Download as pdf or txt
You might also like
- Helmut Zander, Anthroposophie in DeutschlandDocument14 pagesHelmut Zander, Anthroposophie in DeutschlandBibliorare100% (1)
- Strain and Deflection of A Circular Plate - Lab ReportDocument4 pagesStrain and Deflection of A Circular Plate - Lab ReportRoshane NanayakkaraNo ratings yet
- Eastar SpecificationsDocument2 pagesEastar SpecificationsUmar ShamsudinNo ratings yet
- Monte Carlo Simulation of The Tomotherapy Treatment Unit in The Static Mode Using MC HAMMER, A Monte Carlo Tool Dedicated To TomotherapyDocument11 pagesMonte Carlo Simulation of The Tomotherapy Treatment Unit in The Static Mode Using MC HAMMER, A Monte Carlo Tool Dedicated To TomotherapyenriquefisicoNo ratings yet
- Microwave Imaging ThesisDocument4 pagesMicrowave Imaging ThesisSteven Wallach100% (2)
- Experimental and Monte Carlo Evaluation of Eclipse Treatment Planning System For Lung Dose CalculationsDocument12 pagesExperimental and Monte Carlo Evaluation of Eclipse Treatment Planning System For Lung Dose CalculationsSenaxion AriaNo ratings yet
- Xing 1999Document17 pagesXing 1999RadCalc IOLNo ratings yet
- Sadagopan 2009Document16 pagesSadagopan 2009maryam yaftianNo ratings yet
- Monte Carlo Simulation of 6MV Elekta Synergy Platform Linac Photon Beam Using Gate/Geant4Document10 pagesMonte Carlo Simulation of 6MV Elekta Synergy Platform Linac Photon Beam Using Gate/Geant4Nguyễn Thành CôngNo ratings yet
- Foster - FFFcommissioning in PinnacleDocument12 pagesFoster - FFFcommissioning in PinnacleChristopher Scott RoseNo ratings yet
- Medical Physics - 2021 - Praagh - Fully Automated Quantification Method FQM of Coronary Calcium in An AnthropomorphicDocument12 pagesMedical Physics - 2021 - Praagh - Fully Automated Quantification Method FQM of Coronary Calcium in An AnthropomorphicAmril MukminNo ratings yet
- Algorithm InformationDocument5 pagesAlgorithm Informationapi-691667702No ratings yet
- 410 1667 1 PBDocument7 pages410 1667 1 PBSenaxion AriaNo ratings yet
- Zhao 2008 IIDocument9 pagesZhao 2008 IIenriquefisicoNo ratings yet
- Vera 2019 J. Phys. Conf. Ser. 1160 012001Document8 pagesVera 2019 J. Phys. Conf. Ser. 1160 012001veramig1396No ratings yet
- EPID-based Dosimetry To Verify IMRT Planar DoseDocument13 pagesEPID-based Dosimetry To Verify IMRT Planar Dosexiwevi4103No ratings yet
- Dosimetria Principios CLINACDocument36 pagesDosimetria Principios CLINACyumekiNo ratings yet
- Validation of Monaco Treatment Planning System ForDocument5 pagesValidation of Monaco Treatment Planning System Forঅসীম সীমান্তNo ratings yet
- LaurentDocument2 pagesLaurentmahdi123456789No ratings yet
- J Applied Clin Med Phys - 2016 - Pitcher - Radiation Leakage Dose From Elekta Electron Collimation SystemDocument20 pagesJ Applied Clin Med Phys - 2016 - Pitcher - Radiation Leakage Dose From Elekta Electron Collimation Systemjohan NGONTIENo ratings yet
- Monte Carlo Patient Specific Pre Treatment Qa System For Volumetric Modulated Arc TherapyDocument29 pagesMonte Carlo Patient Specific Pre Treatment Qa System For Volumetric Modulated Arc TherapydianaNo ratings yet
- Watershed CYTOMETRY 1997 PsDocument9 pagesWatershed CYTOMETRY 1997 PsGino Asencio AlvaradoNo ratings yet
- Individual Dosimetry System For Targeted Alpha TheDocument8 pagesIndividual Dosimetry System For Targeted Alpha TheMauricio García CamachoNo ratings yet
- 1 s2.0 S1120179722019731 MainDocument15 pages1 s2.0 S1120179722019731 MainNiamatullahNo ratings yet
- Applied Radiation and IsotopesDocument9 pagesApplied Radiation and IsotopesSUBHANo ratings yet
- Evaluation of RT Imaging DevicesDocument7 pagesEvaluation of RT Imaging DevicesKurt Van DelinderNo ratings yet
- 1 s2.0 S1507136716300864 MainDocument10 pages1 s2.0 S1507136716300864 MainRadCalc IOLNo ratings yet
- On Efficiency of Combined Daubechies Wavelets and Statistical Parameters Applied in MammographyDocument20 pagesOn Efficiency of Combined Daubechies Wavelets and Statistical Parameters Applied in MammographySavita Kiran BNo ratings yet
- Euroblastoma: ASE TudyDocument4 pagesEuroblastoma: ASE TudyOmkar KongariNo ratings yet
- Temporal Bone Imaging: Comparison of Flat Panel Volume CT and Multisection CTDocument6 pagesTemporal Bone Imaging: Comparison of Flat Panel Volume CT and Multisection CTNovi DwiyantiNo ratings yet
- Fedon Et Al-2018-Medical Physics HeteroDocument14 pagesFedon Et Al-2018-Medical Physics HeteroChoi Min YoungNo ratings yet
- Comprehensive Validation of Halcyon 2.0 Plans and The Implementation of Patient Specific QA With Multiple Detector PlatformsDocument10 pagesComprehensive Validation of Halcyon 2.0 Plans and The Implementation of Patient Specific QA With Multiple Detector Platformszhen yongjieNo ratings yet
- Acm2 13 019Document15 pagesAcm2 13 019Carolina CorreiaNo ratings yet
- Titt Et Al-2006-Medical PhysicsDocument9 pagesTitt Et Al-2006-Medical PhysicsSUBHANo ratings yet
- Volumetric-Modulated Arc Therapy Planning Using MuDocument12 pagesVolumetric-Modulated Arc Therapy Planning Using MuАня РыбинаNo ratings yet
- Bio Med PaperDocument13 pagesBio Med PaperironmanjrpNo ratings yet
- Abstract Knee PrativaDocument1 pageAbstract Knee PrativaRks RathoreNo ratings yet
- Multi ChannelDocument57 pagesMulti Channelbasavaraj hagaratagiNo ratings yet
- Development of An Independant Mote Carlo Dose Calculation Quality Assurance Tool For Clinal TrialsDocument1 pageDevelopment of An Independant Mote Carlo Dose Calculation Quality Assurance Tool For Clinal Trialszhen yongjieNo ratings yet
- Results: Figure 1 CRNN Architecture ClassificationDocument5 pagesResults: Figure 1 CRNN Architecture ClassificationAisha ZulifqarNo ratings yet
- Elasticity Detection of IMT of Common Carotid ArteryDocument4 pagesElasticity Detection of IMT of Common Carotid Arterypurushothaman sinivasanNo ratings yet
- Technical Evaluation of Tomotherapy Automatic Roll CorrectionDocument10 pagesTechnical Evaluation of Tomotherapy Automatic Roll CorrectionrochimNo ratings yet
- Cal Dose X ManualDocument23 pagesCal Dose X ManualRadiologi RSUD CiawiNo ratings yet
- 3D Imrt VmatDocument13 pages3D Imrt VmatCristi Arias BadaNo ratings yet
- Dosimetric Comparison of DifferentDocument11 pagesDosimetric Comparison of DifferentDanilo SouzaNo ratings yet
- Description and Dosimetric Verification of The PEREGRINE Monte Carlo Dose Calculation System For Photon Beams Incident On A Water PhantomDocument22 pagesDescription and Dosimetric Verification of The PEREGRINE Monte Carlo Dose Calculation System For Photon Beams Incident On A Water PhantomLaellyArifannyNo ratings yet
- Staffhome - Qut.edu - Au Staffgroupt$ Trapp Documents Jamie Research Eprints IUPESM WC2015 Kairn InterplayDocument5 pagesStaffhome - Qut.edu - Au Staffgroupt$ Trapp Documents Jamie Research Eprints IUPESM WC2015 Kairn InterplayZeka ValladolidNo ratings yet
- PIIS1120179711001438Document5 pagesPIIS1120179711001438johan NGONTIENo ratings yet
- Conference PaperDocument14 pagesConference PaperMuhammad Nauman UsmaniNo ratings yet
- Vera 2019 J. Phys. Conf. Ser. 1160 012001Document8 pagesVera 2019 J. Phys. Conf. Ser. 1160 012001veramig1396No ratings yet
- Cirro NeDocument4 pagesCirro NeNguyễn Thành CôngNo ratings yet
- Research Article Microwave Tomography System For Methodical Testing of Human Brain Stroke Detection ApproachesDocument10 pagesResearch Article Microwave Tomography System For Methodical Testing of Human Brain Stroke Detection ApproachesChinaski BukowskiNo ratings yet
- Thesis PAPERDocument10 pagesThesis PAPERAhmed AbdelhadyNo ratings yet
- Comparison of Two Commercial Detector Arrays For IMRT Quality AssuranceDocument13 pagesComparison of Two Commercial Detector Arrays For IMRT Quality AssuranceenriquefisicoNo ratings yet
- Introduction: Types of PhantomDocument4 pagesIntroduction: Types of PhantomAmir ChaNdiaNo ratings yet
- Achieving Reduced Radiation Doses For CT Examination of The Brain Using Optimal Exposure ParametersDocument6 pagesAchieving Reduced Radiation Doses For CT Examination of The Brain Using Optimal Exposure ParametersHamza ArjahNo ratings yet
- Calculo Ontecarlo MetodologiaDocument5 pagesCalculo Ontecarlo MetodologiaCarlos GutierrezNo ratings yet
- An Application of The Empirical Mode Decomposition To Brain Magnetic Resonance Images ClassificationDocument4 pagesAn Application of The Empirical Mode Decomposition To Brain Magnetic Resonance Images ClassificationXavier Martínez MoctezumaNo ratings yet
- Technical Principles of MSCTDocument13 pagesTechnical Principles of MSCTNguyễn HùngNo ratings yet
- Monte Carlo Simulations in Medical Imaging P. F. LiaparinosDocument7 pagesMonte Carlo Simulations in Medical Imaging P. F. Liaparinosjiar001No ratings yet
- Integrated SFCW Transceivers For UWB Breast Cancer Imaging: Architectures and Circuit ConstraintsDocument14 pagesIntegrated SFCW Transceivers For UWB Breast Cancer Imaging: Architectures and Circuit ConstraintsJesus Alejandro Amaya HernandezNo ratings yet
- Circulating Tumor Cells: Isolation and AnalysisFrom EverandCirculating Tumor Cells: Isolation and AnalysisZ. Hugh FanNo ratings yet
- Spline and Spline Wavelet Methods with Applications to Signal and Image Processing: Volume III: Selected TopicsFrom EverandSpline and Spline Wavelet Methods with Applications to Signal and Image Processing: Volume III: Selected TopicsNo ratings yet
- MC Simulation of Radiation-Induced DNA Double Strand BreaksDocument12 pagesMC Simulation of Radiation-Induced DNA Double Strand BreaksChloe FanningNo ratings yet
- Lampe 2018Document11 pagesLampe 2018Chloe FanningNo ratings yet
- A Free Program For Calculating EUD-based NTCP and TCP in External Beam RadiotherapyDocument11 pagesA Free Program For Calculating EUD-based NTCP and TCP in External Beam RadiotherapyChloe FanningNo ratings yet
- GATE-UsersGuideV8 0Document374 pagesGATE-UsersGuideV8 0Chloe FanningNo ratings yet
- Connector: C175T: Powertrain Control Module (PCM) 15525 12A650Document2 pagesConnector: C175T: Powertrain Control Module (PCM) 15525 12A650Matias MartinezNo ratings yet
- Frampton AntithesispedagogyDocument2 pagesFrampton AntithesispedagogyJohann WieseNo ratings yet
- Flow of Communication: Emergency Response For Oil SpillageDocument5 pagesFlow of Communication: Emergency Response For Oil Spillagenarm nNo ratings yet
- InfoDocument2 pagesInfofukinbobNo ratings yet
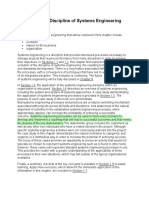
- Chapter 1: The Discipline of Systems EngineeringDocument31 pagesChapter 1: The Discipline of Systems EngineeringTrixiNo ratings yet
- Shortest Route ProblemDocument7 pagesShortest Route ProblemkaushalmightyNo ratings yet
- Vacant Seats: 5-Year Integrated M.Sc. (Hons.) ProgrammesDocument2 pagesVacant Seats: 5-Year Integrated M.Sc. (Hons.) Programmesmana khantNo ratings yet
- Spare Parts Catalogue: AXLE 26.18 - (CM8118) REF: 133821Document8 pagesSpare Parts Catalogue: AXLE 26.18 - (CM8118) REF: 133821Paulinho InformáticaNo ratings yet
- Bill of QuantityDocument6 pagesBill of QuantityKhairoden SangcopanNo ratings yet
- Yellow Illustrative Digital Education For Children InfographicDocument1 pageYellow Illustrative Digital Education For Children InfographicNur Azimah AzibNo ratings yet
- Hangman Interactive TemplateDocument17 pagesHangman Interactive Templatekedisharobinson1No ratings yet
- Continuous Usage Intention of Social Media As An Online Information Distribution ChannelsDocument12 pagesContinuous Usage Intention of Social Media As An Online Information Distribution Channelsapi-563385491No ratings yet
- Is Codes ListDocument37 pagesIs Codes Listmoondonoo7No ratings yet
- Bibby CouplingsDocument25 pagesBibby CouplingsKemoy JohnsonNo ratings yet
- Introduction To Management ScienceDocument30 pagesIntroduction To Management ScienceVenice Marie Arroyo100% (1)
- Application Form For Initial Review: Section A - Basic InformationDocument33 pagesApplication Form For Initial Review: Section A - Basic Informationsaptarshi DasNo ratings yet
- 1001076002-HT8911 Datasheet - V1.1Document13 pages1001076002-HT8911 Datasheet - V1.1Zhang EthanNo ratings yet
- 13-GB 50018-2002-EnDocument109 pages13-GB 50018-2002-Enyyyy071220100% (1)
- Anullment CATHOLIC TRIBUNALDocument20 pagesAnullment CATHOLIC TRIBUNALMons Jr BaturianoNo ratings yet
- International Strategic Alliances 1Document21 pagesInternational Strategic Alliances 1mukesh93567No ratings yet
- SCIETECHNODocument19 pagesSCIETECHNOChini ChanNo ratings yet
- Textbook - Thermal Physics PopleDocument26 pagesTextbook - Thermal Physics PoplecowsarechillNo ratings yet
- Mayank Selection & Recruitment Process BluedartDocument5 pagesMayank Selection & Recruitment Process BluedartMayank SahuNo ratings yet
- Internship Report - AmtechDocument31 pagesInternship Report - AmtechRahil ShahNo ratings yet
- MySQL Cheat Sheet PDFDocument2 pagesMySQL Cheat Sheet PDFEsha ShahNo ratings yet
- THE Cost OF Delay IN ConstructionDocument3 pagesTHE Cost OF Delay IN ConstructionJonathan WallaceNo ratings yet
- Volume AdministrationDocument264 pagesVolume AdministrationeviyipyipNo ratings yet