Download as docx, pdf, or txt
You might also like
- Cleanroom Contamination Prevention & Control: A Practical Guide To The ScienceDocument13 pagesCleanroom Contamination Prevention & Control: A Practical Guide To The ScienceTim Sandle56% (9)
- Medicine in Brief: Name the Disease in Haiku, Tanka and ArtFrom EverandMedicine in Brief: Name the Disease in Haiku, Tanka and ArtRating: 5 out of 5 stars5/5 (1)
- The AMBOSS International 100 Day Study Plan PDFDocument30 pagesThe AMBOSS International 100 Day Study Plan PDFAli Aborges Jr.100% (2)
- Angelito L. Ramos Jr. RN Clinical InstructorDocument68 pagesAngelito L. Ramos Jr. RN Clinical Instructorraymondblade18100% (17)
- Chapter 8 ACCA F2Document9 pagesChapter 8 ACCA F2sikshaNo ratings yet
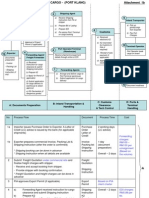
- Export + Import Process Flow - Break Bulk Cargo 27072010Document11 pagesExport + Import Process Flow - Break Bulk Cargo 27072010Ahmad Fauzi Mehat100% (1)
- Pulmonary Thromboembolism: DR Olubunmi Ogunlade Consultant PulmonologistDocument34 pagesPulmonary Thromboembolism: DR Olubunmi Ogunlade Consultant PulmonologistEmeka Chinedu Precious PetrousNo ratings yet
- Pathophysiologic Response of The To Arterial Obstruction and of TheDocument10 pagesPathophysiologic Response of The To Arterial Obstruction and of Thestudy mailNo ratings yet
- Pulmonary EmbolismDocument96 pagesPulmonary Embolismsamice5100% (1)
- Pulmonary Embolism: DR Ntambo L.KDocument43 pagesPulmonary Embolism: DR Ntambo L.Khazunga rayfordNo ratings yet
- Acute Pulmonary EmbolismDocument7 pagesAcute Pulmonary EmbolismSami Chemais100% (1)
- Pulmonary Embolism 2013Document78 pagesPulmonary Embolism 2013mousa elshamlyNo ratings yet
- Respiratory Arrest: Chest Trauma Thoracic TraumaDocument17 pagesRespiratory Arrest: Chest Trauma Thoracic TraumaKay MirandaNo ratings yet
- Deep Venous Thrombosis and Pulmonary ThromboembolismDocument19 pagesDeep Venous Thrombosis and Pulmonary ThromboembolismTaqdees ManzoorNo ratings yet
- DynaMed Plus - Pulmonary Embolism (PE)Document85 pagesDynaMed Plus - Pulmonary Embolism (PE)Gamer MadaNo ratings yet
- Pulmonary HypertensionDocument29 pagesPulmonary Hypertensionomod415No ratings yet
- Pulmonary EmbolismDocument21 pagesPulmonary EmbolismChoga Ilham ArlandoNo ratings yet
- Venous Thromboembolism (VTE)Document8 pagesVenous Thromboembolism (VTE)Anisah AliNo ratings yet
- Pulmonary Embolism, Comparison Two Different Creteria For DiagnosisDocument25 pagesPulmonary Embolism, Comparison Two Different Creteria For Diagnosisgeorvin marcoNo ratings yet
- Embolia PulmonaraDocument3 pagesEmbolia PulmonaraAlina GheNo ratings yet
- Venous Thromboembolism: DR Abdelmoniem Saeed Mohammed Er SpecialistDocument43 pagesVenous Thromboembolism: DR Abdelmoniem Saeed Mohammed Er SpecialistYousef Al-AmeenNo ratings yet
- Pulmonary Embolism PEDocument18 pagesPulmonary Embolism PESafa SalehNo ratings yet
- Pulmonary EmbolismDocument75 pagesPulmonary EmbolismMuntasir BashirNo ratings yet
- Acute Heart FailureDocument9 pagesAcute Heart FailureChen Briones100% (1)
- Pulmonary Embolism 27 JanDocument8 pagesPulmonary Embolism 27 JanDeepak MulajkerNo ratings yet
- Deep Venous Thrombosis & Pulmonary EmbolismDocument11 pagesDeep Venous Thrombosis & Pulmonary EmbolismJuma AwarNo ratings yet
- Deep Vein ThrombosisDocument9 pagesDeep Vein ThrombosisGladys YaresNo ratings yet
- Deep Vein ThrombosisDocument9 pagesDeep Vein ThrombosisGladys YaresNo ratings yet
- 16 - Venous ThromboembolismDocument2 pages16 - Venous ThromboembolismLenard BangugNo ratings yet
- Cardiovascular System: by DR - Nuha Abdel GhaffarDocument41 pagesCardiovascular System: by DR - Nuha Abdel GhaffarMohammed Alaa EldeanNo ratings yet
- Pulmonary EdemaDocument20 pagesPulmonary EdemaMohmmad Lateef GanieNo ratings yet
- Deep Vein Thrombosis / Pulmonary EmbolismDocument55 pagesDeep Vein Thrombosis / Pulmonary EmbolismSenti AnnamalaiNo ratings yet
- DEEP VEIN THROMBOSIS Practice EssentialsDocument63 pagesDEEP VEIN THROMBOSIS Practice Essentialsqayyum consultantfpscNo ratings yet
- 13 Pulmonary EmbolismDocument45 pages13 Pulmonary EmbolismMiky DinuNo ratings yet
- Pulmonary Embolism (PE) PDFDocument9 pagesPulmonary Embolism (PE) PDFMileNo ratings yet
- (Cardiology Clinics) Ori Ben-Yehuda, Michael H. Crawford - Pulmonary Vascular Disease-Saunders (2004)Document145 pages(Cardiology Clinics) Ori Ben-Yehuda, Michael H. Crawford - Pulmonary Vascular Disease-Saunders (2004)LucasPeresBetNo ratings yet
- Acute Pulmonary EmbolismDocument13 pagesAcute Pulmonary EmbolismIrina SumeicoNo ratings yet
- Cor PulmonaleDocument40 pagesCor PulmonaleIbtissame BadadNo ratings yet
- Deep Vein Thrombosis: by Dr. Muhammad Umair ChangDocument20 pagesDeep Vein Thrombosis: by Dr. Muhammad Umair ChangumairNo ratings yet
- Pulmonary EmbolismDocument48 pagesPulmonary Embolismganga2424100% (3)
- Heart Failure RevisionDocument4 pagesHeart Failure RevisionBlanaid MargaretNo ratings yet
- Acute Pulmonary Embolism Dokter ZakkyDocument1 pageAcute Pulmonary Embolism Dokter ZakkyDewi AmeliaNo ratings yet
- Pulmonary Embolism: DR A Hammangabdo Fwacp Professor and Cosultant PulmonologistDocument28 pagesPulmonary Embolism: DR A Hammangabdo Fwacp Professor and Cosultant PulmonologistAdamu Muhammad Dumbulwa100% (1)
- A Pulmonary EmbolismDocument11 pagesA Pulmonary EmbolismMonica Damayani SusiloNo ratings yet
- Cor Pulmonale - StatPearls - NCBI BookshelfDocument4 pagesCor Pulmonale - StatPearls - NCBI BookshelfAldi RafaelNo ratings yet
- Trombembolismul Pulmonar - RO - 2Document73 pagesTrombembolismul Pulmonar - RO - 2Laura AmaliaNo ratings yet
- Heart FailureDocument47 pagesHeart Failureedry901No ratings yet
- Pulmonaryembolism 150329161109 Conversion Gate01Document60 pagesPulmonaryembolism 150329161109 Conversion Gate01Rafika RaraNo ratings yet
- Congenital Heart DiseaseDocument124 pagesCongenital Heart DiseasemulkanmustafaNo ratings yet
- Pulmonary Embolism: AetiologyDocument15 pagesPulmonary Embolism: AetiologyEmad ElhusseinNo ratings yet
- Acute Biologic Crisis-ArDocument71 pagesAcute Biologic Crisis-ArJayvee Novenario CasaljayNo ratings yet
- Pleural Effusion: Zubeir Ahmed BareDocument30 pagesPleural Effusion: Zubeir Ahmed BareAnisa Osman HassanNo ratings yet
- Congenital Heart DeseasesDocument54 pagesCongenital Heart DeseasesAntony100% (1)
- Resp N41Document11 pagesResp N41ashafernandesssNo ratings yet
- Board Review Pediatrics PDFDocument215 pagesBoard Review Pediatrics PDFJoanne Blanco100% (1)
- Venous Thromboembolism (VTE) Pathophysiology September 2016Document46 pagesVenous Thromboembolism (VTE) Pathophysiology September 2016Nick GouvatsosNo ratings yet
- Overview of Acute Pulmonary Embolism in AdultsDocument33 pagesOverview of Acute Pulmonary Embolism in AdultsEyla Breceda Garc�aNo ratings yet
- DVT and Pulmonary Thromboembolism 43Document53 pagesDVT and Pulmonary Thromboembolism 43HussenNo ratings yet
- HEMOPTYSISDocument37 pagesHEMOPTYSISVarun B RenukappaNo ratings yet
- Venous Thromboembolism (VTE)Document33 pagesVenous Thromboembolism (VTE)Kris ChenNo ratings yet
- Acute Pulmonary EmbolismDocument82 pagesAcute Pulmonary Embolismincredible Prages100% (1)
- Pleural EffusionsDocument41 pagesPleural Effusionssanjivdas100% (1)
- Pharmacotherapeutic Management of Cardiovascular Disease Complications: A Textbook for Medical StudentsFrom EverandPharmacotherapeutic Management of Cardiovascular Disease Complications: A Textbook for Medical StudentsNo ratings yet
- PharyngitisDocument10 pagesPharyngitisAli Aborges Jr.No ratings yet
- Kievlyanin 1904 27Document8 pagesKievlyanin 1904 27Ali Aborges Jr.No ratings yet
- Coronary Artery DiseaseDocument20 pagesCoronary Artery DiseaseAli Aborges Jr.No ratings yet
- Emergency Care Algorithms 2023Document88 pagesEmergency Care Algorithms 2023Ali Aborges Jr.No ratings yet
- PneumoniaDocument41 pagesPneumoniaAli Aborges Jr.No ratings yet
- Clostridioides Difficile Infection: in Adults and ChildrenDocument40 pagesClostridioides Difficile Infection: in Adults and ChildrenAli Aborges Jr.No ratings yet
- Treatment of Graves' Orbitopathy (Ophthalmopathy) - UpToDateDocument22 pagesTreatment of Graves' Orbitopathy (Ophthalmopathy) - UpToDateAli Aborges Jr.No ratings yet
- Cardiac Physiology PDFDocument17 pagesCardiac Physiology PDFAli Aborges Jr.No ratings yet
- UntitledמממDocument96 pagesUntitledמממAli Aborges Jr.No ratings yet
- UW Note The BestDocument63 pagesUW Note The BestAli Aborges Jr.No ratings yet
- GuidelinesDocument62 pagesGuidelinesAli Aborges Jr.No ratings yet
- CardioDocument261 pagesCardioAli Aborges Jr.No ratings yet
- Liver AbscessDocument15 pagesLiver AbscessAli Aborges Jr.No ratings yet
- Pathophysiology of KidneysDocument35 pagesPathophysiology of KidneysAli Aborges Jr.No ratings yet
- УСПDocument50 pagesУСПAli Aborges Jr.No ratings yet
- Ziad Aro, MD Internal MedicineDocument100 pagesZiad Aro, MD Internal MedicineAli Aborges Jr.No ratings yet
- Ziad Aro, MD Internal MedicineDocument91 pagesZiad Aro, MD Internal MedicineAli Aborges Jr.No ratings yet
- סילובס מבחן רישוי 111Document43 pagesסילובס מבחן רישוי 111Ali Aborges Jr.No ratings yet
- Medical Emergency CS 79Document9 pagesMedical Emergency CS 79Ali Aborges Jr.No ratings yet
- Free/Open Source Multibody and Aerodynamic Software For Aeroelastic Analysis of Wind TurbinesDocument14 pagesFree/Open Source Multibody and Aerodynamic Software For Aeroelastic Analysis of Wind TurbinesFrankNo ratings yet
- Cold Agglutinin DiseaseDocument4 pagesCold Agglutinin Diseasenavneet21usNo ratings yet
- ASHRAE-tables Lighting Power Density PDFDocument3 pagesASHRAE-tables Lighting Power Density PDFDan MolloyNo ratings yet
- PCI EO MEG Pemex 2013 PDFDocument38 pagesPCI EO MEG Pemex 2013 PDFepesanoNo ratings yet
- E-CatvScope Catalog PDFDocument80 pagesE-CatvScope Catalog PDFAlexander PischulinNo ratings yet
- Heidegger-Origin of The Work of ArtDocument7 pagesHeidegger-Origin of The Work of Artपरन्तप100% (2)
- JNTUH R09 Percentage & Credits Calculator-1Document16 pagesJNTUH R09 Percentage & Credits Calculator-1msg2dpNo ratings yet
- Generalized Analysis of Quasi-Steady-State and Quasi-Transient Measurements of Carrier Lifetimes in SemiconductorsDocument4 pagesGeneralized Analysis of Quasi-Steady-State and Quasi-Transient Measurements of Carrier Lifetimes in SemiconductorsMohaimen UzzamanNo ratings yet
- Construction Method (PICC)Document2 pagesConstruction Method (PICC)rheymar diwaNo ratings yet
- Yaesu FT-1802 Operating ManualDocument88 pagesYaesu FT-1802 Operating ManualYayok S. AnggoroNo ratings yet
- Soft Computing Module IDocument161 pagesSoft Computing Module INatarajanSubramanyamNo ratings yet
- Princeton 112 Plus Service ManualDocument8 pagesPrinceton 112 Plus Service ManualDavid OliveiraNo ratings yet
- Mineral Processing Laboratory ManualDocument43 pagesMineral Processing Laboratory Manualalnemangi100% (1)
- Polynomial FunctionDocument36 pagesPolynomial FunctionfaithreignNo ratings yet
- Unit-Iv Nanomaterials and Nanotechnology: Part-ADocument4 pagesUnit-Iv Nanomaterials and Nanotechnology: Part-AKrishna ThiruvengadamNo ratings yet
- Gateway To Art - 1.08Document40 pagesGateway To Art - 1.08i am bubbleNo ratings yet
- LDPDocument46 pagesLDPSoundradevi ArumugamNo ratings yet
- Design and Implementation of A Distributed IOT System in AquacultureDocument7 pagesDesign and Implementation of A Distributed IOT System in AquacultureAnun YuserboNo ratings yet
- Méthodes de Dissolution FDADocument129 pagesMéthodes de Dissolution FDACH NarimaneNo ratings yet
- STAAD - Pro Plates and Solid Elements (FAQ) - RAM - STAAD Wiki - RAM - STAAD - Bentley CommunitiesDocument15 pagesSTAAD - Pro Plates and Solid Elements (FAQ) - RAM - STAAD Wiki - RAM - STAAD - Bentley CommunitiesKamal RaoNo ratings yet
- Guidelines To An Informal LetterDocument3 pagesGuidelines To An Informal LetterNik Syahina0% (1)
- List of Coolers and HeatersDocument2 pagesList of Coolers and HeatersadityasahayNo ratings yet
- DL24MP HDocument13 pagesDL24MP HTamás SzabóNo ratings yet
- Evaluation of Green Building in The Existing Building of The Department of The Environment of DKI Jakarta Province in The Order of Reducing Greenhouse Gas EmissionsDocument5 pagesEvaluation of Green Building in The Existing Building of The Department of The Environment of DKI Jakarta Province in The Order of Reducing Greenhouse Gas EmissionsInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Recipes From The Foothills Cuisine of Blackberry FarmDocument12 pagesRecipes From The Foothills Cuisine of Blackberry FarmThe Recipe Club50% (2)
- Edux110 SimDocument307 pagesEdux110 SimElijahNo ratings yet
- Msds ManganDocument6 pagesMsds ManganLaely N AfidaNo ratings yet