Download as pdf or txt
You might also like
- Carbon180 - A Review of Global and U.S. Total Available Markets For CarbontechDocument11 pagesCarbon180 - A Review of Global and U.S. Total Available Markets For CarbontechTito JankowskiNo ratings yet
- 26 Manuals 3338, Anti-Aircraft Ammunition PDFDocument129 pages26 Manuals 3338, Anti-Aircraft Ammunition PDFKosta_g100% (1)
- Analgesics Pain MedsDocument113 pagesAnalgesics Pain Medsalhader libraryNo ratings yet
- Other CNS Drugs MonasDocument172 pagesOther CNS Drugs MonasMichael MohammedNo ratings yet
- Opioid AnalgesicsDocument27 pagesOpioid AnalgesicsDivya VarsiniNo ratings yet
- Pharmacology of Opioids1Document36 pagesPharmacology of Opioids1shikhaNo ratings yet
- Yasmin HurdDocument41 pagesYasmin HurdNational Press FoundationNo ratings yet
- Lecture 16-17 - Opioids AnalgesicsDocument20 pagesLecture 16-17 - Opioids AnalgesicsJedoNo ratings yet
- Opioids - An IntroductionDocument48 pagesOpioids - An IntroductionPranathi PrasadNo ratings yet
- 404T Opioid Analgesics and AntagonistDocument14 pages404T Opioid Analgesics and AntagonistRaja RajaNo ratings yet
- 2024-02-29 - 1 - Lecture 16-Opioid Analgesics - Lecture NotesDocument14 pages2024-02-29 - 1 - Lecture 16-Opioid Analgesics - Lecture Notesbaf49411No ratings yet
- Ketidak Patuhan Minum ObatDocument113 pagesKetidak Patuhan Minum ObatNabilla Andasari PutriNo ratings yet
- Fo Analgetik Opioid - Blok6Document65 pagesFo Analgetik Opioid - Blok6Rhena Fitria KhairunnisaNo ratings yet
- Opioid Pharmacology Definitions: N-CH 3 N-CH 3Document13 pagesOpioid Pharmacology Definitions: N-CH 3 N-CH 3Louis Fortunato100% (1)
- 08 OpioidsDocument44 pages08 OpioidsRamya RNo ratings yet
- Referat Analgesik OpioidDocument25 pagesReferat Analgesik OpioidDeny Prima ONo ratings yet
- Opioid PharmacologyDocument47 pagesOpioid PharmacologyEva K. Al KaryNo ratings yet
- Anes DLR Feb 22 2023Document7 pagesAnes DLR Feb 22 2023Benjune RoseladaNo ratings yet
- Opioid Analgesics & Antagonists: Dr. Hayder B Sahib Ph.D. PharmacologyDocument47 pagesOpioid Analgesics & Antagonists: Dr. Hayder B Sahib Ph.D. Pharmacologyarham pirachaNo ratings yet
- Opioid Analgesics: Dr. D. K. Brahma Department of Pharmacology, NEIGRIHMS Shillong, Meghalaya, ImdiaDocument48 pagesOpioid Analgesics: Dr. D. K. Brahma Department of Pharmacology, NEIGRIHMS Shillong, Meghalaya, ImdiaAmiraBenhammou100% (1)
- Opoids TsegiDocument56 pagesOpoids TsegiYosef AssefaNo ratings yet
- OpiodsDocument117 pagesOpiodsTaniya GuptaNo ratings yet
- Opioid Analgesics - A 2018 Update: SA Pharmaceutical Journal January 2018Document8 pagesOpioid Analgesics - A 2018 Update: SA Pharmaceutical Journal January 2018Prudhvi Sai NidadavoluNo ratings yet
- Unit 2-CNS and ANS (Part 3) Modified 2021Document30 pagesUnit 2-CNS and ANS (Part 3) Modified 2021Donia ShormanNo ratings yet
- Opiod Analgesics &antagonistsDocument58 pagesOpiod Analgesics &antagonistsVictoria ChepkorirNo ratings yet
- NarcoticsDocument6 pagesNarcoticsanaeshkl100% (1)
- Presented byDocument71 pagesPresented byRun HajNo ratings yet
- PainDocument23 pagesPainnazbeen.ahmadiNo ratings yet
- Pharm 4 ADocument3 pagesPharm 4 Aravi2likeNo ratings yet
- L6-Analgesics-Pain Relief (BB) - 1Document39 pagesL6-Analgesics-Pain Relief (BB) - 1120420314No ratings yet
- Opoid AnalgesicsDocument29 pagesOpoid AnalgesicsShivsharan100% (1)
- AnalgesiaDocument40 pagesAnalgesiacardiacanesthesiaNo ratings yet
- Antipsychotic Drugs: Referance Book .Essential of Pharmacology by Shah NawazDocument47 pagesAntipsychotic Drugs: Referance Book .Essential of Pharmacology by Shah NawazLaiba ShahNo ratings yet
- Analgesics Agents ZJDocument37 pagesAnalgesics Agents ZJDanial HassanNo ratings yet
- L P Local Anaesthetics Final-1Document24 pagesL P Local Anaesthetics Final-1Zakria Al-HadadNo ratings yet
- Introduction Classification Benzodiazepines BarbituratesDocument15 pagesIntroduction Classification Benzodiazepines BarbituratesVijetha RaiNo ratings yet
- Chapter 4: PsychopharmacologyDocument37 pagesChapter 4: PsychopharmacologyGummyCola100% (2)
- Pharmacology - 1 CNS Sedatives & Hypnotics: Maram A.T. M. KhaledDocument14 pagesPharmacology - 1 CNS Sedatives & Hypnotics: Maram A.T. M. Khaledمحمد الاسوانيNo ratings yet
- OpioidDocument8 pagesOpioidNadia Dwi AriniNo ratings yet
- Opioides Update AustPrescr2014 (1582)Document5 pagesOpioides Update AustPrescr2014 (1582)Paulina ChangoNo ratings yet
- Narcotics Abuse Spring 2021Document51 pagesNarcotics Abuse Spring 2021Fatma HishamNo ratings yet
- AnalgesicDocument56 pagesAnalgesicMuhammad hilmiNo ratings yet
- PHARM Ven IntroToAnesthesiaDocument22 pagesPHARM Ven IntroToAnesthesiaDhaif dhaifNo ratings yet
- Opioid PPTTDocument43 pagesOpioid PPTTking_goldNo ratings yet
- OpioidsDocument29 pagesOpioidsHassan Jahangir100% (1)
- Opioid Analgesics: Dr. Nisha.A.RDocument93 pagesOpioid Analgesics: Dr. Nisha.A.RHassim M H SNo ratings yet
- Opioid Analgesics & AntagonistsDocument13 pagesOpioid Analgesics & AntagonistsafiniherlyanaNo ratings yet
- Opioid AnalgesicDocument43 pagesOpioid AnalgesicAnanta MiaNo ratings yet
- Book ReadingDocument37 pagesBook Reading東廣謀No ratings yet
- Opioids by MDocument24 pagesOpioids by Mwww.munnamichel20No ratings yet
- AnalgesicsDocument36 pagesAnalgesicsTakale BuloNo ratings yet
- CASE1Document13 pagesCASE1tanishapatel1005No ratings yet
- Medical University of Sofia, Faculty of Medicine Department of Pharmacology and ToxicologyDocument51 pagesMedical University of Sofia, Faculty of Medicine Department of Pharmacology and ToxicologyAMIN THAWABTEHNo ratings yet
- AntidepresentDocument34 pagesAntidepresentmariaNo ratings yet
- Introduction To CNS PharmacologyDocument22 pagesIntroduction To CNS PharmacologyTamiru KetemaNo ratings yet
- Opioid Analgesics - Ratna AgusDocument37 pagesOpioid Analgesics - Ratna AgusratnaekawatiNo ratings yet
- Opioid Dependence: DR Ayedh AlkhademDocument39 pagesOpioid Dependence: DR Ayedh AlkhademAyedh TalhaNo ratings yet
- Opiates 2008Document102 pagesOpiates 2008drdavemcdowellNo ratings yet
- Pharmacology - 1 Analgesics: Maram A.T. M. KhaledDocument15 pagesPharmacology - 1 Analgesics: Maram A.T. M. Khaledمحمد الاسوانيNo ratings yet
- Psychopharmacology: A Clinician's Guide for the Effective use of Psychotropic MedicationsFrom EverandPsychopharmacology: A Clinician's Guide for the Effective use of Psychotropic MedicationsNo ratings yet
- 6.4 Procedure For InsulationDocument11 pages6.4 Procedure For Insulationrendra syamNo ratings yet
- Overview of Citric Acid Production From Aspergillus NigerDocument14 pagesOverview of Citric Acid Production From Aspergillus NigerPetru AstefanoaieNo ratings yet
- Magne ProvisionalsDocument10 pagesMagne Provisionalsdrdanielsan100% (1)
- Living Magazine doTERRA Spring 2018 Living MagazineDocument29 pagesLiving Magazine doTERRA Spring 2018 Living Magazineczinege_zoltan3079No ratings yet
- WantedDocument4 pagesWantedMansoor TheenNo ratings yet
- Miraa AbuseDocument2 pagesMiraa AbusewilliamwachiraNo ratings yet
- Programming For Competitive CrossfitDocument53 pagesProgramming For Competitive CrossfitcamilcaNo ratings yet
- Electrical Troubleshooting VespaDocument19 pagesElectrical Troubleshooting VespaMuch Abdulah NurhidayatNo ratings yet
- Optics-Hecht - 03-Chap4-The Propagation of Light - OKDocument45 pagesOptics-Hecht - 03-Chap4-The Propagation of Light - OKfara latifa100% (2)
- W1 Water On EarthDocument28 pagesW1 Water On EarthNetkoNo ratings yet
- Summation of The Sciencemadness Phosphorous ThreadDocument29 pagesSummation of The Sciencemadness Phosphorous ThreadImranNo ratings yet
- Drew Z CVDocument4 pagesDrew Z CVapi-483994460No ratings yet
- 2014 Ftir LabDocument10 pages2014 Ftir LabAnurak OnnnoomNo ratings yet
- DO 5510 LutronDocument2 pagesDO 5510 LutronAditya Arki WardanaNo ratings yet
- Anatomical Effects of Woolly Apple Aphid (Eriosoma Lanigerum Haus) in The Apple Tree BranchDocument9 pagesAnatomical Effects of Woolly Apple Aphid (Eriosoma Lanigerum Haus) in The Apple Tree BranchSaurabh SharmaNo ratings yet
- Roygbiv Love, Simon: Troye SivanDocument6 pagesRoygbiv Love, Simon: Troye SivanJuliana AbanadorNo ratings yet
- Reviewer PurComm Communications and BarriersDocument5 pagesReviewer PurComm Communications and BarriersMhavs CasimiroNo ratings yet
- Topic 8 Cell Respiration and PhotosynthesisDocument12 pagesTopic 8 Cell Respiration and PhotosynthesisCedric Williams100% (1)
- Answers Quiz2Document3 pagesAnswers Quiz2Salim MattarNo ratings yet
- Aashto M145-91Document5 pagesAashto M145-91KkNo ratings yet
- Loi - FormatDocument5 pagesLoi - Formatnandini2309100% (2)
- Fluorescence SpectrosDocument52 pagesFluorescence Spectroshafsa BNo ratings yet
- Data Sheet 6ES7231-4HF32-0XB0: General InformationDocument4 pagesData Sheet 6ES7231-4HF32-0XB0: General InformationafiNo ratings yet
- Lecture 7 & 8 Non-Mendelian GeneticsDocument49 pagesLecture 7 & 8 Non-Mendelian GeneticsSaakshi PalNo ratings yet
- Hidayah, N., A. N. Al-Baarri, Dan C. BudiartiDocument6 pagesHidayah, N., A. N. Al-Baarri, Dan C. Budiartiaulia rahmahNo ratings yet
- Pile Capacity Calculation in Accordance With IS-2911: As Per Geotech Report As Per Geotech Report As Per Geotech ReportDocument4 pagesPile Capacity Calculation in Accordance With IS-2911: As Per Geotech Report As Per Geotech Report As Per Geotech ReportShuja ShowkatNo ratings yet
- 5.cascara SagradaDocument10 pages5.cascara SagradajayNo ratings yet
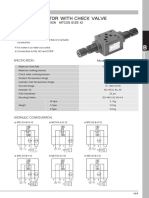
- MTC 03 W Throttle Check ValveDocument4 pagesMTC 03 W Throttle Check Valve박준용No ratings yet