Download as pdf or txt
You might also like
- USMLE Step 3 Lecture Notes 2021-2022: Internal Medicine, Psychiatry, EthicsFrom EverandUSMLE Step 3 Lecture Notes 2021-2022: Internal Medicine, Psychiatry, EthicsRating: 5 out of 5 stars5/5 (9)
- Filipio Culture Values Practices 1Document30 pagesFilipio Culture Values Practices 1yumiNo ratings yet
- Tsonga PeopleDocument5 pagesTsonga Peopletinyiko100% (2)
- 88 - Indian Nutraceutical Market Opportunities - Report - LRDocument44 pages88 - Indian Nutraceutical Market Opportunities - Report - LRdhananjayNo ratings yet
- 0221 Community-Acquired-PneumoniaDocument29 pages0221 Community-Acquired-PneumoniaDiego YanezNo ratings yet
- Convalescent Plasma Therapy in Patients With COVID-19: ConcisereviewDocument7 pagesConvalescent Plasma Therapy in Patients With COVID-19: ConcisereviewendaNo ratings yet
- Neumonia IDocument9 pagesNeumonia IMario RomoNo ratings yet
- Optimizingdiagnosisand Managementofcommunity-Acquiredpneumoniainthe EmergencydepartmentDocument17 pagesOptimizingdiagnosisand Managementofcommunity-Acquiredpneumoniainthe Emergencydepartmentهادي تركي شنبارةNo ratings yet
- Culture Negative SepsisDocument5 pagesCulture Negative SepsismalvindersahiNo ratings yet
- Cervical Colposcopy: Indications and Risk Assessment: Three RecentDocument12 pagesCervical Colposcopy: Indications and Risk Assessment: Three RecentNajla MasturaNo ratings yet
- 625-Article Text-3497-1-10-20200207Document6 pages625-Article Text-3497-1-10-20200207zeyla.riveros.29No ratings yet
- Case Studies of Lower Respiratory Tract InfectionsDocument25 pagesCase Studies of Lower Respiratory Tract InfectionsMarianNo ratings yet
- Predictors of Mortality in Hospitalised Patients With COVID-19: A 1-Year Case-Control StudyDocument12 pagesPredictors of Mortality in Hospitalised Patients With COVID-19: A 1-Year Case-Control Studystardust.m002No ratings yet
- Risk Estimates Supporting The 2019 ASCCP Risk-Based Management Consensus GuidelinesDocument12 pagesRisk Estimates Supporting The 2019 ASCCP Risk-Based Management Consensus GuidelinesJennyNo ratings yet
- Latifi Navid2018Document13 pagesLatifi Navid2018HolaNo ratings yet
- Nejmoa 2019014Document12 pagesNejmoa 2019014Samuel SebastianNo ratings yet
- Incidence and Risk Factors For Ventilator Associated Pneumon 2007 RespiratorDocument6 pagesIncidence and Risk Factors For Ventilator Associated Pneumon 2007 RespiratorTomasNo ratings yet
- BIMA Oxford AZ Vaccine Detailed Position StatementDocument5 pagesBIMA Oxford AZ Vaccine Detailed Position StatementVegha NedyaNo ratings yet
- Does My Healthy 65-Year-Old Patient Still Need The 13-Valent Pneumococcal Conjugate Vaccine (PCV13)Document3 pagesDoes My Healthy 65-Year-Old Patient Still Need The 13-Valent Pneumococcal Conjugate Vaccine (PCV13)tsiko111No ratings yet
- Recent Topics of Pneumococcal Vaccination IndicatiDocument14 pagesRecent Topics of Pneumococcal Vaccination IndicatiSaifulhadi BarohNo ratings yet
- MKV 046Document5 pagesMKV 046ardhenaNo ratings yet
- Nac Etiologia Implicacion para La Seleccion de La Poblacion Diseño de Estudios Cid 2008Document4 pagesNac Etiologia Implicacion para La Seleccion de La Poblacion Diseño de Estudios Cid 2008Gustavo GomezNo ratings yet
- Ivermectin JournalDocument11 pagesIvermectin JournalShahidatul Aqmal SahidinNo ratings yet
- CMW 051Document4 pagesCMW 051Laila Kurnia PramonoNo ratings yet
- Journal Pmed 1003787Document20 pagesJournal Pmed 1003787GAYATHIRINo ratings yet
- CAP PCU ScriptDocument5 pagesCAP PCU ScriptDawn Marie AcostaNo ratings yet
- Clostridium 2Document6 pagesClostridium 2Ioana AntonesiNo ratings yet
- Clinical Features and Outcomes of Children Admitted To The PICU Due To Rotavirus Infection GUNDocument5 pagesClinical Features and Outcomes of Children Admitted To The PICU Due To Rotavirus Infection GUNRoxana Ștefania DrăganNo ratings yet
- Dokumen PDFDocument5 pagesDokumen PDFMacchiatoNo ratings yet
- Real-World Evidence Summary: Covid-19 Vaccine AstrazenecaDocument2 pagesReal-World Evidence Summary: Covid-19 Vaccine AstrazenecaDsmmNo ratings yet
- Romanowski 2018Document7 pagesRomanowski 2018betiromerolopez20No ratings yet
- Covid Plasma NEJM2021Document10 pagesCovid Plasma NEJM2021Inès BekriNo ratings yet
- AJCP / Special Article: BackgroundDocument27 pagesAJCP / Special Article: BackgroundnuvitaNo ratings yet
- Barnes2020 Article ThromboembolismAndAnticoagulanDocument10 pagesBarnes2020 Article ThromboembolismAndAnticoagulanRirin Efsa JutiaNo ratings yet
- Neumonia 2022Document18 pagesNeumonia 2022Lele0407No ratings yet
- Diagnosis and Treatment of Bacterial Meningitis: Arch. Dis. ChildDocument7 pagesDiagnosis and Treatment of Bacterial Meningitis: Arch. Dis. Childapi-214563632No ratings yet
- Stroke Management Clinical Practice GuidelinesDocument26 pagesStroke Management Clinical Practice GuidelinesprinsepejesseNo ratings yet
- WHO EURO 2021 2480 42236 58306 EngDocument3 pagesWHO EURO 2021 2480 42236 58306 EngRizka NoviandariNo ratings yet
- hsr2 214Document7 pageshsr2 214mehakNo ratings yet
- HPV - 2Document10 pagesHPV - 2Apd. IDNo ratings yet
- 394 Full PDFDocument20 pages394 Full PDFHaltiNo ratings yet
- Practice: Interpreting A Covid-19 Test ResultDocument7 pagesPractice: Interpreting A Covid-19 Test Resultnecator samiricanusNo ratings yet
- Factors Predicting Mortality in Pulmonary TuberculosisDocument6 pagesFactors Predicting Mortality in Pulmonary TuberculosisCentral Asian StudiesNo ratings yet
- The Management and Prevention of Anal Squamous Cell CarcinomaDocument10 pagesThe Management and Prevention of Anal Squamous Cell CarcinomaGabriela LemNo ratings yet
- Diagnostic and Prognostic Biomarkers of Sepsis in Critical CareDocument8 pagesDiagnostic and Prognostic Biomarkers of Sepsis in Critical Caremr_curiousityNo ratings yet
- Journal 6Document4 pagesJournal 6margareth silaenNo ratings yet
- Efficacy and Safety of A RecombinantDocument13 pagesEfficacy and Safety of A RecombinantSofyanNo ratings yet
- Ventilator AssociatedDocument10 pagesVentilator Associatedtoothfairy2780No ratings yet
- Evaluation of Prescribing Patterns of Antibiotics in General Medicine Ward in A Tertiary Care HospitalDocument6 pagesEvaluation of Prescribing Patterns of Antibiotics in General Medicine Ward in A Tertiary Care HospitalEditor IJTSRDNo ratings yet
- BCG FDA LeafletDocument13 pagesBCG FDA LeafletEllaNo ratings yet
- Kaposi Sarkoma MulutDocument9 pagesKaposi Sarkoma MulutAyik DarkerThan BlackNo ratings yet
- Comparison of Culture and PCR Methods in The Diagnosis of Bacterial MeningitisDocument5 pagesComparison of Culture and PCR Methods in The Diagnosis of Bacterial Meningitisrais123No ratings yet
- Ebn RespiDocument17 pagesEbn RespilablabkurmNo ratings yet
- Cost Utility of Vaccination Against COVID-19 in BrazilDocument8 pagesCost Utility of Vaccination Against COVID-19 in BrazilTatiana DutraNo ratings yet
- Uncertainty and COVID-19Document6 pagesUncertainty and COVID-19Arthur FernandesNo ratings yet
- 2021 Remap-Cap - Activ-4a - Attacc Covid Severes Heparinoptherapie NejmDocument13 pages2021 Remap-Cap - Activ-4a - Attacc Covid Severes Heparinoptherapie Nejmcarb0ne14rNo ratings yet
- RefrDocument6 pagesRefrkahsuNo ratings yet
- Pi Is 2058534917300689Document5 pagesPi Is 2058534917300689Tina woldegebrielNo ratings yet
- Senior Cycle 1 General Practice: Department of General Practice RCSI Medical School DublinDocument27 pagesSenior Cycle 1 General Practice: Department of General Practice RCSI Medical School Dublinpea_ciha05No ratings yet
- E061126 FullDocument12 pagesE061126 FullAdinda Raihana SitorusNo ratings yet
- Nac 2017Document18 pagesNac 2017Nataly CortesNo ratings yet
- Kuppermann2019 PDFDocument10 pagesKuppermann2019 PDFGonzalo CoaquiraNo ratings yet
- Preprint Not Peer Reviewed: STOBE: A Long-COVID Syndromic Study Using Real-World Data in BrazilDocument35 pagesPreprint Not Peer Reviewed: STOBE: A Long-COVID Syndromic Study Using Real-World Data in BrazilDr. Heitor Cavalini FisioterapeutaNo ratings yet
- The DeFlaming Guidelines, How - DAVID SEAMANDocument10 pagesThe DeFlaming Guidelines, How - DAVID SEAMANpigasos100% (3)
- Barium Esophagogram As The First Step To Modern Tecniques: Poster No.: Congress: Type: AuthorsDocument55 pagesBarium Esophagogram As The First Step To Modern Tecniques: Poster No.: Congress: Type: AuthorsbenznakupNo ratings yet
- Fatty Acid OxidationDocument46 pagesFatty Acid OxidationGhaidaa SadeqNo ratings yet
- School NursingDocument41 pagesSchool NursingJas Castro JoveroNo ratings yet
- CBSE Provisions For CWSNDocument20 pagesCBSE Provisions For CWSNManisha Verma100% (1)
- Preterm Labor Case Pres 1Document71 pagesPreterm Labor Case Pres 1mhegan07No ratings yet
- Medical Surgical Nursing Research ThesisDocument6 pagesMedical Surgical Nursing Research ThesisPaperWritersForCollegeUK100% (2)
- English Analysing Themes and Ideas Presentation Beige Pink Lined StyleDocument14 pagesEnglish Analysing Themes and Ideas Presentation Beige Pink Lined StylejrdccuevasNo ratings yet
- Meditation XVII: Meditation #17 by John Donne From Devotions Upon Emergent Occasions (1623), XVIIDocument1 pageMeditation XVII: Meditation #17 by John Donne From Devotions Upon Emergent Occasions (1623), XVIIFlávio FilhoNo ratings yet
- Nursing Care Plan of Client With Fluid and Electrolyte ImbalanceDocument28 pagesNursing Care Plan of Client With Fluid and Electrolyte ImbalanceCj Aguilar50% (2)
- PhobiasDocument3 pagesPhobiasHaifi HunNo ratings yet
- Cardiovascular System Diseases Part 1Document22 pagesCardiovascular System Diseases Part 1Prince Rener Velasco PeraNo ratings yet
- Week 5-6 - IMMU - Post Midterm Immunology - Practice Questions-2Document21 pagesWeek 5-6 - IMMU - Post Midterm Immunology - Practice Questions-2baf49411No ratings yet
- Tangina Mo BizarDocument1 pageTangina Mo BizarJhon eric EscultorNo ratings yet
- Diagnosis of Honey Bee Diseases: United States Department of AgricultureDocument63 pagesDiagnosis of Honey Bee Diseases: United States Department of AgricultureBre ErbNo ratings yet
- DS Ibuprofen Osteo ARLEDDocument11 pagesDS Ibuprofen Osteo ARLEDvivi's eyebrowsNo ratings yet
- Ischemic Stroke Pathophysiology and Principles of Localization (1) G PDFDocument16 pagesIschemic Stroke Pathophysiology and Principles of Localization (1) G PDFGina Ayudia PutriNo ratings yet
- Behavoural Science Solved Past Papers ...... DR Mazhar AbbasDocument23 pagesBehavoural Science Solved Past Papers ...... DR Mazhar Abbasmjawadullah5No ratings yet
- CHAPTER 12 Abdominal PainDocument2 pagesCHAPTER 12 Abdominal PainIvanka Lizbeth PrieteNo ratings yet
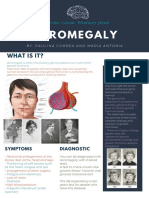
- Acromegaly: What Is It?Document1 pageAcromegaly: What Is It?Paulina CorreaaNo ratings yet
- Red EyeDocument6 pagesRed EyeafatNo ratings yet
- Important Notes Articles For IBPS PODocument8 pagesImportant Notes Articles For IBPS POMilanNo ratings yet
- CHN - Gregorio, Save Us AllDocument3 pagesCHN - Gregorio, Save Us AllShyen100% (1)
- Eating Disorders: Manos, Bencio, Fernandes, ParaisoDocument66 pagesEating Disorders: Manos, Bencio, Fernandes, ParaisoShannen Fernandez100% (1)
- Viral Infections: Presented By: Fatimah Zahraa Ahmed Supervised By: DR - RafilDocument31 pagesViral Infections: Presented By: Fatimah Zahraa Ahmed Supervised By: DR - Rafilfatimah zahraaNo ratings yet
- Arquivos de Gastroenterologia Anais FINAL ARQGA PDFDocument354 pagesArquivos de Gastroenterologia Anais FINAL ARQGA PDFAle AraujoNo ratings yet
- Writing SOAP Notes NYCCDocument7 pagesWriting SOAP Notes NYCCmassagekevin100% (2)