
Isbel
Isbel
You might also like
- TVP-2020-1112 Managing Feline Urethral ObstructionDocument6 pagesTVP-2020-1112 Managing Feline Urethral ObstructionLucas Dos Santos MacedoNo ratings yet
- Glomerulonefritis Primaria Medicine 2015Document6 pagesGlomerulonefritis Primaria Medicine 2015Francisco Rebollar GarduñoNo ratings yet
- Glomerulopatías PrimariasDocument8 pagesGlomerulopatías PrimariasGSENo ratings yet
- Clinical Presentation & Management of Glomerular Diseases: Hematuria, Nephritic & Nephrotic SyndromeDocument4 pagesClinical Presentation & Management of Glomerular Diseases: Hematuria, Nephritic & Nephrotic SyndromeMutiara FauzaNo ratings yet
- Glomerular DiseasesDocument5 pagesGlomerular DiseasesAdrian ZapataNo ratings yet
- Nephrotic Syndrome ComplicationsDocument16 pagesNephrotic Syndrome ComplicationsBeatri AyuzaNo ratings yet
- Renal BiopsyDocument4 pagesRenal BiopsyDeshan AdikariNo ratings yet
- Calcium Dobesilate in Acute Hemorrhoids 2001Document7 pagesCalcium Dobesilate in Acute Hemorrhoids 2001furqanahmedooo123No ratings yet
- Drug-Induced Kidney Disease: ArticleDocument11 pagesDrug-Induced Kidney Disease: Articledwi harisNo ratings yet
- Chronic Kidney Disease and Pregnancy: Medical Complications of Pregnancy: Clinical Expert SeriesDocument13 pagesChronic Kidney Disease and Pregnancy: Medical Complications of Pregnancy: Clinical Expert SeriesIndah95No ratings yet
- Insuficiencia Renal CronicaDocument13 pagesInsuficiencia Renal CronicaCarlos DNo ratings yet
- Serum and Urine Biomarkers of Kidney Disease.Document8 pagesSerum and Urine Biomarkers of Kidney Disease.Andronic GeorgeNo ratings yet
- Evaluation of Chronic Renal Disease, A Staged ApproachDocument8 pagesEvaluation of Chronic Renal Disease, A Staged Approachtaner_soysurenNo ratings yet
- Review and Update of Benign PRDocument6 pagesReview and Update of Benign PRAgung KaryawinaraNo ratings yet
- Present and Future Drug TreatmentsDocument18 pagesPresent and Future Drug Treatmentsagustinaw1981No ratings yet
- Lasificación Histopatológica de La Glomerulonefritis Asociada A ANCADocument9 pagesLasificación Histopatológica de La Glomerulonefritis Asociada A ANCASaid SanchezNo ratings yet
- Nash: Advances in Evaluation and Management: Rakesh K TandonDocument6 pagesNash: Advances in Evaluation and Management: Rakesh K TandonSrinivas GokulnathNo ratings yet
- 2 Nephrotox Associated With Novel Anticancer AgentsDocument18 pages2 Nephrotox Associated With Novel Anticancer AgentsNourNo ratings yet
- Agn Three Fold BrochureDocument4 pagesAgn Three Fold BrochureKristine JamilleNo ratings yet
- 28-Year-Old Man With Crohn Disease and Hematuria: Residents ' ClinicDocument5 pages28-Year-Old Man With Crohn Disease and Hematuria: Residents ' ClinicDesi HutapeaNo ratings yet
- Medicina 55 00365Document21 pagesMedicina 55 00365Sundas EjazNo ratings yet
- Acute GlomerulonephritisDocument18 pagesAcute GlomerulonephritisdanielaNo ratings yet
- Onconephrology: Update in Anticancer Drug-Related NephrotoxicityDocument13 pagesOnconephrology: Update in Anticancer Drug-Related NephrotoxicityFreddy Shanner Chávez VásquezNo ratings yet
- GinjalDocument11 pagesGinjalOneng IfayaniNo ratings yet
- Seminar: Kamyar Kalantar-Zadeh, Tazeen H Jafar, Dorothea Nitsch, Brendon L Neuen, Vlado PerkovicDocument17 pagesSeminar: Kamyar Kalantar-Zadeh, Tazeen H Jafar, Dorothea Nitsch, Brendon L Neuen, Vlado PerkovicJack JackNo ratings yet
- Nephrotic Syndrome Review 2024Document10 pagesNephrotic Syndrome Review 2024Jonathan MorenoNo ratings yet
- Drug Induced Tubular InjuryDocument8 pagesDrug Induced Tubular InjuryRania T. SabriNo ratings yet
- Acute Renal FailureDocument14 pagesAcute Renal FailuredrtpkNo ratings yet
- Calcium Dobesilate in Symptomatic Treatment of Hemorrhoidal Disease: An Interventional StudyDocument3 pagesCalcium Dobesilate in Symptomatic Treatment of Hemorrhoidal Disease: An Interventional StudyN R Reddy HemanthNo ratings yet
- Chronic Kidney Disease and Acute Kidney InjuryDocument46 pagesChronic Kidney Disease and Acute Kidney Injurydikiprestya391No ratings yet
- Cleveland Clinic Journal of Medicine 2003 Kashif 535 7Document9 pagesCleveland Clinic Journal of Medicine 2003 Kashif 535 7shiloinNo ratings yet
- Review of Refractory Lupus NephritisDocument12 pagesReview of Refractory Lupus NephritisDeddy WijayaNo ratings yet
- Oftal Case StudyDocument11 pagesOftal Case StudyMohamad RaisNo ratings yet
- Drug-Induced Nephrotoxicity: Gabriel Teixeira Montezuma Sales Renato Demarchi ForestoDocument9 pagesDrug-Induced Nephrotoxicity: Gabriel Teixeira Montezuma Sales Renato Demarchi ForestoCecep Darwis MuttaqinNo ratings yet
- Renal DiseasesDocument26 pagesRenal DiseasesismailcemNo ratings yet
- Diagnosis and Management of Acute Pancreatitis andDocument11 pagesDiagnosis and Management of Acute Pancreatitis andMarcelitaTaliaDuwiriNo ratings yet
- Chronic PancreatitisDocument8 pagesChronic PancreatitisSanjaya SenevirathneNo ratings yet
- Proteinuria in Diabetic Kidney Disease A MechanisticDocument15 pagesProteinuria in Diabetic Kidney Disease A Mechanisticmutiara nurzaniNo ratings yet
- Management of Patients With Nephrotic Syndrome: Sophie de Seigneux, Pierre-Yves MartinDocument7 pagesManagement of Patients With Nephrotic Syndrome: Sophie de Seigneux, Pierre-Yves MartinGarit Hapsari KiranaNo ratings yet
- CKD Lancet 2021Document17 pagesCKD Lancet 2021Fabiola AlonsoNo ratings yet
- Case Report of Acute and Chronic Interstitial NephritisDocument10 pagesCase Report of Acute and Chronic Interstitial NephritisDoncyNo ratings yet
- Artigotutoria PDFDocument12 pagesArtigotutoria PDFZARA BATISTANo ratings yet
- Chronic Renal Failure and Uremia: ObjectivesDocument7 pagesChronic Renal Failure and Uremia: ObjectivesNurulSyaidahNo ratings yet
- Headache: General PrinciplesDocument5 pagesHeadache: General PrinciplesAl Glen EgarleNo ratings yet
- 1.acute Kidney InjuryDocument3 pages1.acute Kidney InjuryIan CruzNo ratings yet
- Renal Disease 2023Document9 pagesRenal Disease 2023MaeNo ratings yet
- Biomarcadores en IRC Temprana en Gatos 2013Document6 pagesBiomarcadores en IRC Temprana en Gatos 2013Wilson Enrique Guerrero JojoaNo ratings yet
- Renal CaseDocument3 pagesRenal CaseAndy BiersackNo ratings yet
- Review On Treatment of Gout & HyperuricemiaDocument11 pagesReview On Treatment of Gout & HyperuricemiaMirza ProthikhaNo ratings yet
- ACG Clinical Guideline: Chronic PancreatitisDocument18 pagesACG Clinical Guideline: Chronic PancreatitisRene CordovaNo ratings yet
- Piis0085253815527324 PDFDocument5 pagesPiis0085253815527324 PDFdodong skyroseNo ratings yet
- Gagal Ginjal Akut - Bhs InggrisDocument27 pagesGagal Ginjal Akut - Bhs InggrisAgustinusNo ratings yet
- Nefropatia Diabetica Trayectorias NATUREDocument11 pagesNefropatia Diabetica Trayectorias NATURERAUL ALMYR MONTES GONZALEZNo ratings yet
- 2018 Tto Del SN CorticoresistenteDocument11 pages2018 Tto Del SN CorticoresistenteJeff Daniel Landauro PanayNo ratings yet
- RevDiabeticStud 12 087Document23 pagesRevDiabeticStud 12 087Win by the ForceNo ratings yet
- Hussein 2009Document4 pagesHussein 2009djsuraz0No ratings yet
- Acute Kidney Injury: Current Concepts and New Insights: Key WordsDocument5 pagesAcute Kidney Injury: Current Concepts and New Insights: Key WordsIHNo ratings yet
- The Perfect Neutropenic Diet Cookbook; The Complete Nutrition Guide To Reinstating Overall Health For General Wellness With Delectable And Nourishing RecipesFrom EverandThe Perfect Neutropenic Diet Cookbook; The Complete Nutrition Guide To Reinstating Overall Health For General Wellness With Delectable And Nourishing RecipesNo ratings yet
- Hypoxic Ischaemic Encephalopathy HIE AsphyxiaDocument6 pagesHypoxic Ischaemic Encephalopathy HIE AsphyxiaCaity YoungNo ratings yet
- A I - E M: Drenal Nsufficiency Mergency AnagementDocument12 pagesA I - E M: Drenal Nsufficiency Mergency AnagementCaity YoungNo ratings yet
- Rhumatologie-Pediatrique FRDocument4 pagesRhumatologie-Pediatrique FRCaity YoungNo ratings yet
- Afoem Sample Paper Stage B Written Exam Paper 7Document46 pagesAfoem Sample Paper Stage B Written Exam Paper 7Caity YoungNo ratings yet
- Afoem Sample Paper Stage B Written Exam Paper 7Document43 pagesAfoem Sample Paper Stage B Written Exam Paper 7Caity YoungNo ratings yet
- 2014 A Health Professionals Guide To Using The ChartsDocument14 pages2014 A Health Professionals Guide To Using The ChartsCaity YoungNo ratings yet
- CP2 Learning ObjectivesDocument992 pagesCP2 Learning ObjectivesCaity YoungNo ratings yet
- Fluid Calculator DKADocument3 pagesFluid Calculator DKACaity YoungNo ratings yet
- SSHADESS HandoutDocument1 pageSSHADESS HandoutCaity YoungNo ratings yet
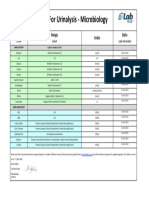
- Reference Ranges For Urinalysis - Microbiology: Test Range Units DateDocument1 pageReference Ranges For Urinalysis - Microbiology: Test Range Units DateCaity YoungNo ratings yet
- 2 - McDonald - Examples - of - Unhelpful - ThoughtsDocument2 pages2 - McDonald - Examples - of - Unhelpful - ThoughtsCaity YoungNo ratings yet
- SpirometryDocument17 pagesSpirometryCaity YoungNo ratings yet
- Correspondence: Classifi Cation of CFTR Mutation ClassesDocument2 pagesCorrespondence: Classifi Cation of CFTR Mutation ClassesCaity YoungNo ratings yet
- Genetic Basis For Congenital Heart Disease: Revisited: CirculationDocument59 pagesGenetic Basis For Congenital Heart Disease: Revisited: CirculationCaity YoungNo ratings yet
- ToF ScriptDocument6 pagesToF ScriptCaity YoungNo ratings yet
- Part 2: Male Reproductive System: Normal Physiology and StructureDocument30 pagesPart 2: Male Reproductive System: Normal Physiology and StructureCaity YoungNo ratings yet
- 4-5 GlomerularDiseasesDocument21 pages4-5 GlomerularDiseasesCaity YoungNo ratings yet
- Sore Throat: Navigating The Differential DiagnosisDocument7 pagesSore Throat: Navigating The Differential DiagnosisCaity YoungNo ratings yet












































































Download as pdf or txt
You might also like
- TVP-2020-1112 Managing Feline Urethral ObstructionDocument6 pagesTVP-2020-1112 Managing Feline Urethral ObstructionLucas Dos Santos MacedoNo ratings yet
- Glomerulonefritis Primaria Medicine 2015Document6 pagesGlomerulonefritis Primaria Medicine 2015Francisco Rebollar GarduñoNo ratings yet
- Glomerulopatías PrimariasDocument8 pagesGlomerulopatías PrimariasGSENo ratings yet
- Clinical Presentation & Management of Glomerular Diseases: Hematuria, Nephritic & Nephrotic SyndromeDocument4 pagesClinical Presentation & Management of Glomerular Diseases: Hematuria, Nephritic & Nephrotic SyndromeMutiara FauzaNo ratings yet
- Glomerular DiseasesDocument5 pagesGlomerular DiseasesAdrian ZapataNo ratings yet
- Nephrotic Syndrome ComplicationsDocument16 pagesNephrotic Syndrome ComplicationsBeatri AyuzaNo ratings yet
- Renal BiopsyDocument4 pagesRenal BiopsyDeshan AdikariNo ratings yet
- Calcium Dobesilate in Acute Hemorrhoids 2001Document7 pagesCalcium Dobesilate in Acute Hemorrhoids 2001furqanahmedooo123No ratings yet
- Drug-Induced Kidney Disease: ArticleDocument11 pagesDrug-Induced Kidney Disease: Articledwi harisNo ratings yet
- Chronic Kidney Disease and Pregnancy: Medical Complications of Pregnancy: Clinical Expert SeriesDocument13 pagesChronic Kidney Disease and Pregnancy: Medical Complications of Pregnancy: Clinical Expert SeriesIndah95No ratings yet
- Insuficiencia Renal CronicaDocument13 pagesInsuficiencia Renal CronicaCarlos DNo ratings yet
- Serum and Urine Biomarkers of Kidney Disease.Document8 pagesSerum and Urine Biomarkers of Kidney Disease.Andronic GeorgeNo ratings yet
- Evaluation of Chronic Renal Disease, A Staged ApproachDocument8 pagesEvaluation of Chronic Renal Disease, A Staged Approachtaner_soysurenNo ratings yet
- Review and Update of Benign PRDocument6 pagesReview and Update of Benign PRAgung KaryawinaraNo ratings yet
- Present and Future Drug TreatmentsDocument18 pagesPresent and Future Drug Treatmentsagustinaw1981No ratings yet
- Lasificación Histopatológica de La Glomerulonefritis Asociada A ANCADocument9 pagesLasificación Histopatológica de La Glomerulonefritis Asociada A ANCASaid SanchezNo ratings yet
- Nash: Advances in Evaluation and Management: Rakesh K TandonDocument6 pagesNash: Advances in Evaluation and Management: Rakesh K TandonSrinivas GokulnathNo ratings yet
- 2 Nephrotox Associated With Novel Anticancer AgentsDocument18 pages2 Nephrotox Associated With Novel Anticancer AgentsNourNo ratings yet
- Agn Three Fold BrochureDocument4 pagesAgn Three Fold BrochureKristine JamilleNo ratings yet
- 28-Year-Old Man With Crohn Disease and Hematuria: Residents ' ClinicDocument5 pages28-Year-Old Man With Crohn Disease and Hematuria: Residents ' ClinicDesi HutapeaNo ratings yet
- Medicina 55 00365Document21 pagesMedicina 55 00365Sundas EjazNo ratings yet
- Acute GlomerulonephritisDocument18 pagesAcute GlomerulonephritisdanielaNo ratings yet
- Onconephrology: Update in Anticancer Drug-Related NephrotoxicityDocument13 pagesOnconephrology: Update in Anticancer Drug-Related NephrotoxicityFreddy Shanner Chávez VásquezNo ratings yet
- GinjalDocument11 pagesGinjalOneng IfayaniNo ratings yet
- Seminar: Kamyar Kalantar-Zadeh, Tazeen H Jafar, Dorothea Nitsch, Brendon L Neuen, Vlado PerkovicDocument17 pagesSeminar: Kamyar Kalantar-Zadeh, Tazeen H Jafar, Dorothea Nitsch, Brendon L Neuen, Vlado PerkovicJack JackNo ratings yet
- Nephrotic Syndrome Review 2024Document10 pagesNephrotic Syndrome Review 2024Jonathan MorenoNo ratings yet
- Drug Induced Tubular InjuryDocument8 pagesDrug Induced Tubular InjuryRania T. SabriNo ratings yet
- Acute Renal FailureDocument14 pagesAcute Renal FailuredrtpkNo ratings yet
- Calcium Dobesilate in Symptomatic Treatment of Hemorrhoidal Disease: An Interventional StudyDocument3 pagesCalcium Dobesilate in Symptomatic Treatment of Hemorrhoidal Disease: An Interventional StudyN R Reddy HemanthNo ratings yet
- Chronic Kidney Disease and Acute Kidney InjuryDocument46 pagesChronic Kidney Disease and Acute Kidney Injurydikiprestya391No ratings yet
- Cleveland Clinic Journal of Medicine 2003 Kashif 535 7Document9 pagesCleveland Clinic Journal of Medicine 2003 Kashif 535 7shiloinNo ratings yet
- Review of Refractory Lupus NephritisDocument12 pagesReview of Refractory Lupus NephritisDeddy WijayaNo ratings yet
- Oftal Case StudyDocument11 pagesOftal Case StudyMohamad RaisNo ratings yet
- Drug-Induced Nephrotoxicity: Gabriel Teixeira Montezuma Sales Renato Demarchi ForestoDocument9 pagesDrug-Induced Nephrotoxicity: Gabriel Teixeira Montezuma Sales Renato Demarchi ForestoCecep Darwis MuttaqinNo ratings yet
- Renal DiseasesDocument26 pagesRenal DiseasesismailcemNo ratings yet
- Diagnosis and Management of Acute Pancreatitis andDocument11 pagesDiagnosis and Management of Acute Pancreatitis andMarcelitaTaliaDuwiriNo ratings yet
- Chronic PancreatitisDocument8 pagesChronic PancreatitisSanjaya SenevirathneNo ratings yet
- Proteinuria in Diabetic Kidney Disease A MechanisticDocument15 pagesProteinuria in Diabetic Kidney Disease A Mechanisticmutiara nurzaniNo ratings yet
- Management of Patients With Nephrotic Syndrome: Sophie de Seigneux, Pierre-Yves MartinDocument7 pagesManagement of Patients With Nephrotic Syndrome: Sophie de Seigneux, Pierre-Yves MartinGarit Hapsari KiranaNo ratings yet
- CKD Lancet 2021Document17 pagesCKD Lancet 2021Fabiola AlonsoNo ratings yet
- Case Report of Acute and Chronic Interstitial NephritisDocument10 pagesCase Report of Acute and Chronic Interstitial NephritisDoncyNo ratings yet
- Artigotutoria PDFDocument12 pagesArtigotutoria PDFZARA BATISTANo ratings yet
- Chronic Renal Failure and Uremia: ObjectivesDocument7 pagesChronic Renal Failure and Uremia: ObjectivesNurulSyaidahNo ratings yet
- Headache: General PrinciplesDocument5 pagesHeadache: General PrinciplesAl Glen EgarleNo ratings yet
- 1.acute Kidney InjuryDocument3 pages1.acute Kidney InjuryIan CruzNo ratings yet
- Renal Disease 2023Document9 pagesRenal Disease 2023MaeNo ratings yet
- Biomarcadores en IRC Temprana en Gatos 2013Document6 pagesBiomarcadores en IRC Temprana en Gatos 2013Wilson Enrique Guerrero JojoaNo ratings yet
- Renal CaseDocument3 pagesRenal CaseAndy BiersackNo ratings yet
- Review On Treatment of Gout & HyperuricemiaDocument11 pagesReview On Treatment of Gout & HyperuricemiaMirza ProthikhaNo ratings yet
- ACG Clinical Guideline: Chronic PancreatitisDocument18 pagesACG Clinical Guideline: Chronic PancreatitisRene CordovaNo ratings yet
- Piis0085253815527324 PDFDocument5 pagesPiis0085253815527324 PDFdodong skyroseNo ratings yet
- Gagal Ginjal Akut - Bhs InggrisDocument27 pagesGagal Ginjal Akut - Bhs InggrisAgustinusNo ratings yet
- Nefropatia Diabetica Trayectorias NATUREDocument11 pagesNefropatia Diabetica Trayectorias NATURERAUL ALMYR MONTES GONZALEZNo ratings yet
- 2018 Tto Del SN CorticoresistenteDocument11 pages2018 Tto Del SN CorticoresistenteJeff Daniel Landauro PanayNo ratings yet
- RevDiabeticStud 12 087Document23 pagesRevDiabeticStud 12 087Win by the ForceNo ratings yet
- Hussein 2009Document4 pagesHussein 2009djsuraz0No ratings yet
- Acute Kidney Injury: Current Concepts and New Insights: Key WordsDocument5 pagesAcute Kidney Injury: Current Concepts and New Insights: Key WordsIHNo ratings yet
- The Perfect Neutropenic Diet Cookbook; The Complete Nutrition Guide To Reinstating Overall Health For General Wellness With Delectable And Nourishing RecipesFrom EverandThe Perfect Neutropenic Diet Cookbook; The Complete Nutrition Guide To Reinstating Overall Health For General Wellness With Delectable And Nourishing RecipesNo ratings yet
- Hypoxic Ischaemic Encephalopathy HIE AsphyxiaDocument6 pagesHypoxic Ischaemic Encephalopathy HIE AsphyxiaCaity YoungNo ratings yet
- A I - E M: Drenal Nsufficiency Mergency AnagementDocument12 pagesA I - E M: Drenal Nsufficiency Mergency AnagementCaity YoungNo ratings yet
- Rhumatologie-Pediatrique FRDocument4 pagesRhumatologie-Pediatrique FRCaity YoungNo ratings yet
- Afoem Sample Paper Stage B Written Exam Paper 7Document46 pagesAfoem Sample Paper Stage B Written Exam Paper 7Caity YoungNo ratings yet
- Afoem Sample Paper Stage B Written Exam Paper 7Document43 pagesAfoem Sample Paper Stage B Written Exam Paper 7Caity YoungNo ratings yet
- 2014 A Health Professionals Guide To Using The ChartsDocument14 pages2014 A Health Professionals Guide To Using The ChartsCaity YoungNo ratings yet
- CP2 Learning ObjectivesDocument992 pagesCP2 Learning ObjectivesCaity YoungNo ratings yet
- Fluid Calculator DKADocument3 pagesFluid Calculator DKACaity YoungNo ratings yet
- SSHADESS HandoutDocument1 pageSSHADESS HandoutCaity YoungNo ratings yet
- Reference Ranges For Urinalysis - Microbiology: Test Range Units DateDocument1 pageReference Ranges For Urinalysis - Microbiology: Test Range Units DateCaity YoungNo ratings yet
- 2 - McDonald - Examples - of - Unhelpful - ThoughtsDocument2 pages2 - McDonald - Examples - of - Unhelpful - ThoughtsCaity YoungNo ratings yet
- SpirometryDocument17 pagesSpirometryCaity YoungNo ratings yet
- Correspondence: Classifi Cation of CFTR Mutation ClassesDocument2 pagesCorrespondence: Classifi Cation of CFTR Mutation ClassesCaity YoungNo ratings yet
- Genetic Basis For Congenital Heart Disease: Revisited: CirculationDocument59 pagesGenetic Basis For Congenital Heart Disease: Revisited: CirculationCaity YoungNo ratings yet
- ToF ScriptDocument6 pagesToF ScriptCaity YoungNo ratings yet
- Part 2: Male Reproductive System: Normal Physiology and StructureDocument30 pagesPart 2: Male Reproductive System: Normal Physiology and StructureCaity YoungNo ratings yet
- 4-5 GlomerularDiseasesDocument21 pages4-5 GlomerularDiseasesCaity YoungNo ratings yet
- Sore Throat: Navigating The Differential DiagnosisDocument7 pagesSore Throat: Navigating The Differential DiagnosisCaity YoungNo ratings yet