
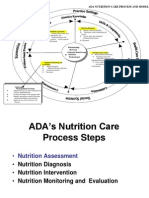
Nutrition Care Process Midterm Notes
Nutrition Care Process Midterm Notes
You might also like
- PES Statement Cheat SheetDocument17 pagesPES Statement Cheat SheetCarly100% (2)
- Hinmans Atlas of Pediatric Urology SurgeryDocument950 pagesHinmans Atlas of Pediatric Urology SurgeryDian Auliah Sari HafiedNo ratings yet
- Case 3 QuestionsDocument8 pagesCase 3 Questionsapi-532124328No ratings yet
- Test Bank For Medical Terminology and Anatomy For Coding 3rd Edition by ShilandDocument8 pagesTest Bank For Medical Terminology and Anatomy For Coding 3rd Edition by Shilanda5967275420% (2)
- Adime Note Sports NutritionDocument3 pagesAdime Note Sports Nutritionapi-242547654No ratings yet
- Case Study OutlineDocument3 pagesCase Study OutlineExcel MarieNo ratings yet
- Adime RenalDocument3 pagesAdime Renalapi-508953960No ratings yet
- MODULE IV. Notes 1Document10 pagesMODULE IV. Notes 1Thea Shaine B. SILARDE100% (1)
- Nutrition LecDocument14 pagesNutrition LecCheska jane Morales100% (1)
- An Introduction To Agricultural BiochemistryDocument490 pagesAn Introduction To Agricultural BiochemistryJecel Lazarra50% (2)
- MNT Case Study For IBSDocument7 pagesMNT Case Study For IBSRuihan LINo ratings yet
- ADA Nutrition Diagnosis and Intervention Standardized Language For The Nutrition Care Process PDFDocument292 pagesADA Nutrition Diagnosis and Intervention Standardized Language For The Nutrition Care Process PDFofalNo ratings yet
- Nutritional AssessmentDocument49 pagesNutritional AssessmentIrene Grace Balcueva100% (1)
- Nutrition Care Process FormDocument1 pageNutrition Care Process Formilham nugrahaNo ratings yet
- 5 Nutrition Care ProcessDocument10 pages5 Nutrition Care ProcessMilagros Constantino100% (1)
- PES StatementsDocument6 pagesPES Statementsdoniazad13112100% (1)
- Pes Statements SamplesDocument19 pagesPes Statements SamplesJennie ManobanNo ratings yet
- Nutrition & Diet Therapy: By: Odessa S. Bugarin, ManDocument46 pagesNutrition & Diet Therapy: By: Odessa S. Bugarin, ManWincy Salazar100% (1)
- Nutritional Support NotesDocument14 pagesNutritional Support NotesAudrie Allyson Gabales100% (1)
- Booklet NBCDocument93 pagesBooklet NBCJermeLou BaoNo ratings yet
- Porter Obesity Adime 2Document3 pagesPorter Obesity Adime 2api-538657643No ratings yet
- Nutrition Guidelines - InsideDocument81 pagesNutrition Guidelines - Insideannaafia69969No ratings yet
- NCPT For EALDocument61 pagesNCPT For EALAsri SubarjatiNo ratings yet
- Nutritional StatusDocument5 pagesNutritional StatusBern Nerquit100% (1)
- Screening Nutrition Care ProcessDocument70 pagesScreening Nutrition Care ProcessSiwonniekyubum DijaNo ratings yet
- NCP Step 2. Nutrition Diagnosis: SnapshotDocument2 pagesNCP Step 2. Nutrition Diagnosis: SnapshotFalguniNo ratings yet
- Nutrition Care Process Briefer CP OrientationDocument37 pagesNutrition Care Process Briefer CP OrientationDadanNo ratings yet
- Casestudy 1Document6 pagesCasestudy 1api-240055755No ratings yet
- Adime Note PracticeDocument2 pagesAdime Note Practiceapi-497774789100% (1)
- LIFE CYCLE NUTRITION - Pregnancy and Lactation 2Document63 pagesLIFE CYCLE NUTRITION - Pregnancy and Lactation 2Ruby Ann David-DancelNo ratings yet
- Nutrition Care Process (NCP)Document48 pagesNutrition Care Process (NCP)annyeong_123100% (1)
- Nutritional AssessmentDocument7 pagesNutritional AssessmentCm MacaliaNo ratings yet
- Dietary Assessment Methods in Nutrition EpidemiologyDocument14 pagesDietary Assessment Methods in Nutrition EpidemiologyArMadea De'aMra100% (1)
- Nutrition in Health and Illness: For 2 Yr Nursing StudentsDocument46 pagesNutrition in Health and Illness: For 2 Yr Nursing StudentsGizachew Asimare100% (2)
- Nutritional AssessmentDocument28 pagesNutritional AssessmentArella Flores100% (2)
- Basic Concepts of Food and NutritionDocument14 pagesBasic Concepts of Food and NutritionDilon MendoncaNo ratings yet
- Nutrition Care ProcessDocument17 pagesNutrition Care ProcessJamie VispoNo ratings yet
- 2012 - Nutritional Biochem and Clin Dietetics Mock Board PDFDocument15 pages2012 - Nutritional Biochem and Clin Dietetics Mock Board PDFNhadziy IsmaelNo ratings yet
- C The Food & Nutrition Program PlanningDocument8 pagesC The Food & Nutrition Program PlanningGabriel PhilippeNo ratings yet
- Nutri Lab Group ReportDocument14 pagesNutri Lab Group ReportJay Estrella100% (2)
- Nutrition Care Process NCP For RenalDocument17 pagesNutrition Care Process NCP For RenalJermeLou BaoNo ratings yet
- Nutritional EpidemiologyDocument3 pagesNutritional Epidemiologylample100% (1)
- Dietary TherapyDocument48 pagesDietary TherapyVanetNo ratings yet
- Nutrition Across The LifespanDocument31 pagesNutrition Across The LifespanGuila Aira Gracelle100% (1)
- Snapshot NCP Step 3 Nutrition Intervention-1Document1 pageSnapshot NCP Step 3 Nutrition Intervention-1api-250924915No ratings yet
- Chapter 9 - Sensory EvaluationDocument15 pagesChapter 9 - Sensory EvaluationLiyana ShahiminNo ratings yet
- AdimeDocument4 pagesAdimeapi-340838547No ratings yet
- Case Study ObesityDocument2 pagesCase Study ObesityPaolo Alshu PacresNo ratings yet
- Lesson 2 - Principles of Nutrition TherapyDocument15 pagesLesson 2 - Principles of Nutrition TherapyJoddie LoplopNo ratings yet
- Clinical Nutrition Internship BookletDocument95 pagesClinical Nutrition Internship BookletomoleganpatienceNo ratings yet
- Hospital Diets MNTDocument7 pagesHospital Diets MNTCarl Mark Vincent Babasoro100% (1)
- Dietary Calculations 1 PDFDocument3 pagesDietary Calculations 1 PDFGuyon, Alhea L.100% (1)
- NA NME TerminologyDocument3 pagesNA NME TerminologyVha AmalaNo ratings yet
- Nutr302l NCP NotesDocument14 pagesNutr302l NCP Notesapi-271284613No ratings yet
- Introduction To Nutrition and Diet Therapy PDFDocument16 pagesIntroduction To Nutrition and Diet Therapy PDFOfficially RandomNo ratings yet
- Assessment of Nutritional SituationDocument24 pagesAssessment of Nutritional SituationMawasumi Ayu Andini0% (1)
- Online Diet Planning System by Farah AbdullahDocument25 pagesOnline Diet Planning System by Farah AbdullahDeepu kumarNo ratings yet
- Try This! Look Around You.: Directions: Cut Out 10 Food Labels With Nutrition FactsDocument12 pagesTry This! Look Around You.: Directions: Cut Out 10 Food Labels With Nutrition FactsChristine Joy MolinaNo ratings yet
- Adime Malnutrition and OncolgyDocument6 pagesAdime Malnutrition and Oncolgyapi-300587226100% (1)
- BASIC NUTRITION CALCULATIONS BY Nutritionist Zeeshan AhmadDocument8 pagesBASIC NUTRITION CALCULATIONS BY Nutritionist Zeeshan AhmadSaba TanveerNo ratings yet
- Water and Food SanitationDocument7 pagesWater and Food SanitationKaye Nee100% (1)
- Applied Nutrition and Dietetics 2020-2021Document6 pagesApplied Nutrition and Dietetics 2020-2021Anindita Phani100% (1)
- Food Science and Technology in Australia: A review of research since 1900From EverandFood Science and Technology in Australia: A review of research since 1900No ratings yet
- The Effects of COVID 19 Pandemic Outbreak On Food Consumption Preferences and Their Causes-With-Cover-Page-V2Document6 pagesThe Effects of COVID 19 Pandemic Outbreak On Food Consumption Preferences and Their Causes-With-Cover-Page-V2Jecel LazarraNo ratings yet
- UntitledDocument26 pagesUntitledJecel LazarraNo ratings yet
- Biochemical and Clinical Skills Laboratory: Kay Ma. Pearl S. Reyes RND, MDDocument25 pagesBiochemical and Clinical Skills Laboratory: Kay Ma. Pearl S. Reyes RND, MDJecel LazarraNo ratings yet
- NSTP CWTS 2 Module 1 Community Immersion of NSTPDocument33 pagesNSTP CWTS 2 Module 1 Community Immersion of NSTPJecel LazarraNo ratings yet
- Fundamentals of Food Technology Midterm NotesDocument14 pagesFundamentals of Food Technology Midterm NotesJecel LazarraNo ratings yet
- Life Stages Midterm FormulasDocument3 pagesLife Stages Midterm FormulasJecel LazarraNo ratings yet
- Nutrition in The Life Stages 1 Midterm NotesDocument21 pagesNutrition in The Life Stages 1 Midterm NotesJecel LazarraNo ratings yet
- Module 2 in NSTP Part 2Document8 pagesModule 2 in NSTP Part 2Jecel LazarraNo ratings yet
- Module 3 in NSTP Part 1Document7 pagesModule 3 in NSTP Part 1Jecel LazarraNo ratings yet
- RPH Act. 4Document1 pageRPH Act. 4Jecel LazarraNo ratings yet
- Module 2 in NSTP Part 2Document8 pagesModule 2 in NSTP Part 2Jecel LazarraNo ratings yet
- Name: Lazarra, Jecel B. Course/Year: BSND1-1Document10 pagesName: Lazarra, Jecel B. Course/Year: BSND1-1Jecel LazarraNo ratings yet
- The Effectiveness of Coconut (Cocosnucifera) Shell, Coir and Lakatan Banana (Musa Acuminata) Peel As Water FilterDocument19 pagesThe Effectiveness of Coconut (Cocosnucifera) Shell, Coir and Lakatan Banana (Musa Acuminata) Peel As Water FilterJecel Lazarra100% (1)
- Lab Module Activity - Blood and Blood VesselsDocument19 pagesLab Module Activity - Blood and Blood VesselsJecel LazarraNo ratings yet
- Lab Module Activity Respiratory SystemDocument8 pagesLab Module Activity Respiratory SystemJecel LazarraNo ratings yet
- Domains of Truth Examples Justification: 1. Objective DomainDocument1 pageDomains of Truth Examples Justification: 1. Objective DomainJecel LazarraNo ratings yet
- 1240 V. Concepcion Street., Sampaloc, Manila 1008Document15 pages1240 V. Concepcion Street., Sampaloc, Manila 1008Jecel LazarraNo ratings yet
- Academia in The Time of COVID-19: Towards An Ethics of Care: Planning Theory & PracticeDocument10 pagesAcademia in The Time of COVID-19: Towards An Ethics of Care: Planning Theory & PracticeJecel LazarraNo ratings yet
- Experiment-Design and Discussion Gacila-Et - Al-1Document6 pagesExperiment-Design and Discussion Gacila-Et - Al-1Jecel LazarraNo ratings yet
- Vector Voyage Worksheet 1: North Europe AmericaDocument1 pageVector Voyage Worksheet 1: North Europe AmericaJecel LazarraNo ratings yet
- Danger Signs During Pregnancy 4 1Document33 pagesDanger Signs During Pregnancy 4 1Precious Maslang PadawilNo ratings yet
- Algoritma StatinDocument1 pageAlgoritma StatinAgnes Irene ZagotoNo ratings yet
- Test Bank For Lehnes Pharmacology For Nursing Care Burchum 9th EditionDocument20 pagesTest Bank For Lehnes Pharmacology For Nursing Care Burchum 9th EditionLily Rector100% (45)
- OBSTETRICS - NotesDocument16 pagesOBSTETRICS - NotesGabrielle Joyce TagalaNo ratings yet
- Deep Learning-Based ElectrocarDocument9 pagesDeep Learning-Based ElectrocarAiraa ShaneNo ratings yet
- Markandeya Raju Test Reports 30.11.2021 PDFDocument2 pagesMarkandeya Raju Test Reports 30.11.2021 PDFHOD (MVGR Civil)No ratings yet
- M4 Module 12G-26203Document27 pagesM4 Module 12G-26203Michelle FactoNo ratings yet
- Drug Name Actions Side Effects Adverse Effects Indications Contraindication S Nursing Responsibilities Generic NameDocument2 pagesDrug Name Actions Side Effects Adverse Effects Indications Contraindication S Nursing Responsibilities Generic NameMae Abigail Mallonga BunaganNo ratings yet
- Screenshot 2024-02-02 at 00.43.06Document87 pagesScreenshot 2024-02-02 at 00.43.06khawaja.meraj707No ratings yet
- Unit 4 Capstone PowerpointDocument8 pagesUnit 4 Capstone Powerpointapi-269707483No ratings yet
- طفيليات نظري المحاضرة 18 (الثالثة)Document6 pagesطفيليات نظري المحاضرة 18 (الثالثة)montadheralaydiyNo ratings yet
- Acute Respiratory Distress Syndrome - Background, Pathophysiology, EtiologyDocument5 pagesAcute Respiratory Distress Syndrome - Background, Pathophysiology, EtiologyARHNo ratings yet
- SJDV 2/2015Document44 pagesSJDV 2/2015Aleksandar BugarskiNo ratings yet
- Clinical Translational Med - 2023 - Baez - Global South Research Is Critical For Understanding Brain Health Ageing andDocument4 pagesClinical Translational Med - 2023 - Baez - Global South Research Is Critical For Understanding Brain Health Ageing andPaul R. MessinaNo ratings yet
- ZofranDocument1 pageZofranKatie McPeek0% (1)
- Charcot Neuropathy TBH PresentationDocument15 pagesCharcot Neuropathy TBH PresentationHuguette Marie NseleNo ratings yet
- PedsCases CF Note (SP Edit)Document1 pagePedsCases CF Note (SP Edit)Mehtab AlamNo ratings yet
- Registered NurseDocument5 pagesRegistered Nurseapi-121390694No ratings yet
- Anorexia Integrated TreatmentDocument6 pagesAnorexia Integrated Treatmentmadequal2658No ratings yet
- Pulmonary EmbolismDocument16 pagesPulmonary EmbolismEhab Mokhtar WehebaNo ratings yet
- FIRST AID AND WATER SAFETY 3 HandoutDocument12 pagesFIRST AID AND WATER SAFETY 3 HandoutJOYCE ANN PEREGRINONo ratings yet
- Medical Hypotheses: James A. MorrisDocument5 pagesMedical Hypotheses: James A. Morriscut putri amalyaNo ratings yet
- Osteoarthritis and Fibromyalgia: by Tamara MitchellDocument13 pagesOsteoarthritis and Fibromyalgia: by Tamara MitchellmailbabuNo ratings yet
- Chapter 4 - Medical Aspects of Food SafetyDocument17 pagesChapter 4 - Medical Aspects of Food SafetyasushkNo ratings yet
- Thyroid Function Tests: What Is The Thyroid Gland?Document2 pagesThyroid Function Tests: What Is The Thyroid Gland?rastamaneazy269No ratings yet
- Drug StudyDocument43 pagesDrug StudyMamot MotNo ratings yet
- Mood Disorders-Causes and TreatmentsDocument9 pagesMood Disorders-Causes and TreatmentsMica MoradaNo ratings yet
- Jib Achha Applied Preventive Vet MedicineDocument2 pagesJib Achha Applied Preventive Vet MedicineAweke EngdaworkNo ratings yet











































































































Download as pdf or txt
You might also like
- PES Statement Cheat SheetDocument17 pagesPES Statement Cheat SheetCarly100% (2)
- Hinmans Atlas of Pediatric Urology SurgeryDocument950 pagesHinmans Atlas of Pediatric Urology SurgeryDian Auliah Sari HafiedNo ratings yet
- Case 3 QuestionsDocument8 pagesCase 3 Questionsapi-532124328No ratings yet
- Test Bank For Medical Terminology and Anatomy For Coding 3rd Edition by ShilandDocument8 pagesTest Bank For Medical Terminology and Anatomy For Coding 3rd Edition by Shilanda5967275420% (2)
- Adime Note Sports NutritionDocument3 pagesAdime Note Sports Nutritionapi-242547654No ratings yet
- Case Study OutlineDocument3 pagesCase Study OutlineExcel MarieNo ratings yet
- Adime RenalDocument3 pagesAdime Renalapi-508953960No ratings yet
- MODULE IV. Notes 1Document10 pagesMODULE IV. Notes 1Thea Shaine B. SILARDE100% (1)
- Nutrition LecDocument14 pagesNutrition LecCheska jane Morales100% (1)
- An Introduction To Agricultural BiochemistryDocument490 pagesAn Introduction To Agricultural BiochemistryJecel Lazarra50% (2)
- MNT Case Study For IBSDocument7 pagesMNT Case Study For IBSRuihan LINo ratings yet
- ADA Nutrition Diagnosis and Intervention Standardized Language For The Nutrition Care Process PDFDocument292 pagesADA Nutrition Diagnosis and Intervention Standardized Language For The Nutrition Care Process PDFofalNo ratings yet
- Nutritional AssessmentDocument49 pagesNutritional AssessmentIrene Grace Balcueva100% (1)
- Nutrition Care Process FormDocument1 pageNutrition Care Process Formilham nugrahaNo ratings yet
- 5 Nutrition Care ProcessDocument10 pages5 Nutrition Care ProcessMilagros Constantino100% (1)
- PES StatementsDocument6 pagesPES Statementsdoniazad13112100% (1)
- Pes Statements SamplesDocument19 pagesPes Statements SamplesJennie ManobanNo ratings yet
- Nutrition & Diet Therapy: By: Odessa S. Bugarin, ManDocument46 pagesNutrition & Diet Therapy: By: Odessa S. Bugarin, ManWincy Salazar100% (1)
- Nutritional Support NotesDocument14 pagesNutritional Support NotesAudrie Allyson Gabales100% (1)
- Booklet NBCDocument93 pagesBooklet NBCJermeLou BaoNo ratings yet
- Porter Obesity Adime 2Document3 pagesPorter Obesity Adime 2api-538657643No ratings yet
- Nutrition Guidelines - InsideDocument81 pagesNutrition Guidelines - Insideannaafia69969No ratings yet
- NCPT For EALDocument61 pagesNCPT For EALAsri SubarjatiNo ratings yet
- Nutritional StatusDocument5 pagesNutritional StatusBern Nerquit100% (1)
- Screening Nutrition Care ProcessDocument70 pagesScreening Nutrition Care ProcessSiwonniekyubum DijaNo ratings yet
- NCP Step 2. Nutrition Diagnosis: SnapshotDocument2 pagesNCP Step 2. Nutrition Diagnosis: SnapshotFalguniNo ratings yet
- Nutrition Care Process Briefer CP OrientationDocument37 pagesNutrition Care Process Briefer CP OrientationDadanNo ratings yet
- Casestudy 1Document6 pagesCasestudy 1api-240055755No ratings yet
- Adime Note PracticeDocument2 pagesAdime Note Practiceapi-497774789100% (1)
- LIFE CYCLE NUTRITION - Pregnancy and Lactation 2Document63 pagesLIFE CYCLE NUTRITION - Pregnancy and Lactation 2Ruby Ann David-DancelNo ratings yet
- Nutrition Care Process (NCP)Document48 pagesNutrition Care Process (NCP)annyeong_123100% (1)
- Nutritional AssessmentDocument7 pagesNutritional AssessmentCm MacaliaNo ratings yet
- Dietary Assessment Methods in Nutrition EpidemiologyDocument14 pagesDietary Assessment Methods in Nutrition EpidemiologyArMadea De'aMra100% (1)
- Nutrition in Health and Illness: For 2 Yr Nursing StudentsDocument46 pagesNutrition in Health and Illness: For 2 Yr Nursing StudentsGizachew Asimare100% (2)
- Nutritional AssessmentDocument28 pagesNutritional AssessmentArella Flores100% (2)
- Basic Concepts of Food and NutritionDocument14 pagesBasic Concepts of Food and NutritionDilon MendoncaNo ratings yet
- Nutrition Care ProcessDocument17 pagesNutrition Care ProcessJamie VispoNo ratings yet
- 2012 - Nutritional Biochem and Clin Dietetics Mock Board PDFDocument15 pages2012 - Nutritional Biochem and Clin Dietetics Mock Board PDFNhadziy IsmaelNo ratings yet
- C The Food & Nutrition Program PlanningDocument8 pagesC The Food & Nutrition Program PlanningGabriel PhilippeNo ratings yet
- Nutri Lab Group ReportDocument14 pagesNutri Lab Group ReportJay Estrella100% (2)
- Nutrition Care Process NCP For RenalDocument17 pagesNutrition Care Process NCP For RenalJermeLou BaoNo ratings yet
- Nutritional EpidemiologyDocument3 pagesNutritional Epidemiologylample100% (1)
- Dietary TherapyDocument48 pagesDietary TherapyVanetNo ratings yet
- Nutrition Across The LifespanDocument31 pagesNutrition Across The LifespanGuila Aira Gracelle100% (1)
- Snapshot NCP Step 3 Nutrition Intervention-1Document1 pageSnapshot NCP Step 3 Nutrition Intervention-1api-250924915No ratings yet
- Chapter 9 - Sensory EvaluationDocument15 pagesChapter 9 - Sensory EvaluationLiyana ShahiminNo ratings yet
- AdimeDocument4 pagesAdimeapi-340838547No ratings yet
- Case Study ObesityDocument2 pagesCase Study ObesityPaolo Alshu PacresNo ratings yet
- Lesson 2 - Principles of Nutrition TherapyDocument15 pagesLesson 2 - Principles of Nutrition TherapyJoddie LoplopNo ratings yet
- Clinical Nutrition Internship BookletDocument95 pagesClinical Nutrition Internship BookletomoleganpatienceNo ratings yet
- Hospital Diets MNTDocument7 pagesHospital Diets MNTCarl Mark Vincent Babasoro100% (1)
- Dietary Calculations 1 PDFDocument3 pagesDietary Calculations 1 PDFGuyon, Alhea L.100% (1)
- NA NME TerminologyDocument3 pagesNA NME TerminologyVha AmalaNo ratings yet
- Nutr302l NCP NotesDocument14 pagesNutr302l NCP Notesapi-271284613No ratings yet
- Introduction To Nutrition and Diet Therapy PDFDocument16 pagesIntroduction To Nutrition and Diet Therapy PDFOfficially RandomNo ratings yet
- Assessment of Nutritional SituationDocument24 pagesAssessment of Nutritional SituationMawasumi Ayu Andini0% (1)
- Online Diet Planning System by Farah AbdullahDocument25 pagesOnline Diet Planning System by Farah AbdullahDeepu kumarNo ratings yet
- Try This! Look Around You.: Directions: Cut Out 10 Food Labels With Nutrition FactsDocument12 pagesTry This! Look Around You.: Directions: Cut Out 10 Food Labels With Nutrition FactsChristine Joy MolinaNo ratings yet
- Adime Malnutrition and OncolgyDocument6 pagesAdime Malnutrition and Oncolgyapi-300587226100% (1)
- BASIC NUTRITION CALCULATIONS BY Nutritionist Zeeshan AhmadDocument8 pagesBASIC NUTRITION CALCULATIONS BY Nutritionist Zeeshan AhmadSaba TanveerNo ratings yet
- Water and Food SanitationDocument7 pagesWater and Food SanitationKaye Nee100% (1)
- Applied Nutrition and Dietetics 2020-2021Document6 pagesApplied Nutrition and Dietetics 2020-2021Anindita Phani100% (1)
- Food Science and Technology in Australia: A review of research since 1900From EverandFood Science and Technology in Australia: A review of research since 1900No ratings yet
- The Effects of COVID 19 Pandemic Outbreak On Food Consumption Preferences and Their Causes-With-Cover-Page-V2Document6 pagesThe Effects of COVID 19 Pandemic Outbreak On Food Consumption Preferences and Their Causes-With-Cover-Page-V2Jecel LazarraNo ratings yet
- UntitledDocument26 pagesUntitledJecel LazarraNo ratings yet
- Biochemical and Clinical Skills Laboratory: Kay Ma. Pearl S. Reyes RND, MDDocument25 pagesBiochemical and Clinical Skills Laboratory: Kay Ma. Pearl S. Reyes RND, MDJecel LazarraNo ratings yet
- NSTP CWTS 2 Module 1 Community Immersion of NSTPDocument33 pagesNSTP CWTS 2 Module 1 Community Immersion of NSTPJecel LazarraNo ratings yet
- Fundamentals of Food Technology Midterm NotesDocument14 pagesFundamentals of Food Technology Midterm NotesJecel LazarraNo ratings yet
- Life Stages Midterm FormulasDocument3 pagesLife Stages Midterm FormulasJecel LazarraNo ratings yet
- Nutrition in The Life Stages 1 Midterm NotesDocument21 pagesNutrition in The Life Stages 1 Midterm NotesJecel LazarraNo ratings yet
- Module 2 in NSTP Part 2Document8 pagesModule 2 in NSTP Part 2Jecel LazarraNo ratings yet
- Module 3 in NSTP Part 1Document7 pagesModule 3 in NSTP Part 1Jecel LazarraNo ratings yet
- RPH Act. 4Document1 pageRPH Act. 4Jecel LazarraNo ratings yet
- Module 2 in NSTP Part 2Document8 pagesModule 2 in NSTP Part 2Jecel LazarraNo ratings yet
- Name: Lazarra, Jecel B. Course/Year: BSND1-1Document10 pagesName: Lazarra, Jecel B. Course/Year: BSND1-1Jecel LazarraNo ratings yet
- The Effectiveness of Coconut (Cocosnucifera) Shell, Coir and Lakatan Banana (Musa Acuminata) Peel As Water FilterDocument19 pagesThe Effectiveness of Coconut (Cocosnucifera) Shell, Coir and Lakatan Banana (Musa Acuminata) Peel As Water FilterJecel Lazarra100% (1)
- Lab Module Activity - Blood and Blood VesselsDocument19 pagesLab Module Activity - Blood and Blood VesselsJecel LazarraNo ratings yet
- Lab Module Activity Respiratory SystemDocument8 pagesLab Module Activity Respiratory SystemJecel LazarraNo ratings yet
- Domains of Truth Examples Justification: 1. Objective DomainDocument1 pageDomains of Truth Examples Justification: 1. Objective DomainJecel LazarraNo ratings yet
- 1240 V. Concepcion Street., Sampaloc, Manila 1008Document15 pages1240 V. Concepcion Street., Sampaloc, Manila 1008Jecel LazarraNo ratings yet
- Academia in The Time of COVID-19: Towards An Ethics of Care: Planning Theory & PracticeDocument10 pagesAcademia in The Time of COVID-19: Towards An Ethics of Care: Planning Theory & PracticeJecel LazarraNo ratings yet
- Experiment-Design and Discussion Gacila-Et - Al-1Document6 pagesExperiment-Design and Discussion Gacila-Et - Al-1Jecel LazarraNo ratings yet
- Vector Voyage Worksheet 1: North Europe AmericaDocument1 pageVector Voyage Worksheet 1: North Europe AmericaJecel LazarraNo ratings yet
- Danger Signs During Pregnancy 4 1Document33 pagesDanger Signs During Pregnancy 4 1Precious Maslang PadawilNo ratings yet
- Algoritma StatinDocument1 pageAlgoritma StatinAgnes Irene ZagotoNo ratings yet
- Test Bank For Lehnes Pharmacology For Nursing Care Burchum 9th EditionDocument20 pagesTest Bank For Lehnes Pharmacology For Nursing Care Burchum 9th EditionLily Rector100% (45)
- OBSTETRICS - NotesDocument16 pagesOBSTETRICS - NotesGabrielle Joyce TagalaNo ratings yet
- Deep Learning-Based ElectrocarDocument9 pagesDeep Learning-Based ElectrocarAiraa ShaneNo ratings yet
- Markandeya Raju Test Reports 30.11.2021 PDFDocument2 pagesMarkandeya Raju Test Reports 30.11.2021 PDFHOD (MVGR Civil)No ratings yet
- M4 Module 12G-26203Document27 pagesM4 Module 12G-26203Michelle FactoNo ratings yet
- Drug Name Actions Side Effects Adverse Effects Indications Contraindication S Nursing Responsibilities Generic NameDocument2 pagesDrug Name Actions Side Effects Adverse Effects Indications Contraindication S Nursing Responsibilities Generic NameMae Abigail Mallonga BunaganNo ratings yet
- Screenshot 2024-02-02 at 00.43.06Document87 pagesScreenshot 2024-02-02 at 00.43.06khawaja.meraj707No ratings yet
- Unit 4 Capstone PowerpointDocument8 pagesUnit 4 Capstone Powerpointapi-269707483No ratings yet
- طفيليات نظري المحاضرة 18 (الثالثة)Document6 pagesطفيليات نظري المحاضرة 18 (الثالثة)montadheralaydiyNo ratings yet
- Acute Respiratory Distress Syndrome - Background, Pathophysiology, EtiologyDocument5 pagesAcute Respiratory Distress Syndrome - Background, Pathophysiology, EtiologyARHNo ratings yet
- SJDV 2/2015Document44 pagesSJDV 2/2015Aleksandar BugarskiNo ratings yet
- Clinical Translational Med - 2023 - Baez - Global South Research Is Critical For Understanding Brain Health Ageing andDocument4 pagesClinical Translational Med - 2023 - Baez - Global South Research Is Critical For Understanding Brain Health Ageing andPaul R. MessinaNo ratings yet
- ZofranDocument1 pageZofranKatie McPeek0% (1)
- Charcot Neuropathy TBH PresentationDocument15 pagesCharcot Neuropathy TBH PresentationHuguette Marie NseleNo ratings yet
- PedsCases CF Note (SP Edit)Document1 pagePedsCases CF Note (SP Edit)Mehtab AlamNo ratings yet
- Registered NurseDocument5 pagesRegistered Nurseapi-121390694No ratings yet
- Anorexia Integrated TreatmentDocument6 pagesAnorexia Integrated Treatmentmadequal2658No ratings yet
- Pulmonary EmbolismDocument16 pagesPulmonary EmbolismEhab Mokhtar WehebaNo ratings yet
- FIRST AID AND WATER SAFETY 3 HandoutDocument12 pagesFIRST AID AND WATER SAFETY 3 HandoutJOYCE ANN PEREGRINONo ratings yet
- Medical Hypotheses: James A. MorrisDocument5 pagesMedical Hypotheses: James A. Morriscut putri amalyaNo ratings yet
- Osteoarthritis and Fibromyalgia: by Tamara MitchellDocument13 pagesOsteoarthritis and Fibromyalgia: by Tamara MitchellmailbabuNo ratings yet
- Chapter 4 - Medical Aspects of Food SafetyDocument17 pagesChapter 4 - Medical Aspects of Food SafetyasushkNo ratings yet
- Thyroid Function Tests: What Is The Thyroid Gland?Document2 pagesThyroid Function Tests: What Is The Thyroid Gland?rastamaneazy269No ratings yet
- Drug StudyDocument43 pagesDrug StudyMamot MotNo ratings yet
- Mood Disorders-Causes and TreatmentsDocument9 pagesMood Disorders-Causes and TreatmentsMica MoradaNo ratings yet
- Jib Achha Applied Preventive Vet MedicineDocument2 pagesJib Achha Applied Preventive Vet MedicineAweke EngdaworkNo ratings yet