Download as docx, pdf, or txt
You might also like
- A330 ManualDocument642 pagesA330 ManualMcNo ratings yet
- Tarlacstateuniversity College of Science Nursing DepartmentDocument5 pagesTarlacstateuniversity College of Science Nursing DepartmentBethrice MelegritoNo ratings yet
- Checklist - Nursing ProceduresDocument53 pagesChecklist - Nursing ProceduresAbigail Mangaoang100% (4)
- Situation 1Document18 pagesSituation 1Maler De VeraNo ratings yet
- Philippine Water Supply Sector Roadmap 2nd EditionDocument91 pagesPhilippine Water Supply Sector Roadmap 2nd EditionjohnllenalcantaraNo ratings yet
- v723 6986675 SM 4-10 (Full Permission) - UnprotectedDocument913 pagesv723 6986675 SM 4-10 (Full Permission) - UnprotectedAaron VanceNo ratings yet
- Care and Dressing of Wound PERFORMANCE CHECKLISTDocument2 pagesCare and Dressing of Wound PERFORMANCE CHECKLISTKathrina Mendoza HembradorNo ratings yet
- Gloving ChecklistDocument1 pageGloving Checklistromanamercadero314No ratings yet
- REVISED OB Pack ChecklistDocument4 pagesREVISED OB Pack Checklistsheam albaNo ratings yet
- Tracheostomy CareDocument3 pagesTracheostomy CareangelaclaireramosNo ratings yet
- Scrubbing Gloving ChecklistDocument3 pagesScrubbing Gloving ChecklistLea CelestialNo ratings yet
- Handwashing ChecklistDocument1 pageHandwashing ChecklistRichard PidlaoanNo ratings yet
- Procedure Checklist With Rating Form Donning and Removing Sterile GlovesDocument4 pagesProcedure Checklist With Rating Form Donning and Removing Sterile GlovesRachel VillanuevaNo ratings yet
- GlovingDocument2 pagesGlovingAngelica AmandoNo ratings yet
- NCM 102 Basic Nursing ProceduresDocument50 pagesNCM 102 Basic Nursing Proceduresjohn datu100% (1)
- Donning and Removing Sterile Gloves (Open Method)Document2 pagesDonning and Removing Sterile Gloves (Open Method)Ej Mae FabiNo ratings yet
- HandwashingGloving PositioningDocument6 pagesHandwashingGloving PositioningFiona Marie PelaezNo ratings yet
- Care Dressing WoundsDocument2 pagesCare Dressing WoundsJan Erika AlmeronNo ratings yet
- Surgical Handwashing Gowning and Gloving ChecklistDocument6 pagesSurgical Handwashing Gowning and Gloving ChecklistMichelle Dona MirallesNo ratings yet
- Handwashing ChecklistDocument4 pagesHandwashing ChecklistAldrin SabayNo ratings yet
- Gloving Open MethodDocument2 pagesGloving Open Methodguerrerolejan1No ratings yet
- Performance Checklist Bag Technique: VisionDocument3 pagesPerformance Checklist Bag Technique: VisionPrincess ZantuaNo ratings yet
- Performance Evaluation Tool Colostomy Care 1Document2 pagesPerformance Evaluation Tool Colostomy Care 1Pamela LarraquelNo ratings yet
- Gloving ChecklistDocument2 pagesGloving ChecklistlemuelNo ratings yet
- Colostomy CareDocument1 pageColostomy CareGrace Dianne MendozaNo ratings yet
- E Tool Bag TechniqueDocument2 pagesE Tool Bag TechniqueMaurice Ann MarquezNo ratings yet
- Perineal Genital Care PERFORMANCE-CHECKLISTDocument2 pagesPerineal Genital Care PERFORMANCE-CHECKLISTMary joy PaaNo ratings yet
- Bag Technique ToolDocument1 pageBag Technique ToolAriel Delos ReyesNo ratings yet
- Gloving Open EtoolDocument1 pageGloving Open EtoolArah UntalanNo ratings yet
- NCM 109 ChecklistDocument22 pagesNCM 109 ChecklistNYZHEL DEL VALLENo ratings yet
- Procedure Performed Independently Performed With Assistance Unable TO Perfor M Remarks 4-5 2-3 0-1 AssessmentDocument3 pagesProcedure Performed Independently Performed With Assistance Unable TO Perfor M Remarks 4-5 2-3 0-1 AssessmentMelchizeder Solis LumanogNo ratings yet
- BAG TECHNIQUE CHECKLIST CompressedDocument1 pageBAG TECHNIQUE CHECKLIST CompressedRuel John RanayNo ratings yet
- State Purposes of Gloving. Assemble Necessary Materials For Gloving. Perform Medical Hand WashingDocument2 pagesState Purposes of Gloving. Assemble Necessary Materials For Gloving. Perform Medical Hand WashingSean Philippe CabralNo ratings yet
- Level 2Document52 pagesLevel 2Kia MadineNo ratings yet
- Donning and Removing Personal Protective EquipmentDocument2 pagesDonning and Removing Personal Protective EquipmentEj Mae FabiNo ratings yet
- BSN 1 Procedure ChecklistDocument25 pagesBSN 1 Procedure ChecklistSteve EstebanNo ratings yet
- Checklist Wound CareDocument2 pagesChecklist Wound CareKath NambuNo ratings yet
- 5 Assist in Gowning and GlovingDocument2 pages5 Assist in Gowning and GlovingFitzLucario QueNo ratings yet
- Nursing Aid Training Program.Document23 pagesNursing Aid Training Program.BeyangaStephenNo ratings yet
- Chapter 9 Sterile TechniqueDocument8 pagesChapter 9 Sterile TechniqueNila ManguerraNo ratings yet
- Gowning and GlovingDocument1 pageGowning and Glovingcataleya mesaNo ratings yet
- NCM 122 Procedural ChecklistDocument39 pagesNCM 122 Procedural ChecklistLorenz Jude CańeteNo ratings yet
- BCG EtoolDocument1 pageBCG EtoolAriel Delos ReyesNo ratings yet
- Checklist Opthalmic MedDocument3 pagesChecklist Opthalmic MedamaNo ratings yet
- FBS Quarter 1 Module 3Document30 pagesFBS Quarter 1 Module 3Maymay AuauNo ratings yet
- Oro-Nasopharyngeal Suctioning ChecklistDocument7 pagesOro-Nasopharyngeal Suctioning ChecklistAL HAMIER DAUD DAGANIONo ratings yet
- C - IntradermalDocument3 pagesC - IntradermalLyons SchimttNo ratings yet
- Quarter 4 Week 6 Day 1 4Document12 pagesQuarter 4 Week 6 Day 1 4kateNo ratings yet
- Bag Technique & UA Procedure Checklist (Revised)Document1 pageBag Technique & UA Procedure Checklist (Revised)isa masiasNo ratings yet
- JP Drain Hemovac CHECKLISTDocument6 pagesJP Drain Hemovac CHECKLISTxaestalloNo ratings yet
- NCM 103B Performance ChecklistsWITHratingDocument19 pagesNCM 103B Performance ChecklistsWITHratingVINCE KHALID ASARAL ABDULLAHNo ratings yet
- Nbs - Checklist AutosavedDocument2 pagesNbs - Checklist Autosavedtanya merdeNo ratings yet
- Checklist For Bag TechniqueDocument2 pagesChecklist For Bag TechniqueEllyna UssielNo ratings yet
- Checklists NewDocument53 pagesChecklists Newashu pandeyNo ratings yet
- Funda Rle Retdem ProceduresDocument9 pagesFunda Rle Retdem Proceduresaceh lorttNo ratings yet
- PA 4 Neurological Assessment e ToolDocument3 pagesPA 4 Neurological Assessment e ToolMikylla OrdanielNo ratings yet
- Bag Technique and Urine TestingDocument2 pagesBag Technique and Urine TestingKyedae ShymkoNo ratings yet
- PRS InjectionsDocument3 pagesPRS InjectionsLuke SmithNo ratings yet
- Technology and Livelihood Education (Tle) : Learner's Activity Sheet Assessment ChecklistDocument8 pagesTechnology and Livelihood Education (Tle) : Learner's Activity Sheet Assessment ChecklistJohaima HaronNo ratings yet
- HG Assessment Tools JhsDocument6 pagesHG Assessment Tools JhsANA CELLA MARZONo ratings yet
- Perineal Prep Before Vaginal DeliveryDocument1 pagePerineal Prep Before Vaginal DeliveryMva AgueroNo ratings yet
- Checklist For Motuth Neck and EyesDocument7 pagesChecklist For Motuth Neck and EyesWylyn Mae VisqueraNo ratings yet
- Rle Journal Nursing 2024Document11 pagesRle Journal Nursing 2024revillachristinekylaNo ratings yet
- War and Violence in BuddhismDocument3 pagesWar and Violence in BuddhismSean HolarNo ratings yet
- Lab Experiment-SalivaDocument1 pageLab Experiment-SalivaSean HolarNo ratings yet
- Anatomy and PhysiologyDocument5 pagesAnatomy and PhysiologySean HolarNo ratings yet
- ACTIVITIESDocument1 pageACTIVITIESSean HolarNo ratings yet
- Ethics MedtechDocument1 pageEthics MedtechSean HolarNo ratings yet
- Biostatistics and EpidiomologyDocument2 pagesBiostatistics and EpidiomologySean HolarNo ratings yet
- Activity Task D Y S Defend Your StandDocument1 pageActivity Task D Y S Defend Your StandSean HolarNo ratings yet
- Activity Practice Task AnswerDocument1 pageActivity Practice Task AnswerSean HolarNo ratings yet
- Activity 1Document1 pageActivity 1Sean Holar100% (1)
- Positioning and Draping ChecklistDocument5 pagesPositioning and Draping ChecklistSean HolarNo ratings yet
- Informed ConsentDocument11 pagesInformed ConsentSean HolarNo ratings yet
- The HumanDocument10 pagesThe HumanSean HolarNo ratings yet
- Communication TechniquesDocument80 pagesCommunication TechniquesSean HolarNo ratings yet
- Production and Sensory Acceptability of Carrot CookieDocument17 pagesProduction and Sensory Acceptability of Carrot CookieGeraldine ChavezNo ratings yet
- Actuaries CodeDocument4 pagesActuaries CodeShizukaNo ratings yet
- Outline PDF 06052024Document14 pagesOutline PDF 06052024Ryu SenaNo ratings yet
- Field Study 1 Episode 5Document8 pagesField Study 1 Episode 5Fredie RamosNo ratings yet
- PROTEIN SynthesisDocument37 pagesPROTEIN SynthesisChirag KothariNo ratings yet
- Isolation in Endodontics 1kr997b - 2Document9 pagesIsolation in Endodontics 1kr997b - 2Black Hack HakerNo ratings yet
- Omoung LassiDocument3 pagesOmoung LassiWaqas MehmoodNo ratings yet
- Tecson vs. SSSDocument4 pagesTecson vs. SSSFrance De LunaNo ratings yet
- Section: Section:: Student's Information Student's InformationDocument1 pageSection: Section:: Student's Information Student's InformationMello Jane Garcia DedosinNo ratings yet
- Alcohol Addiction TreatmentDocument12 pagesAlcohol Addiction Treatmentkuna2750% (2)
- The Robin Hood Robber: You Witness A Man Rob A Bank, But Instead of Keeping The Money ForDocument4 pagesThe Robin Hood Robber: You Witness A Man Rob A Bank, But Instead of Keeping The Money ForMiguelNo ratings yet
- Intro PaperDocument6 pagesIntro PaperbonnmengulloNo ratings yet
- Emulsions Concept PosterDocument1 pageEmulsions Concept PosterAllison Hoang ThiNo ratings yet
- Fact Sheet On The Safety of Levonorgestrel-Alone Emergency Contraceptive PillsDocument3 pagesFact Sheet On The Safety of Levonorgestrel-Alone Emergency Contraceptive PillsRH Reality CheckNo ratings yet
- 4 B Epbp Cat Technical Details 2017 PreviewDocument546 pages4 B Epbp Cat Technical Details 2017 Previewphotosynergy technologyNo ratings yet
- Tomatoes Tamed Again With CRISPR: Gene Editing Opens The Way To Healthier Crops, FindsDocument1 pageTomatoes Tamed Again With CRISPR: Gene Editing Opens The Way To Healthier Crops, FindsHan YiNo ratings yet
- HavmoreDocument11 pagesHavmorebhhhhNo ratings yet
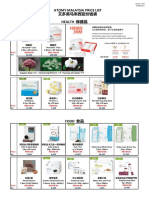
- Atomy Malaysia Price List 艾多美马来西亚价钱表 Health 保健品Document6 pagesAtomy Malaysia Price List 艾多美马来西亚价钱表 Health 保健品Lee Ling PengNo ratings yet
- Casestudy LacticacidfermentationDocument4 pagesCasestudy Lacticacidfermentationapi-3400035320% (1)
- CASE Ferozsons Laboratories LimitedDocument8 pagesCASE Ferozsons Laboratories LimitedOcmi NidiaNo ratings yet
- A Glimpse To A Human Person: Who Am I?: Front PageDocument17 pagesA Glimpse To A Human Person: Who Am I?: Front PageGabrielle May LacsamanaNo ratings yet
- Grout Volume CalculationDocument3 pagesGrout Volume CalculationGEOLOGICS100% (1)
- Exploring The Design Preferences of Neurodivergent Populations For Quiet Spaces - Toar SadiaDocument106 pagesExploring The Design Preferences of Neurodivergent Populations For Quiet Spaces - Toar SadiaLAM POOI WAI / UPMNo ratings yet
- CBSE Schools and KV Class VII SA I Science Model Question Paper 2015Document4 pagesCBSE Schools and KV Class VII SA I Science Model Question Paper 2015Amrita SenNo ratings yet
- 1 PBDocument8 pages1 PBDewi SartikaNo ratings yet
- IGNOU MCA AssignmentDocument12 pagesIGNOU MCA AssignmentafifaNo ratings yet