
Pharm 00 A14
Pharm 00 A14
You might also like
- Hippo Emergency Medicine Board Review - Cram Section - MnemonicsDocument1 pageHippo Emergency Medicine Board Review - Cram Section - MnemonicslotskiNo ratings yet
- OCCUPATIONAL DISEASES Clinical cases 2015 англ 2Document28 pagesOCCUPATIONAL DISEASES Clinical cases 2015 англ 2kjk100% (1)
- MCAT Biology Complete OutlinesDocument34 pagesMCAT Biology Complete OutlinesJacob Mikhail90% (10)
- Gastrointestinal System (Letu Da) PDFDocument74 pagesGastrointestinal System (Letu Da) PDFNafiul Islam100% (4)
- Phys Offluidselectrolytes7 121107201529 Phpapp02Document38 pagesPhys Offluidselectrolytes7 121107201529 Phpapp02Rehab weridaNo ratings yet
- Cardiovascular System: Department of Biochemistry. Faculty of Medicine, UNHAS Rosdiana NatzirDocument68 pagesCardiovascular System: Department of Biochemistry. Faculty of Medicine, UNHAS Rosdiana NatzirikhyNo ratings yet
- Physiology RenalDocument14 pagesPhysiology Renalahmedsalah565vvvNo ratings yet
- PKPD Esterase1Document2 pagesPKPD Esterase1أسعد حسنانNo ratings yet
- Bioch CL 7. Enzime Utilizate in Diagnostic 20-21 (R+e)Document44 pagesBioch CL 7. Enzime Utilizate in Diagnostic 20-21 (R+e)Andrea ModestieNo ratings yet
- 2024 - Aula Grupo - Metabolismo Colesterol e Ácidos Biliares 2Document42 pages2024 - Aula Grupo - Metabolismo Colesterol e Ácidos Biliares 2MavumeNo ratings yet
- Biochemistry of Cardiovascular SystemDocument113 pagesBiochemistry of Cardiovascular SystemNindy75% (4)
- Enzyme IsoenzymesDocument60 pagesEnzyme IsoenzymesSrishti GoenkaNo ratings yet
- I So EnzymesDocument31 pagesI So Enzymesalinaibrar80No ratings yet
- Answers of Exam Ques.Document3 pagesAnswers of Exam Ques.Sonali SehrawatNo ratings yet
- Alcoholics - Episode 289 - Step 1, Step 2CK, Step 3Document2 pagesAlcoholics - Episode 289 - Step 1, Step 2CK, Step 3dhanwin shettyNo ratings yet
- Fluids and Electrolytes Fluids and Electrolytes Acids, Bases, and Acids, Bases, and PH PH By: By: SMM SMM,, RN RN MD MD By: By: SMM SMM,, RN RN MD MDDocument50 pagesFluids and Electrolytes Fluids and Electrolytes Acids, Bases, and Acids, Bases, and PH PH By: By: SMM SMM,, RN RN MD MD By: By: SMM SMM,, RN RN MD MDRose AlmanzorNo ratings yet
- Cholesteril MetabolismDocument54 pagesCholesteril MetabolismAna AbuladzeNo ratings yet
- Liquidos y Electrolitos 2016Document5 pagesLiquidos y Electrolitos 2016MARIA JOSE MEDINA JAIMES100% (1)
- Bone SemeioticaDocument11 pagesBone SemeioticaFrancesco De PalmaNo ratings yet
- Body Fluids: M. Alif Prizarky 04011381419173 GammaDocument7 pagesBody Fluids: M. Alif Prizarky 04011381419173 GammaAlviss RmidNo ratings yet
- EnzymesDocument18 pagesEnzymesRichard PoonNo ratings yet
- Kenzu B, (MD, Asst - Professor of Surgery)Document40 pagesKenzu B, (MD, Asst - Professor of Surgery)kenzu bedruNo ratings yet
- Body Fluids and Blood - HUMAN PHYSIOLOGYDocument29 pagesBody Fluids and Blood - HUMAN PHYSIOLOGYSodeinde SimeonNo ratings yet
- Explorarea Echilibrului Hidro - ElectroliticDocument77 pagesExplorarea Echilibrului Hidro - ElectroliticCopăcel AlexandraNo ratings yet
- Lecture EnzymesDocument45 pagesLecture EnzymesJohn Alfrey Dondiego PuebloNo ratings yet
- Gangguan Dan Keseimbangan Cairan Dan ElektrolitDocument37 pagesGangguan Dan Keseimbangan Cairan Dan ElektrolitFyana PutriNo ratings yet
- Lec. 3 - Fluid and ElectrolyteDocument16 pagesLec. 3 - Fluid and Electrolyteمجيب سلطانNo ratings yet
- 10 Pyruvate Oxid Tricarb Acid Cycle Notes GanapathyDocument7 pages10 Pyruvate Oxid Tricarb Acid Cycle Notes Ganapathykalps.galleryNo ratings yet
- Biochemistry of CVSDocument311 pagesBiochemistry of CVSAsne ManNo ratings yet
- Metabolic Aspect of CVSDocument25 pagesMetabolic Aspect of CVSsamar yousif mohamedNo ratings yet
- CH 18 Cholesterol Metabolism: Biochem Block 3 NotesDocument38 pagesCH 18 Cholesterol Metabolism: Biochem Block 3 NotesJoseph KimNo ratings yet
- Cardiac EnzymesDocument20 pagesCardiac Enzymesstrypto123aaaNo ratings yet
- TCA CycleDocument47 pagesTCA CycleMita SeptianiNo ratings yet
- 04 Metabolisme Xenobiotik NWDocument36 pages04 Metabolisme Xenobiotik NWDesy NataliaNo ratings yet
- Lecture 05. Lipid Metabolism-2. Lipogenesis. Metabolism of Cholesterol and Ketone Bodies.Document33 pagesLecture 05. Lipid Metabolism-2. Lipogenesis. Metabolism of Cholesterol and Ketone Bodies.Віталій Михайлович НечипорукNo ratings yet
- Medical-Surgical Nursing 1Document28 pagesMedical-Surgical Nursing 1Maui Ting100% (1)
- PeroxisomesDocument2 pagesPeroxisomesIndigoSilverNo ratings yet
- Organophosphates (OPs) and Carbamates (CMS)Document15 pagesOrganophosphates (OPs) and Carbamates (CMS)مصطفى أحمدNo ratings yet
- Clinical EnzymologyDocument23 pagesClinical EnzymologyKishore KaranNo ratings yet
- FluidslectureDocument26 pagesFluidslectureIgor StefanetNo ratings yet
- Chapter 18 Lippincott BiochemistryDocument62 pagesChapter 18 Lippincott BiochemistryMeysam SajjadiNo ratings yet
- 228 Carbohydrate MetabolismDocument43 pages228 Carbohydrate MetabolismAmanullahNo ratings yet
- FLuid & Elect & Acid Base & Surg. Nutr.Document24 pagesFLuid & Elect & Acid Base & Surg. Nutr.anon_761270640No ratings yet
- Fluid BalanceDocument30 pagesFluid BalanceBadrun DalangNo ratings yet
- Funda Fluids Elect.Document26 pagesFunda Fluids Elect.j UNo ratings yet
- Body Fluids and ElectrolytesDocument42 pagesBody Fluids and ElectrolytesQusaiBadr100% (1)
- 15.fluid BalanceDocument48 pages15.fluid BalanceImtiaz AhmadNo ratings yet
- Student Book 2Document101 pagesStudent Book 2helena coelho odaNo ratings yet
- Physiology - BSDocument14 pagesPhysiology - BSkep1313No ratings yet
- Cholesterol and Steroid MetabolismDocument17 pagesCholesterol and Steroid MetabolismMarkyNo ratings yet
- Biochem Questions SlidesDocument46 pagesBiochem Questions SlidesTelesha Zabie50% (2)
- Phase: I Hydrolysis of XenobioticsDocument37 pagesPhase: I Hydrolysis of XenobioticsSunilNo ratings yet
- Fluid and Electrolyte TherapyDocument23 pagesFluid and Electrolyte TherapyJamal ArizonaNo ratings yet
- Clinical Enzymology 2Document55 pagesClinical Enzymology 2reuben kwotaNo ratings yet
- MI - 11 - Ciclo de Cori, Creatina Fosfato y Ciclos Energéticos Del MúsculoDocument39 pagesMI - 11 - Ciclo de Cori, Creatina Fosfato y Ciclos Energéticos Del MúsculoANDRÉS FELIPE VALDERRAMA BAEZNo ratings yet
- Fluids and Electrolytes Part 1Document4 pagesFluids and Electrolytes Part 1baraderoayyah41No ratings yet
- Causes HyperlactemiaDocument5 pagesCauses HyperlactemiaArvin ReinaldoNo ratings yet
- Carbohydrate Metabolism 2Document41 pagesCarbohydrate Metabolism 2Shimmering MoonNo ratings yet
- Disorders of Potassium Metabolism PresentationDocument20 pagesDisorders of Potassium Metabolism PresentationSolomon Fallah Foa SandyNo ratings yet
- Chapter 17 18 Cholesterol Metabolism and Protaglandins b7990672Document18 pagesChapter 17 18 Cholesterol Metabolism and Protaglandins b7990672toumeh.halaNo ratings yet
- Fluid and Electrolytes: Ma. Medine L. Amorsolo RN ManDocument29 pagesFluid and Electrolytes: Ma. Medine L. Amorsolo RN ManMichael Baylon Dueñas100% (1)
- Physiol 93 B3Document1 pagePhysiol 93 B3DonkeyManNo ratings yet
- CEACCP - KetamineDocument5 pagesCEACCP - KetamineDonkeyManNo ratings yet
- CEACCP - Latex AllergyDocument4 pagesCEACCP - Latex AllergyDonkeyManNo ratings yet
- CEACCP - Illegal Substances in Anaesthetic and Intensive Care PracticesDocument5 pagesCEACCP - Illegal Substances in Anaesthetic and Intensive Care PracticesDonkeyManNo ratings yet
- Pharmacodynamics, Drug Action Targets, PharmacogeneticsDocument21 pagesPharmacodynamics, Drug Action Targets, PharmacogeneticsDonkeyManNo ratings yet
- Cellular Physiology SAQsDocument1 pageCellular Physiology SAQsDonkeyManNo ratings yet
- Define The Mechanisms of Action and Adverse Effects of Metoprolol, GTN, and Diltiazem When Used To Manage MIDocument2 pagesDefine The Mechanisms of Action and Adverse Effects of Metoprolol, GTN, and Diltiazem When Used To Manage MIDonkeyManNo ratings yet
- Pharm 02 A11Document4 pagesPharm 02 A11DonkeyManNo ratings yet
- CEACCP - Intrathecal Opioids in The Management of Acute Postoperative PainDocument5 pagesCEACCP - Intrathecal Opioids in The Management of Acute Postoperative PainDonkeyManNo ratings yet
- Pharm 00 B15Document2 pagesPharm 00 B15DonkeyManNo ratings yet
- Outline The Physiological Consequences of Hyperosmolar Diabetic KetoacidosisDocument2 pagesOutline The Physiological Consequences of Hyperosmolar Diabetic KetoacidosisDonkeyManNo ratings yet
- Pharm 02 A10Document2 pagesPharm 02 A10DonkeyManNo ratings yet
- Pharm 00 A15Document2 pagesPharm 00 A15DonkeyManNo ratings yet
- Compare and Contrast Neostigmine and The Organophosphate CompoundsDocument1 pageCompare and Contrast Neostigmine and The Organophosphate CompoundsDonkeyManNo ratings yet
- Pharm 00 B11Document1 pagePharm 00 B11DonkeyManNo ratings yet
- Pharm 00 B14Document2 pagesPharm 00 B14DonkeyManNo ratings yet
- Pharm 00 A12Document1 pagePharm 00 A12DonkeyManNo ratings yet
- Compare and Contrast Atropine and Glycopyrulate, and Discuss The Clinical ImplicationsDocument2 pagesCompare and Contrast Atropine and Glycopyrulate, and Discuss The Clinical ImplicationsDonkeyManNo ratings yet
- Compare and Contrast The Pharamcology of Ephedrine and NoradrenalineDocument1 pageCompare and Contrast The Pharamcology of Ephedrine and NoradrenalineDonkeyManNo ratings yet
- Pharm 00 A9Document2 pagesPharm 00 A9DonkeyManNo ratings yet
- Compare and Contrast The Pharmacology of Esmolol and PropanololDocument1 pageCompare and Contrast The Pharmacology of Esmolol and PropanololDonkeyManNo ratings yet
- FS Antimicrobial Dosing Obesity AMS Updates Issue4 - Nov2018Document4 pagesFS Antimicrobial Dosing Obesity AMS Updates Issue4 - Nov2018DonkeyManNo ratings yet
- Comparative Pharmacokinetics of Fentanyl and Alfentanil: Br. J. Anaesth. (1982), 54, 871Document7 pagesComparative Pharmacokinetics of Fentanyl and Alfentanil: Br. J. Anaesth. (1982), 54, 871DonkeyManNo ratings yet
- VOLATILEAGENTSDocument4 pagesVOLATILEAGENTSDonkeyManNo ratings yet
- The Physiology of The GIT and The Liver QuestionsDocument44 pagesThe Physiology of The GIT and The Liver QuestionsDonkeyManNo ratings yet
- Palliative Care HandbookDocument82 pagesPalliative Care HandbookDonkeyManNo ratings yet
- Base Excess (Be) Measure of Metabolic Acid-Base Status: Dr. David LynessDocument1 pageBase Excess (Be) Measure of Metabolic Acid-Base Status: Dr. David LynessDonkeyManNo ratings yet
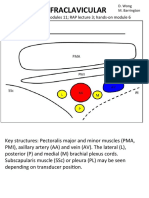
- Infraclavicular: Toolbox: Online Modules 11 RAP Lecture 3 Hands - On Module 6Document4 pagesInfraclavicular: Toolbox: Online Modules 11 RAP Lecture 3 Hands - On Module 6DonkeyManNo ratings yet
- Cholinergic Agents: Cholinergic Receptors Types of Receptor Muscarinic Receptor Nicotinic ReceptorDocument4 pagesCholinergic Agents: Cholinergic Receptors Types of Receptor Muscarinic Receptor Nicotinic ReceptorDonkeyManNo ratings yet
- Student Overview: # Question and Answer Choices Points CategoriesDocument17 pagesStudent Overview: # Question and Answer Choices Points CategoriesGabriel AndradeNo ratings yet
- Chapter 1 QuestionsDocument3 pagesChapter 1 QuestionsCarina Jaksha MarcianoNo ratings yet
- GMC Policy Benefits ChartDocument3 pagesGMC Policy Benefits ChartpankajgujjarNo ratings yet
- Pharmacology MnemonicsDocument26 pagesPharmacology MnemonicsArthur JamesNo ratings yet
- Editors, Asim Kurjak, Frank A. Chervenak. - Donald School Textbook of Ultrasound in Obstetrics and Gynecology (2011., Jaypee Bros. Medical Publ.) PDFDocument1,035 pagesEditors, Asim Kurjak, Frank A. Chervenak. - Donald School Textbook of Ultrasound in Obstetrics and Gynecology (2011., Jaypee Bros. Medical Publ.) PDFRaluca Haba100% (1)
- Community Assessment Paper Pasco County - Omar Shaout 2Document8 pagesCommunity Assessment Paper Pasco County - Omar Shaout 2api-679742031No ratings yet
- EAU Guidelines On Urolithiasis 2023Document120 pagesEAU Guidelines On Urolithiasis 2023luonganhsiNo ratings yet
- CNA Body Mechanics Bed Making Comfort CareDocument32 pagesCNA Body Mechanics Bed Making Comfort CareFaith VaughnNo ratings yet
- Virus ClassificationDocument2 pagesVirus ClassificationJoshua PrinceNo ratings yet
- Congenital HypothyroidismDocument21 pagesCongenital HypothyroidismIkhsan Nurkholis SudradjatNo ratings yet
- Shock ManagementDocument17 pagesShock ManagementAmare EshetieNo ratings yet
- Reasonable Accommodation Forms2Document4 pagesReasonable Accommodation Forms2DBHAAdminNo ratings yet
- Study Guide PCE Jason Shane Amanda MrsicDocument117 pagesStudy Guide PCE Jason Shane Amanda MrsicShora Jari0% (1)
- Case Report OADocument31 pagesCase Report OAmarindadaNo ratings yet
- Temblor de HolmesDocument7 pagesTemblor de HolmesIan Luis Flores SaavedraNo ratings yet
- Pereira Nunes Et Al 2023 Novel Arthrogryposis Multiplex Congenita Presentation in A Newborn With Pierpont SyndromeDocument5 pagesPereira Nunes Et Al 2023 Novel Arthrogryposis Multiplex Congenita Presentation in A Newborn With Pierpont SyndromeRafii KhairuddinNo ratings yet
- Pre-Travel Questionnaire Form: Section A - Traveler InformationDocument2 pagesPre-Travel Questionnaire Form: Section A - Traveler InformationNikhil JoharNo ratings yet
- NURSING PROCEDURES RT GI SYSTEMDocument226 pagesNURSING PROCEDURES RT GI SYSTEMMika SaldanaNo ratings yet
- Psychopharmacology Is The Study of Drug-Induced Changes in Mood, Sensation, ThinkingDocument5 pagesPsychopharmacology Is The Study of Drug-Induced Changes in Mood, Sensation, Thinking0921pyNo ratings yet
- Assessment of Nutritional Status Based On Strongkids Tool in Iranian Hospitalized ChildrenDocument7 pagesAssessment of Nutritional Status Based On Strongkids Tool in Iranian Hospitalized Childrenfarah febriyantiNo ratings yet
- Burning Mouth SyndromeDocument3 pagesBurning Mouth SyndromeYohana RebeccaNo ratings yet
- Grabovoi NumbersDocument29 pagesGrabovoi Numberssillyminds100% (3)
- Immunology: Historical Perspective and TheoriesDocument12 pagesImmunology: Historical Perspective and TheoriesROJA BINTE AMINNo ratings yet
- Breast ScreeningDocument76 pagesBreast ScreeningBenny KurniawanNo ratings yet
- 10 Myths About SchizophreniaDocument11 pages10 Myths About SchizophreniaQuennie Marie Moreno VillanuevaNo ratings yet
- RhabdovirusDocument74 pagesRhabdovirustummalapalli venkateswara raoNo ratings yet
- Diabetes Related CKD 2Document1 pageDiabetes Related CKD 2Jia-PeiWuNo ratings yet



















































































































Download as pdf or txt
You might also like
- Hippo Emergency Medicine Board Review - Cram Section - MnemonicsDocument1 pageHippo Emergency Medicine Board Review - Cram Section - MnemonicslotskiNo ratings yet
- OCCUPATIONAL DISEASES Clinical cases 2015 англ 2Document28 pagesOCCUPATIONAL DISEASES Clinical cases 2015 англ 2kjk100% (1)
- MCAT Biology Complete OutlinesDocument34 pagesMCAT Biology Complete OutlinesJacob Mikhail90% (10)
- Gastrointestinal System (Letu Da) PDFDocument74 pagesGastrointestinal System (Letu Da) PDFNafiul Islam100% (4)
- Phys Offluidselectrolytes7 121107201529 Phpapp02Document38 pagesPhys Offluidselectrolytes7 121107201529 Phpapp02Rehab weridaNo ratings yet
- Cardiovascular System: Department of Biochemistry. Faculty of Medicine, UNHAS Rosdiana NatzirDocument68 pagesCardiovascular System: Department of Biochemistry. Faculty of Medicine, UNHAS Rosdiana NatzirikhyNo ratings yet
- Physiology RenalDocument14 pagesPhysiology Renalahmedsalah565vvvNo ratings yet
- PKPD Esterase1Document2 pagesPKPD Esterase1أسعد حسنانNo ratings yet
- Bioch CL 7. Enzime Utilizate in Diagnostic 20-21 (R+e)Document44 pagesBioch CL 7. Enzime Utilizate in Diagnostic 20-21 (R+e)Andrea ModestieNo ratings yet
- 2024 - Aula Grupo - Metabolismo Colesterol e Ácidos Biliares 2Document42 pages2024 - Aula Grupo - Metabolismo Colesterol e Ácidos Biliares 2MavumeNo ratings yet
- Biochemistry of Cardiovascular SystemDocument113 pagesBiochemistry of Cardiovascular SystemNindy75% (4)
- Enzyme IsoenzymesDocument60 pagesEnzyme IsoenzymesSrishti GoenkaNo ratings yet
- I So EnzymesDocument31 pagesI So Enzymesalinaibrar80No ratings yet
- Answers of Exam Ques.Document3 pagesAnswers of Exam Ques.Sonali SehrawatNo ratings yet
- Alcoholics - Episode 289 - Step 1, Step 2CK, Step 3Document2 pagesAlcoholics - Episode 289 - Step 1, Step 2CK, Step 3dhanwin shettyNo ratings yet
- Fluids and Electrolytes Fluids and Electrolytes Acids, Bases, and Acids, Bases, and PH PH By: By: SMM SMM,, RN RN MD MD By: By: SMM SMM,, RN RN MD MDDocument50 pagesFluids and Electrolytes Fluids and Electrolytes Acids, Bases, and Acids, Bases, and PH PH By: By: SMM SMM,, RN RN MD MD By: By: SMM SMM,, RN RN MD MDRose AlmanzorNo ratings yet
- Cholesteril MetabolismDocument54 pagesCholesteril MetabolismAna AbuladzeNo ratings yet
- Liquidos y Electrolitos 2016Document5 pagesLiquidos y Electrolitos 2016MARIA JOSE MEDINA JAIMES100% (1)
- Bone SemeioticaDocument11 pagesBone SemeioticaFrancesco De PalmaNo ratings yet
- Body Fluids: M. Alif Prizarky 04011381419173 GammaDocument7 pagesBody Fluids: M. Alif Prizarky 04011381419173 GammaAlviss RmidNo ratings yet
- EnzymesDocument18 pagesEnzymesRichard PoonNo ratings yet
- Kenzu B, (MD, Asst - Professor of Surgery)Document40 pagesKenzu B, (MD, Asst - Professor of Surgery)kenzu bedruNo ratings yet
- Body Fluids and Blood - HUMAN PHYSIOLOGYDocument29 pagesBody Fluids and Blood - HUMAN PHYSIOLOGYSodeinde SimeonNo ratings yet
- Explorarea Echilibrului Hidro - ElectroliticDocument77 pagesExplorarea Echilibrului Hidro - ElectroliticCopăcel AlexandraNo ratings yet
- Lecture EnzymesDocument45 pagesLecture EnzymesJohn Alfrey Dondiego PuebloNo ratings yet
- Gangguan Dan Keseimbangan Cairan Dan ElektrolitDocument37 pagesGangguan Dan Keseimbangan Cairan Dan ElektrolitFyana PutriNo ratings yet
- Lec. 3 - Fluid and ElectrolyteDocument16 pagesLec. 3 - Fluid and Electrolyteمجيب سلطانNo ratings yet
- 10 Pyruvate Oxid Tricarb Acid Cycle Notes GanapathyDocument7 pages10 Pyruvate Oxid Tricarb Acid Cycle Notes Ganapathykalps.galleryNo ratings yet
- Biochemistry of CVSDocument311 pagesBiochemistry of CVSAsne ManNo ratings yet
- Metabolic Aspect of CVSDocument25 pagesMetabolic Aspect of CVSsamar yousif mohamedNo ratings yet
- CH 18 Cholesterol Metabolism: Biochem Block 3 NotesDocument38 pagesCH 18 Cholesterol Metabolism: Biochem Block 3 NotesJoseph KimNo ratings yet
- Cardiac EnzymesDocument20 pagesCardiac Enzymesstrypto123aaaNo ratings yet
- TCA CycleDocument47 pagesTCA CycleMita SeptianiNo ratings yet
- 04 Metabolisme Xenobiotik NWDocument36 pages04 Metabolisme Xenobiotik NWDesy NataliaNo ratings yet
- Lecture 05. Lipid Metabolism-2. Lipogenesis. Metabolism of Cholesterol and Ketone Bodies.Document33 pagesLecture 05. Lipid Metabolism-2. Lipogenesis. Metabolism of Cholesterol and Ketone Bodies.Віталій Михайлович НечипорукNo ratings yet
- Medical-Surgical Nursing 1Document28 pagesMedical-Surgical Nursing 1Maui Ting100% (1)
- PeroxisomesDocument2 pagesPeroxisomesIndigoSilverNo ratings yet
- Organophosphates (OPs) and Carbamates (CMS)Document15 pagesOrganophosphates (OPs) and Carbamates (CMS)مصطفى أحمدNo ratings yet
- Clinical EnzymologyDocument23 pagesClinical EnzymologyKishore KaranNo ratings yet
- FluidslectureDocument26 pagesFluidslectureIgor StefanetNo ratings yet
- Chapter 18 Lippincott BiochemistryDocument62 pagesChapter 18 Lippincott BiochemistryMeysam SajjadiNo ratings yet
- 228 Carbohydrate MetabolismDocument43 pages228 Carbohydrate MetabolismAmanullahNo ratings yet
- FLuid & Elect & Acid Base & Surg. Nutr.Document24 pagesFLuid & Elect & Acid Base & Surg. Nutr.anon_761270640No ratings yet
- Fluid BalanceDocument30 pagesFluid BalanceBadrun DalangNo ratings yet
- Funda Fluids Elect.Document26 pagesFunda Fluids Elect.j UNo ratings yet
- Body Fluids and ElectrolytesDocument42 pagesBody Fluids and ElectrolytesQusaiBadr100% (1)
- 15.fluid BalanceDocument48 pages15.fluid BalanceImtiaz AhmadNo ratings yet
- Student Book 2Document101 pagesStudent Book 2helena coelho odaNo ratings yet
- Physiology - BSDocument14 pagesPhysiology - BSkep1313No ratings yet
- Cholesterol and Steroid MetabolismDocument17 pagesCholesterol and Steroid MetabolismMarkyNo ratings yet
- Biochem Questions SlidesDocument46 pagesBiochem Questions SlidesTelesha Zabie50% (2)
- Phase: I Hydrolysis of XenobioticsDocument37 pagesPhase: I Hydrolysis of XenobioticsSunilNo ratings yet
- Fluid and Electrolyte TherapyDocument23 pagesFluid and Electrolyte TherapyJamal ArizonaNo ratings yet
- Clinical Enzymology 2Document55 pagesClinical Enzymology 2reuben kwotaNo ratings yet
- MI - 11 - Ciclo de Cori, Creatina Fosfato y Ciclos Energéticos Del MúsculoDocument39 pagesMI - 11 - Ciclo de Cori, Creatina Fosfato y Ciclos Energéticos Del MúsculoANDRÉS FELIPE VALDERRAMA BAEZNo ratings yet
- Fluids and Electrolytes Part 1Document4 pagesFluids and Electrolytes Part 1baraderoayyah41No ratings yet
- Causes HyperlactemiaDocument5 pagesCauses HyperlactemiaArvin ReinaldoNo ratings yet
- Carbohydrate Metabolism 2Document41 pagesCarbohydrate Metabolism 2Shimmering MoonNo ratings yet
- Disorders of Potassium Metabolism PresentationDocument20 pagesDisorders of Potassium Metabolism PresentationSolomon Fallah Foa SandyNo ratings yet
- Chapter 17 18 Cholesterol Metabolism and Protaglandins b7990672Document18 pagesChapter 17 18 Cholesterol Metabolism and Protaglandins b7990672toumeh.halaNo ratings yet
- Fluid and Electrolytes: Ma. Medine L. Amorsolo RN ManDocument29 pagesFluid and Electrolytes: Ma. Medine L. Amorsolo RN ManMichael Baylon Dueñas100% (1)
- Physiol 93 B3Document1 pagePhysiol 93 B3DonkeyManNo ratings yet
- CEACCP - KetamineDocument5 pagesCEACCP - KetamineDonkeyManNo ratings yet
- CEACCP - Latex AllergyDocument4 pagesCEACCP - Latex AllergyDonkeyManNo ratings yet
- CEACCP - Illegal Substances in Anaesthetic and Intensive Care PracticesDocument5 pagesCEACCP - Illegal Substances in Anaesthetic and Intensive Care PracticesDonkeyManNo ratings yet
- Pharmacodynamics, Drug Action Targets, PharmacogeneticsDocument21 pagesPharmacodynamics, Drug Action Targets, PharmacogeneticsDonkeyManNo ratings yet
- Cellular Physiology SAQsDocument1 pageCellular Physiology SAQsDonkeyManNo ratings yet
- Define The Mechanisms of Action and Adverse Effects of Metoprolol, GTN, and Diltiazem When Used To Manage MIDocument2 pagesDefine The Mechanisms of Action and Adverse Effects of Metoprolol, GTN, and Diltiazem When Used To Manage MIDonkeyManNo ratings yet
- Pharm 02 A11Document4 pagesPharm 02 A11DonkeyManNo ratings yet
- CEACCP - Intrathecal Opioids in The Management of Acute Postoperative PainDocument5 pagesCEACCP - Intrathecal Opioids in The Management of Acute Postoperative PainDonkeyManNo ratings yet
- Pharm 00 B15Document2 pagesPharm 00 B15DonkeyManNo ratings yet
- Outline The Physiological Consequences of Hyperosmolar Diabetic KetoacidosisDocument2 pagesOutline The Physiological Consequences of Hyperosmolar Diabetic KetoacidosisDonkeyManNo ratings yet
- Pharm 02 A10Document2 pagesPharm 02 A10DonkeyManNo ratings yet
- Pharm 00 A15Document2 pagesPharm 00 A15DonkeyManNo ratings yet
- Compare and Contrast Neostigmine and The Organophosphate CompoundsDocument1 pageCompare and Contrast Neostigmine and The Organophosphate CompoundsDonkeyManNo ratings yet
- Pharm 00 B11Document1 pagePharm 00 B11DonkeyManNo ratings yet
- Pharm 00 B14Document2 pagesPharm 00 B14DonkeyManNo ratings yet
- Pharm 00 A12Document1 pagePharm 00 A12DonkeyManNo ratings yet
- Compare and Contrast Atropine and Glycopyrulate, and Discuss The Clinical ImplicationsDocument2 pagesCompare and Contrast Atropine and Glycopyrulate, and Discuss The Clinical ImplicationsDonkeyManNo ratings yet
- Compare and Contrast The Pharamcology of Ephedrine and NoradrenalineDocument1 pageCompare and Contrast The Pharamcology of Ephedrine and NoradrenalineDonkeyManNo ratings yet
- Pharm 00 A9Document2 pagesPharm 00 A9DonkeyManNo ratings yet
- Compare and Contrast The Pharmacology of Esmolol and PropanololDocument1 pageCompare and Contrast The Pharmacology of Esmolol and PropanololDonkeyManNo ratings yet
- FS Antimicrobial Dosing Obesity AMS Updates Issue4 - Nov2018Document4 pagesFS Antimicrobial Dosing Obesity AMS Updates Issue4 - Nov2018DonkeyManNo ratings yet
- Comparative Pharmacokinetics of Fentanyl and Alfentanil: Br. J. Anaesth. (1982), 54, 871Document7 pagesComparative Pharmacokinetics of Fentanyl and Alfentanil: Br. J. Anaesth. (1982), 54, 871DonkeyManNo ratings yet
- VOLATILEAGENTSDocument4 pagesVOLATILEAGENTSDonkeyManNo ratings yet
- The Physiology of The GIT and The Liver QuestionsDocument44 pagesThe Physiology of The GIT and The Liver QuestionsDonkeyManNo ratings yet
- Palliative Care HandbookDocument82 pagesPalliative Care HandbookDonkeyManNo ratings yet
- Base Excess (Be) Measure of Metabolic Acid-Base Status: Dr. David LynessDocument1 pageBase Excess (Be) Measure of Metabolic Acid-Base Status: Dr. David LynessDonkeyManNo ratings yet
- Infraclavicular: Toolbox: Online Modules 11 RAP Lecture 3 Hands - On Module 6Document4 pagesInfraclavicular: Toolbox: Online Modules 11 RAP Lecture 3 Hands - On Module 6DonkeyManNo ratings yet
- Cholinergic Agents: Cholinergic Receptors Types of Receptor Muscarinic Receptor Nicotinic ReceptorDocument4 pagesCholinergic Agents: Cholinergic Receptors Types of Receptor Muscarinic Receptor Nicotinic ReceptorDonkeyManNo ratings yet
- Student Overview: # Question and Answer Choices Points CategoriesDocument17 pagesStudent Overview: # Question and Answer Choices Points CategoriesGabriel AndradeNo ratings yet
- Chapter 1 QuestionsDocument3 pagesChapter 1 QuestionsCarina Jaksha MarcianoNo ratings yet
- GMC Policy Benefits ChartDocument3 pagesGMC Policy Benefits ChartpankajgujjarNo ratings yet
- Pharmacology MnemonicsDocument26 pagesPharmacology MnemonicsArthur JamesNo ratings yet
- Editors, Asim Kurjak, Frank A. Chervenak. - Donald School Textbook of Ultrasound in Obstetrics and Gynecology (2011., Jaypee Bros. Medical Publ.) PDFDocument1,035 pagesEditors, Asim Kurjak, Frank A. Chervenak. - Donald School Textbook of Ultrasound in Obstetrics and Gynecology (2011., Jaypee Bros. Medical Publ.) PDFRaluca Haba100% (1)
- Community Assessment Paper Pasco County - Omar Shaout 2Document8 pagesCommunity Assessment Paper Pasco County - Omar Shaout 2api-679742031No ratings yet
- EAU Guidelines On Urolithiasis 2023Document120 pagesEAU Guidelines On Urolithiasis 2023luonganhsiNo ratings yet
- CNA Body Mechanics Bed Making Comfort CareDocument32 pagesCNA Body Mechanics Bed Making Comfort CareFaith VaughnNo ratings yet
- Virus ClassificationDocument2 pagesVirus ClassificationJoshua PrinceNo ratings yet
- Congenital HypothyroidismDocument21 pagesCongenital HypothyroidismIkhsan Nurkholis SudradjatNo ratings yet
- Shock ManagementDocument17 pagesShock ManagementAmare EshetieNo ratings yet
- Reasonable Accommodation Forms2Document4 pagesReasonable Accommodation Forms2DBHAAdminNo ratings yet
- Study Guide PCE Jason Shane Amanda MrsicDocument117 pagesStudy Guide PCE Jason Shane Amanda MrsicShora Jari0% (1)
- Case Report OADocument31 pagesCase Report OAmarindadaNo ratings yet
- Temblor de HolmesDocument7 pagesTemblor de HolmesIan Luis Flores SaavedraNo ratings yet
- Pereira Nunes Et Al 2023 Novel Arthrogryposis Multiplex Congenita Presentation in A Newborn With Pierpont SyndromeDocument5 pagesPereira Nunes Et Al 2023 Novel Arthrogryposis Multiplex Congenita Presentation in A Newborn With Pierpont SyndromeRafii KhairuddinNo ratings yet
- Pre-Travel Questionnaire Form: Section A - Traveler InformationDocument2 pagesPre-Travel Questionnaire Form: Section A - Traveler InformationNikhil JoharNo ratings yet
- NURSING PROCEDURES RT GI SYSTEMDocument226 pagesNURSING PROCEDURES RT GI SYSTEMMika SaldanaNo ratings yet
- Psychopharmacology Is The Study of Drug-Induced Changes in Mood, Sensation, ThinkingDocument5 pagesPsychopharmacology Is The Study of Drug-Induced Changes in Mood, Sensation, Thinking0921pyNo ratings yet
- Assessment of Nutritional Status Based On Strongkids Tool in Iranian Hospitalized ChildrenDocument7 pagesAssessment of Nutritional Status Based On Strongkids Tool in Iranian Hospitalized Childrenfarah febriyantiNo ratings yet
- Burning Mouth SyndromeDocument3 pagesBurning Mouth SyndromeYohana RebeccaNo ratings yet
- Grabovoi NumbersDocument29 pagesGrabovoi Numberssillyminds100% (3)
- Immunology: Historical Perspective and TheoriesDocument12 pagesImmunology: Historical Perspective and TheoriesROJA BINTE AMINNo ratings yet
- Breast ScreeningDocument76 pagesBreast ScreeningBenny KurniawanNo ratings yet
- 10 Myths About SchizophreniaDocument11 pages10 Myths About SchizophreniaQuennie Marie Moreno VillanuevaNo ratings yet
- RhabdovirusDocument74 pagesRhabdovirustummalapalli venkateswara raoNo ratings yet
- Diabetes Related CKD 2Document1 pageDiabetes Related CKD 2Jia-PeiWuNo ratings yet