Vrie 2019Document38 pagesCrisis en Eega de Vrie 2019Jimmy Pino CoricazaNo ratings yet
- Kuperberg - Electroencephalography. Capitulo 6 PersDocument12 pagesKuperberg - Electroencephalography. Capitulo 6 PersAlejandra GaonaNo ratings yet
- Clinical-Neurophysiology 2016 MedicineDocument5 pagesClinical-Neurophysiology 2016 MedicinemateoNo ratings yet
- Expert Systems With Applications: Semih Altunay, Ziya Telatar, Osman ErogulDocument5 pagesExpert Systems With Applications: Semih Altunay, Ziya Telatar, Osman ErogulViswanath ReddyNo ratings yet
- EEG Signal Analysis A SurveyDocument18 pagesEEG Signal Analysis A Surveybhavesh mishraNo ratings yet
- Electroencephalography: Source of EEG ActivityDocument16 pagesElectroencephalography: Source of EEG ActivityJames LevyNo ratings yet
- Quantitative Electroencephalography QEEG - 04052010Document15 pagesQuantitative Electroencephalography QEEG - 04052010Ngô Tuấn HưngNo ratings yet
- Amplitude-Integrated EEG Classification and InterpDocument15 pagesAmplitude-Integrated EEG Classification and InterpAhalia NicuNo ratings yet
- EEG - Dynamics - Sevo - Children - Br. J. Anaesth.-2015-Akeju-i66-76Document11 pagesEEG - Dynamics - Sevo - Children - Br. J. Anaesth.-2015-Akeju-i66-76MIRELA MIHALACHINo ratings yet
- ElectroencephalographyDocument17 pagesElectroencephalographysambadeeNo ratings yet
- Role of Cerebral Function Monitoring in The NewbornDocument7 pagesRole of Cerebral Function Monitoring in The NewbornFer45No ratings yet
- EegDocument16 pagesEegAhmed Al-helfiNo ratings yet
- Electroencephalography (Eeg)Document13 pagesElectroencephalography (Eeg)Shelten GeorgeNo ratings yet
- Neurophysiological Recordings Improve The Accuracy of 2022 European JournalDocument6 pagesNeurophysiological Recordings Improve The Accuracy of 2022 European Journalcsepulveda10No ratings yet
- Electroencephalography: Source of EEG ActivityDocument16 pagesElectroencephalography: Source of EEG ActivityEmonNo ratings yet
- EEG Signal Analysis: A Survey: Original PaperDocument18 pagesEEG Signal Analysis: A Survey: Original PaperRajesh KandalaNo ratings yet
- Review of Significant Research On EEG Based Automated Detection of Epilepsy Seizures Brain TumorDocument9 pagesReview of Significant Research On EEG Based Automated Detection of Epilepsy Seizures Brain TumorSachin GuptaNo ratings yet
- Practicals NeurophysiologyDocument36 pagesPracticals NeurophysiologysridharNo ratings yet
- I Spine Best Neurodiagnostics in Houston KeywordsDocument2 pagesI Spine Best Neurodiagnostics in Houston Keywordsdeepak kumarNo ratings yet
- Analysis of Epilepsy Using Approximate Entropy AlgorithmDocument5 pagesAnalysis of Epilepsy Using Approximate Entropy Algorithmanon_287269697No ratings yet
- Paper 6Document7 pagesPaper 6Sweena MaryNo ratings yet
- Accepted Manuscript: Computers in Biology and MedicineDocument25 pagesAccepted Manuscript: Computers in Biology and MedicineDhanalekshmi YedurkarNo ratings yet
- Eeg For Pediatric ResidentsDocument45 pagesEeg For Pediatric ResidentsChindia Bunga100% (1)
- Electroencephalography (EEG) in The Diagnosis of Seizures and Epilepsy - UpToDate PDFDocument37 pagesElectroencephalography (EEG) in The Diagnosis of Seizures and Epilepsy - UpToDate PDFRobert MîndreanuNo ratings yet
- EEG in Dementia and EncephalopathyDocument19 pagesEEG in Dementia and EncephalopathyDumitruAuraNo ratings yet
- NF Basics R. Thatcher, J. LubarDocument38 pagesNF Basics R. Thatcher, J. Lubarvictoria castroNo ratings yet
- Using Aeeg Di NeonatalDocument9 pagesUsing Aeeg Di NeonatalannaNo ratings yet
- 1 s2.0 S0165027002003400 MainDocument19 pages1 s2.0 S0165027002003400 MainVaNo ratings yet
- Early Detection of Epilepsy Using EEG Signals: Selvin Pradeep Kumar.S Ajitha.LDocument6 pagesEarly Detection of Epilepsy Using EEG Signals: Selvin Pradeep Kumar.S Ajitha.LPRIYANKANo ratings yet
- Jurnal EEGDocument17 pagesJurnal EEGNurul FajriNo ratings yet
- Neurophysiology of Juvenile Myoclonic EpilepsyDocument10 pagesNeurophysiology of Juvenile Myoclonic EpilepsyDiana Marcela Cornejo SanchezNo ratings yet
- Neurofeedback Treatment For EpilepsyDocument11 pagesNeurofeedback Treatment For EpilepsyFelix NogueiraNo ratings yet
- Brain Mapping 6-1225032385340935-8Document5 pagesBrain Mapping 6-1225032385340935-8skyclad_21No ratings yet
- Visualization of EEG Data To Detect ADHD in Children and AdultsDocument5 pagesVisualization of EEG Data To Detect ADHD in Children and AdultsInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- (6-12) A Novel Approach For EEGDocument7 pages(6-12) A Novel Approach For EEGHema KumbharNo ratings yet
- EEG Microstate Complexity For Aiding Early Diagnosis of Alzheimer's DiseaseDocument10 pagesEEG Microstate Complexity For Aiding Early Diagnosis of Alzheimer's DiseaseGabriel Souza SuzartNo ratings yet
- Epilepsy q5Document48 pagesEpilepsy q5Christopher AdhisasmitaNo ratings yet
- EEGSurveyDocument19 pagesEEGSurveyGeo MeNo ratings yet
- Approaches To Staging Sleep in Polysomnographic Studies With Epileptic Activity 2003Document9 pagesApproaches To Staging Sleep in Polysomnographic Studies With Epileptic Activity 2003Bruna PinheirosNo ratings yet
- Automated Classification of Eeg Signals Using DTCWT and Ann ClassifierDocument6 pagesAutomated Classification of Eeg Signals Using DTCWT and Ann ClassifierLJANo ratings yet
- EEG StressDocument16 pagesEEG StressRavi ChanderNo ratings yet
- Ref 5Document15 pagesRef 5Neha BhatiNo ratings yet
- WOS - Neurodevelopment in Newborns A Sample Entropy Analysis of ElectroencephalogramDocument15 pagesWOS - Neurodevelopment in Newborns A Sample Entropy Analysis of Electroencephalogramanto.fernandez0107No ratings yet
- 10.1016@B978 0 444 64032 1.00009 6Document18 pages10.1016@B978 0 444 64032 1.00009 6ilonaskorinNo ratings yet
- A Novel Signal Modeling Approach For Classification of Seizure and Seizure-Free EEG SignalsDocument10 pagesA Novel Signal Modeling Approach For Classification of Seizure and Seizure-Free EEG SignalsDhanalekshmi YedurkarNo ratings yet
- Fundamental of EEG MeasurementDocument12 pagesFundamental of EEG MeasurementRyna Aulia Falamy100% (1)
- Electroencephalography (EEG) in The Diagnosis of Seizures and Epilepsy - UpToDateDocument41 pagesElectroencephalography (EEG) in The Diagnosis of Seizures and Epilepsy - UpToDateAndres Rojas JerezNo ratings yet
- Compressive Wideband Power Spectrum Analysis For Eeg Signals Using Fastica and Neural NetworkDocument7 pagesCompressive Wideband Power Spectrum Analysis For Eeg Signals Using Fastica and Neural NetworkInternational Organization of Scientific Research (IOSR)No ratings yet
- Clinical Neurophysiology and Electroencephalography: Jong Woo Lee, MD, PHD, and Shahram Khoshbin, MDDocument9 pagesClinical Neurophysiology and Electroencephalography: Jong Woo Lee, MD, PHD, and Shahram Khoshbin, MDEmilio SanchezNo ratings yet
- Electronic Brain Wave MachineDocument13 pagesElectronic Brain Wave MachineRudransh NaredaNo ratings yet
- Acharya 2012Document8 pagesAcharya 2012Dhanalekshmi YedurkarNo ratings yet
- Aftab - NeuroDocument17 pagesAftab - NeuroAkmal SharafNo ratings yet
- Neurofeedback - The Neurofeedback Book for Patients and Therapists : A Symphony of the MindFrom EverandNeurofeedback - The Neurofeedback Book for Patients and Therapists : A Symphony of the MindNo ratings yet
- TheDocument12 pagesTheVictor PileggiNo ratings yet
- Stalking & Dreaming PDFDocument4 pagesStalking & Dreaming PDFJoannaAllen100% (2)
- Wee1964 N001Document9 pagesWee1964 N001Oliver RubioNo ratings yet
- Microcontroller Based Speech To Text Translation SystemDocument6 pagesMicrocontroller Based Speech To Text Translation SystemJay Prakash MandalNo ratings yet
- Sonia Thakker 184 Jignesh Bhatt 105 Rekha Wachkawde 188 Shailendra Singh 178 Pravin Nayak 147 Jibu James 128Document44 pagesSonia Thakker 184 Jignesh Bhatt 105 Rekha Wachkawde 188 Shailendra Singh 178 Pravin Nayak 147 Jibu James 128treakoNo ratings yet
- 561566642977unit-3 - TextilesDocument11 pages561566642977unit-3 - TextilesGaganpreet Kaur Fashion DesigningNo ratings yet
- Lab ManualDocument41 pagesLab Manualprojectapply2023No ratings yet
- M20 LatticeDocument30 pagesM20 LatticeKerwin Cley UgaleNo ratings yet
- The Talmud of Jerusalem - Schwab Moise 1839-1918 TRDocument201 pagesThe Talmud of Jerusalem - Schwab Moise 1839-1918 TRJanice O'BrianNo ratings yet
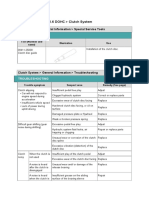
- 06.clutch SystemDocument24 pages06.clutch SystemTony D'AngeloNo ratings yet
- Scapula Setting AnaIsabel AlmeidaDocument1 pageScapula Setting AnaIsabel AlmeidaPeter ZachNo ratings yet
- Uops Parex Modeling Simulation and OptimizationDocument11 pagesUops Parex Modeling Simulation and OptimizationMaissa. ffNo ratings yet
- Laws of Malaysia: Factories and Machinery Act 1967 (Act 139)Document3 pagesLaws of Malaysia: Factories and Machinery Act 1967 (Act 139)daveleyconsNo ratings yet
- SyllogismDocument25 pagesSyllogismSunil GahlotNo ratings yet
- Exhaust Gas Recirculation (EGR)Document18 pagesExhaust Gas Recirculation (EGR)Srinath Pai100% (1)
- Drop Tower MQP Final ReportDocument70 pagesDrop Tower MQP Final ReportFABIAN FIENGONo ratings yet
- Samsung Galaxy S22 Ultra 5G - Full Phone SpecificationsDocument13 pagesSamsung Galaxy S22 Ultra 5G - Full Phone SpecificationsAb BossNo ratings yet
- Metabolizam SeceraDocument52 pagesMetabolizam SeceraAnel RedzepiNo ratings yet
- DIAGRAMA - 2007 - NEW YarisDocument1 pageDIAGRAMA - 2007 - NEW YarisLuis M. Valenzuela Arias50% (2)
- Sub Pekerjaan: D.Pekerjaan Mekanikal & Elektrikal: A Pekerjaan Panel, Trafo, Dan GensetDocument15 pagesSub Pekerjaan: D.Pekerjaan Mekanikal & Elektrikal: A Pekerjaan Panel, Trafo, Dan Gensetberkah shokaNo ratings yet
- Drug Information and Poison InformationDocument6 pagesDrug Information and Poison Informationsri deepika sri deepikaNo ratings yet
- Ap One Pagers Combined PDFDocument10 pagesAp One Pagers Combined PDFJack KirbyNo ratings yet
- Total Result 2594 Total Result 2583Document2,897 pagesTotal Result 2594 Total Result 2583anjali shilpa kajalNo ratings yet
- Tools and Service Items: A/C Can TapsDocument15 pagesTools and Service Items: A/C Can Tapshome businessNo ratings yet
- Module 2 (People and The Earth's Ecosystem)Document11 pagesModule 2 (People and The Earth's Ecosystem)chris ian0% (2)
- 2006 Philippines Road ClassificationDocument44 pages2006 Philippines Road ClassificationpetiepanNo ratings yet
- Introduction To GlobalizationDocument6 pagesIntroduction To GlobalizationJeselica Anne Marie CastroNo ratings yet
- The Occidental Man in Search of Human ValuesDocument11 pagesThe Occidental Man in Search of Human ValuesBen Ritche LayosNo ratings yet