
Factors Contributing To Emergence of Hypertension in Diabetic Patients Attending Diabetics Outpatient Clinic in Nyamira County
Factors Contributing To Emergence of Hypertension in Diabetic Patients Attending Diabetics Outpatient Clinic in Nyamira County
You might also like
- Health Education Interventions For Older Adults With Hypertension: A Systematic Review and Meta-AnalysisDocument9 pagesHealth Education Interventions For Older Adults With Hypertension: A Systematic Review and Meta-AnalysisJosé Carlos Sánchez-RamirezNo ratings yet
- IC 13 Guidelines On Standards For High Dependency UnitsDocument4 pagesIC 13 Guidelines On Standards For High Dependency UnitsAnonymous 0WHX7nNo ratings yet
- Angelina Alphonce JohoDocument80 pagesAngelina Alphonce JohoMerlina WijayawatiNo ratings yet
- Final Research ProposalDocument20 pagesFinal Research ProposalNatnael G.No ratings yet
- Factors Affecting Management of Sickle Cell Disease Among Children 0-12 Years Attending Nakaseke Sickle Cell ClinicDocument66 pagesFactors Affecting Management of Sickle Cell Disease Among Children 0-12 Years Attending Nakaseke Sickle Cell Clinicbaluku yosiah100% (1)
- Literature Review On Diabetes PDFDocument4 pagesLiterature Review On Diabetes PDFklbndecnd100% (1)
- Research ProposalDocument24 pagesResearch ProposalLorraine ZarateNo ratings yet
- NCD National PolicyDocument14 pagesNCD National PolicyHerlene Lyneth ZalamedaNo ratings yet
- Assessment of Awareness of Diabetic Retinopathy Among Type 2 Diabetes Mellitus Cross Sectional Study From Central IndiaDocument7 pagesAssessment of Awareness of Diabetic Retinopathy Among Type 2 Diabetes Mellitus Cross Sectional Study From Central IndiaAthenaeum Scientific PublishersNo ratings yet
- Final Pint ResearchDocument90 pagesFinal Pint ResearchNhelia Santos BañagaNo ratings yet
- IPD Patient History ChecklistDocument2 pagesIPD Patient History ChecklistdrjriNo ratings yet
- Basic Public Health (1) - MergedDocument89 pagesBasic Public Health (1) - Mergedrimsha tariqNo ratings yet
- Management of Vacuum Assisted Closure TherapyDocument14 pagesManagement of Vacuum Assisted Closure TherapyVoiculescu MihaelaNo ratings yet
- Barriers To Access Quality Healthcare Services Among Physically Challenged Persons in Gem Sub County, Siaya County'Document9 pagesBarriers To Access Quality Healthcare Services Among Physically Challenged Persons in Gem Sub County, Siaya County'Premier PublishersNo ratings yet
- Marylin's ProjectDocument84 pagesMarylin's ProjectDavid UdohNo ratings yet
- Edited Research ProposalDocument20 pagesEdited Research ProposalNestoryNo ratings yet
- Under Nutrition and Its Associated Factors Among Adolescent Girls in Rural Community of Aseko District, Eastern Arsi Zone, Oromia Region, Eastern Ethiopia, 2017Document10 pagesUnder Nutrition and Its Associated Factors Among Adolescent Girls in Rural Community of Aseko District, Eastern Arsi Zone, Oromia Region, Eastern Ethiopia, 2017Anonymous SMEU6r2No ratings yet
- JBDS Oncology Guideline Final Revised September 2021Document57 pagesJBDS Oncology Guideline Final Revised September 2021Majid KhanNo ratings yet
- Nancy,,, GITARI PROJECTDocument46 pagesNancy,,, GITARI PROJECTjohn mwambuNo ratings yet
- RMNCAH Quality Improvement QI FrameworkDocument82 pagesRMNCAH Quality Improvement QI FrameworkShahidul Islam ChowdhuryNo ratings yet
- KAP Analysis of Covid-19Document9 pagesKAP Analysis of Covid-19Bhaskar ReddyNo ratings yet
- Antihypertension Non AdherenceDocument16 pagesAntihypertension Non AdherencebezieNo ratings yet
- WDF14-852 Draft Guidelines TB-DM 07-01-2015Document20 pagesWDF14-852 Draft Guidelines TB-DM 07-01-2015adindadian12No ratings yet
- Synopsis 8TH AAAAaaDocument19 pagesSynopsis 8TH AAAAaaعثمان علیNo ratings yet
- Research ProposalDocument21 pagesResearch ProposalBeatrice KarimiNo ratings yet
- IdrvDocument39 pagesIdrvMyk MacalintalNo ratings yet
- Diet and Exercise in Management of Obesity and OveDocument6 pagesDiet and Exercise in Management of Obesity and OveXavi Martinez SantamariaNo ratings yet
- Trends in Nursing PracticeDocument12 pagesTrends in Nursing PracticeJerome Cid100% (1)
- Adeliana Joseph KJDocument29 pagesAdeliana Joseph KJNyagawa GodkNo ratings yet
- Health IndicatorDocument30 pagesHealth IndicatorPawan KumarNo ratings yet
- Protokol Critical ApraisalDocument16 pagesProtokol Critical ApraisalMustika ayu lestariNo ratings yet
- 2011 Nosocomial Infections - Knowledge and Source of Information Among Clinical Health Care Students in GhanaDocument4 pages2011 Nosocomial Infections - Knowledge and Source of Information Among Clinical Health Care Students in GhanaMostafa AbdelrahmanNo ratings yet
- Roles and Responsibilitiesof A Professional NurseDocument94 pagesRoles and Responsibilitiesof A Professional Nursecassandraolson.kya07No ratings yet
- EpidemologyDocument41 pagesEpidemologyswati patanwalNo ratings yet
- Adherence To Iron Folate and Associated Factors Among Pregnant WomenDocument9 pagesAdherence To Iron Folate and Associated Factors Among Pregnant WomenBICARA JIWANo ratings yet
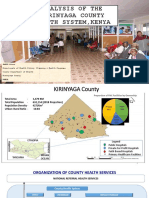
- Analysis of The Kirinyaga County Health System - Esbon - GakuuDocument18 pagesAnalysis of The Kirinyaga County Health System - Esbon - Gakuuesbon gakuu100% (1)
- Conrad Research ProposalDocument26 pagesConrad Research Proposalyvette kinyuy100% (1)
- Presentation On Nurse Specialists RolesDocument28 pagesPresentation On Nurse Specialists RolesRaphael KorkortsiNo ratings yet
- WG 3 2non CommunicableDocument337 pagesWG 3 2non CommunicableVaishnavi JayakumarNo ratings yet
- Revolutionizing HIV Prevention in Africa Landmark Innovations That Transformed The FightDocument12 pagesRevolutionizing HIV Prevention in Africa Landmark Innovations That Transformed The FightKIU PUBLICATION AND EXTENSIONNo ratings yet
- 70th Makerere Graduation Lists 2020Document99 pages70th Makerere Graduation Lists 2020miiro allanNo ratings yet
- Technologies Designed To Help Improve Patients OutcomeDocument53 pagesTechnologies Designed To Help Improve Patients OutcomeHarby Ongbay AbellanosaNo ratings yet
- Nutrition Status:: 1.direct MethodDocument8 pagesNutrition Status:: 1.direct MethodNusrat TamannaNo ratings yet
- Understanding The Psycho-Social, Health and Livelihood Problems of People Recovered From Covid-19: An Empirical StudyDocument20 pagesUnderstanding The Psycho-Social, Health and Livelihood Problems of People Recovered From Covid-19: An Empirical StudyMutluri Abraham100% (1)
- PSM Vivke JainDocument6 pagesPSM Vivke JainHouytr JikolNo ratings yet
- Seminar On Specialities in Nursing Masters and Advanced Nursing ProgramsDocument17 pagesSeminar On Specialities in Nursing Masters and Advanced Nursing ProgramsPriya SinghNo ratings yet
- Operational Guidelines For HWCDocument83 pagesOperational Guidelines For HWCharleenNo ratings yet
- Types of AnemiaDocument8 pagesTypes of AnemiaApril Mae Magos LabradorNo ratings yet
- Nosocomial InfectionDocument18 pagesNosocomial InfectionLibérée Rumagihwa100% (1)
- Infection Control Program 2020 - 2021Document9 pagesInfection Control Program 2020 - 2021HIBA OMERNo ratings yet
- Guthrie Test Is One of Screening Test For Amino Acid Especially To DetectDocument6 pagesGuthrie Test Is One of Screening Test For Amino Acid Especially To DetectAyioKunNo ratings yet
- The Use of Protocol in Breaking Bad News - Evidence and Ethos PDFDocument7 pagesThe Use of Protocol in Breaking Bad News - Evidence and Ethos PDFBayu Pratama PutraNo ratings yet
- Essay On Fast FoodDocument7 pagesEssay On Fast FoodRuslan Lan100% (1)
- National TB ControlDocument25 pagesNational TB Controlnirmal2444No ratings yet
- 7 Case Definitions of Infectious Disease in MalaysiaDocument110 pages7 Case Definitions of Infectious Disease in MalaysiaICNo ratings yet
- Primary Health Care Presented by SrikanthDocument33 pagesPrimary Health Care Presented by SrikanthHUSSAINA BANONo ratings yet
- Disaster ManagementDocument42 pagesDisaster ManagementLoma Waghmare (Jadhav)No ratings yet
- Communicable Disease Review MaterialDocument43 pagesCommunicable Disease Review Materialrceponelas1127No ratings yet
- Efficacy of Lifestyle Interventions in Patients With Type 2 Diabetes - A Systematic Review and Meta-AnalysisDocument11 pagesEfficacy of Lifestyle Interventions in Patients With Type 2 Diabetes - A Systematic Review and Meta-AnalysisDara Agusti MaulidyaNo ratings yet
- A Study of the Lack of Hiv/Aids Awareness Among African American Women: a Leadership Perspective: Awareness That All Cultures Should Know AboutFrom EverandA Study of the Lack of Hiv/Aids Awareness Among African American Women: a Leadership Perspective: Awareness That All Cultures Should Know AboutRating: 5 out of 5 stars5/5 (1)
- Role of Dietary Fibers and Nutraceuticals in Preventing DiseasesFrom EverandRole of Dietary Fibers and Nutraceuticals in Preventing DiseasesRating: 5 out of 5 stars5/5 (1)
- Winnie MomanyiDocument43 pagesWinnie MomanyiJoshua MokayaNo ratings yet
- Depo ProveraDocument2 pagesDepo ProveraJoshua MokayaNo ratings yet
- A Study To Determine Prevalence and Risk Factors Associated With Chronic Kidney Disease Among Patients Attending Renal Care Unit in Nyamira County Referral Hospital.Document46 pagesA Study To Determine Prevalence and Risk Factors Associated With Chronic Kidney Disease Among Patients Attending Renal Care Unit in Nyamira County Referral Hospital.Joshua MokayaNo ratings yet
- Kenya Medical Training College PO BOX 574-40500 Nyamira Submission Date: January 2023Document39 pagesKenya Medical Training College PO BOX 574-40500 Nyamira Submission Date: January 2023Joshua MokayaNo ratings yet
- A Study On Knowledge Attitude and Practice On Medical Waste Segregation Among Health Care Providers Nyamira County Referral HospitalDocument27 pagesA Study On Knowledge Attitude and Practice On Medical Waste Segregation Among Health Care Providers Nyamira County Referral HospitalJoshua MokayaNo ratings yet
- The Impact of Employee Remuneration and PerformanceDocument12 pagesThe Impact of Employee Remuneration and PerformanceJoshua MokayaNo ratings yet
- Factors Affecting Developmental Milestones Among Children Under Five Years Attending Child Welfare Clinic in Nyamira County Referral Hospital.Document27 pagesFactors Affecting Developmental Milestones Among Children Under Five Years Attending Child Welfare Clinic in Nyamira County Referral Hospital.Joshua MokayaNo ratings yet
- Sindi Artika (ENGLISH FOR NURSE 3. Reading)Document3 pagesSindi Artika (ENGLISH FOR NURSE 3. Reading)Artika SindiNo ratings yet
- Residual Limb Complications and Management StrategiesDocument9 pagesResidual Limb Complications and Management StrategiesTarushi TanwarNo ratings yet
- Bronchial AsthmaDocument39 pagesBronchial AsthmaSaeed mohamed100% (1)
- A Conceptual Study On Yoni PichuDocument3 pagesA Conceptual Study On Yoni PichuResearch ParkNo ratings yet
- Sci Digest Circ Respir Systems v1Document36 pagesSci Digest Circ Respir Systems v1draganNo ratings yet
- Human Physiology - The Basis of MedicineDocument2 pagesHuman Physiology - The Basis of MedicineDozzyNo ratings yet
- NCP Nutrition1Document4 pagesNCP Nutrition1java_biscocho1229100% (1)
- Dental EssayDocument3 pagesDental Essayvaleriana calaniNo ratings yet
- 2018 Abbott Annual - ReportDocument261 pages2018 Abbott Annual - Reportana cuapioNo ratings yet
- Uso Correcto de CubrebocasDocument24 pagesUso Correcto de CubrebocasMarco LeónNo ratings yet
- Fever PDFDocument2 pagesFever PDFMuhammad AkrimNo ratings yet
- Nursing Abbreviations: Aorab Aorart A&E A&P A&WDocument20 pagesNursing Abbreviations: Aorab Aorart A&E A&P A&WivahcamilleNo ratings yet
- Evolution Removable Partial Denture Design: Academics and EducationDocument9 pagesEvolution Removable Partial Denture Design: Academics and EducationSahana RangarajanNo ratings yet
- Lung Ultrasound For Critically Ill Patients - Mojoli F, Bouhemad B, Mongodi S, Lichtenstein D. (Am J Respir Crit Care Med. 2019)Document53 pagesLung Ultrasound For Critically Ill Patients - Mojoli F, Bouhemad B, Mongodi S, Lichtenstein D. (Am J Respir Crit Care Med. 2019)Mr. IncognitoNo ratings yet
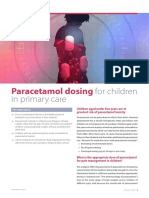
- Paracetamol Dosing: For Children in Primary CareDocument3 pagesParacetamol Dosing: For Children in Primary Careacha kyungsooNo ratings yet
- OXYTOCINDocument1 pageOXYTOCINBernardNo ratings yet
- Fisio1 Exc6 Act1Document5 pagesFisio1 Exc6 Act1Fadli Nurul HanifNo ratings yet
- Homeopathic IngredientDocument39 pagesHomeopathic IngredientJehanzeb Zeb100% (1)
- PHECC Field Guide 2011Document125 pagesPHECC Field Guide 2011Michael B. San JuanNo ratings yet
- Lab Report InheritanceDocument14 pagesLab Report InheritanceYusri RaemyNo ratings yet
- Surviving Sepsis Hour 1 Bundle InfographDocument1 pageSurviving Sepsis Hour 1 Bundle InfographLaura PutriNo ratings yet
- OutlineDocument3 pagesOutlinerabia khalidNo ratings yet
- tmp92D8 TMPDocument244 pagestmp92D8 TMPFrontiersNo ratings yet
- Transplant Hepatology: Finanacial Program OrganizationDocument37 pagesTransplant Hepatology: Finanacial Program OrganizationRobert G. Gish, MDNo ratings yet
- Lippincott's PEDIATRIC3 ANSWERSDocument8 pagesLippincott's PEDIATRIC3 ANSWERSNursyNurseNo ratings yet
- IM Injection AdultDocument1 pageIM Injection AdultDaniel TurkeyNo ratings yet
- Male Pelvic Floor - Advanced Massage and BodyworkDocument6 pagesMale Pelvic Floor - Advanced Massage and Bodyworkpujarze2No ratings yet
- Pharmacology MCQDocument46 pagesPharmacology MCQpathan mohid100% (3)
- Epidemiology of Premenstrual Syndrome (PMS) - A Systematic Review and Meta-Analysis StudyDocument4 pagesEpidemiology of Premenstrual Syndrome (PMS) - A Systematic Review and Meta-Analysis StudyPhong Triệu LêNo ratings yet






























































































Download as docx, pdf, or txt
You might also like
- Health Education Interventions For Older Adults With Hypertension: A Systematic Review and Meta-AnalysisDocument9 pagesHealth Education Interventions For Older Adults With Hypertension: A Systematic Review and Meta-AnalysisJosé Carlos Sánchez-RamirezNo ratings yet
- IC 13 Guidelines On Standards For High Dependency UnitsDocument4 pagesIC 13 Guidelines On Standards For High Dependency UnitsAnonymous 0WHX7nNo ratings yet
- Angelina Alphonce JohoDocument80 pagesAngelina Alphonce JohoMerlina WijayawatiNo ratings yet
- Final Research ProposalDocument20 pagesFinal Research ProposalNatnael G.No ratings yet
- Factors Affecting Management of Sickle Cell Disease Among Children 0-12 Years Attending Nakaseke Sickle Cell ClinicDocument66 pagesFactors Affecting Management of Sickle Cell Disease Among Children 0-12 Years Attending Nakaseke Sickle Cell Clinicbaluku yosiah100% (1)
- Literature Review On Diabetes PDFDocument4 pagesLiterature Review On Diabetes PDFklbndecnd100% (1)
- Research ProposalDocument24 pagesResearch ProposalLorraine ZarateNo ratings yet
- NCD National PolicyDocument14 pagesNCD National PolicyHerlene Lyneth ZalamedaNo ratings yet
- Assessment of Awareness of Diabetic Retinopathy Among Type 2 Diabetes Mellitus Cross Sectional Study From Central IndiaDocument7 pagesAssessment of Awareness of Diabetic Retinopathy Among Type 2 Diabetes Mellitus Cross Sectional Study From Central IndiaAthenaeum Scientific PublishersNo ratings yet
- Final Pint ResearchDocument90 pagesFinal Pint ResearchNhelia Santos BañagaNo ratings yet
- IPD Patient History ChecklistDocument2 pagesIPD Patient History ChecklistdrjriNo ratings yet
- Basic Public Health (1) - MergedDocument89 pagesBasic Public Health (1) - Mergedrimsha tariqNo ratings yet
- Management of Vacuum Assisted Closure TherapyDocument14 pagesManagement of Vacuum Assisted Closure TherapyVoiculescu MihaelaNo ratings yet
- Barriers To Access Quality Healthcare Services Among Physically Challenged Persons in Gem Sub County, Siaya County'Document9 pagesBarriers To Access Quality Healthcare Services Among Physically Challenged Persons in Gem Sub County, Siaya County'Premier PublishersNo ratings yet
- Marylin's ProjectDocument84 pagesMarylin's ProjectDavid UdohNo ratings yet
- Edited Research ProposalDocument20 pagesEdited Research ProposalNestoryNo ratings yet
- Under Nutrition and Its Associated Factors Among Adolescent Girls in Rural Community of Aseko District, Eastern Arsi Zone, Oromia Region, Eastern Ethiopia, 2017Document10 pagesUnder Nutrition and Its Associated Factors Among Adolescent Girls in Rural Community of Aseko District, Eastern Arsi Zone, Oromia Region, Eastern Ethiopia, 2017Anonymous SMEU6r2No ratings yet
- JBDS Oncology Guideline Final Revised September 2021Document57 pagesJBDS Oncology Guideline Final Revised September 2021Majid KhanNo ratings yet
- Nancy,,, GITARI PROJECTDocument46 pagesNancy,,, GITARI PROJECTjohn mwambuNo ratings yet
- RMNCAH Quality Improvement QI FrameworkDocument82 pagesRMNCAH Quality Improvement QI FrameworkShahidul Islam ChowdhuryNo ratings yet
- KAP Analysis of Covid-19Document9 pagesKAP Analysis of Covid-19Bhaskar ReddyNo ratings yet
- Antihypertension Non AdherenceDocument16 pagesAntihypertension Non AdherencebezieNo ratings yet
- WDF14-852 Draft Guidelines TB-DM 07-01-2015Document20 pagesWDF14-852 Draft Guidelines TB-DM 07-01-2015adindadian12No ratings yet
- Synopsis 8TH AAAAaaDocument19 pagesSynopsis 8TH AAAAaaعثمان علیNo ratings yet
- Research ProposalDocument21 pagesResearch ProposalBeatrice KarimiNo ratings yet
- IdrvDocument39 pagesIdrvMyk MacalintalNo ratings yet
- Diet and Exercise in Management of Obesity and OveDocument6 pagesDiet and Exercise in Management of Obesity and OveXavi Martinez SantamariaNo ratings yet
- Trends in Nursing PracticeDocument12 pagesTrends in Nursing PracticeJerome Cid100% (1)
- Adeliana Joseph KJDocument29 pagesAdeliana Joseph KJNyagawa GodkNo ratings yet
- Health IndicatorDocument30 pagesHealth IndicatorPawan KumarNo ratings yet
- Protokol Critical ApraisalDocument16 pagesProtokol Critical ApraisalMustika ayu lestariNo ratings yet
- 2011 Nosocomial Infections - Knowledge and Source of Information Among Clinical Health Care Students in GhanaDocument4 pages2011 Nosocomial Infections - Knowledge and Source of Information Among Clinical Health Care Students in GhanaMostafa AbdelrahmanNo ratings yet
- Roles and Responsibilitiesof A Professional NurseDocument94 pagesRoles and Responsibilitiesof A Professional Nursecassandraolson.kya07No ratings yet
- EpidemologyDocument41 pagesEpidemologyswati patanwalNo ratings yet
- Adherence To Iron Folate and Associated Factors Among Pregnant WomenDocument9 pagesAdherence To Iron Folate and Associated Factors Among Pregnant WomenBICARA JIWANo ratings yet
- Analysis of The Kirinyaga County Health System - Esbon - GakuuDocument18 pagesAnalysis of The Kirinyaga County Health System - Esbon - Gakuuesbon gakuu100% (1)
- Conrad Research ProposalDocument26 pagesConrad Research Proposalyvette kinyuy100% (1)
- Presentation On Nurse Specialists RolesDocument28 pagesPresentation On Nurse Specialists RolesRaphael KorkortsiNo ratings yet
- WG 3 2non CommunicableDocument337 pagesWG 3 2non CommunicableVaishnavi JayakumarNo ratings yet
- Revolutionizing HIV Prevention in Africa Landmark Innovations That Transformed The FightDocument12 pagesRevolutionizing HIV Prevention in Africa Landmark Innovations That Transformed The FightKIU PUBLICATION AND EXTENSIONNo ratings yet
- 70th Makerere Graduation Lists 2020Document99 pages70th Makerere Graduation Lists 2020miiro allanNo ratings yet
- Technologies Designed To Help Improve Patients OutcomeDocument53 pagesTechnologies Designed To Help Improve Patients OutcomeHarby Ongbay AbellanosaNo ratings yet
- Nutrition Status:: 1.direct MethodDocument8 pagesNutrition Status:: 1.direct MethodNusrat TamannaNo ratings yet
- Understanding The Psycho-Social, Health and Livelihood Problems of People Recovered From Covid-19: An Empirical StudyDocument20 pagesUnderstanding The Psycho-Social, Health and Livelihood Problems of People Recovered From Covid-19: An Empirical StudyMutluri Abraham100% (1)
- PSM Vivke JainDocument6 pagesPSM Vivke JainHouytr JikolNo ratings yet
- Seminar On Specialities in Nursing Masters and Advanced Nursing ProgramsDocument17 pagesSeminar On Specialities in Nursing Masters and Advanced Nursing ProgramsPriya SinghNo ratings yet
- Operational Guidelines For HWCDocument83 pagesOperational Guidelines For HWCharleenNo ratings yet
- Types of AnemiaDocument8 pagesTypes of AnemiaApril Mae Magos LabradorNo ratings yet
- Nosocomial InfectionDocument18 pagesNosocomial InfectionLibérée Rumagihwa100% (1)
- Infection Control Program 2020 - 2021Document9 pagesInfection Control Program 2020 - 2021HIBA OMERNo ratings yet
- Guthrie Test Is One of Screening Test For Amino Acid Especially To DetectDocument6 pagesGuthrie Test Is One of Screening Test For Amino Acid Especially To DetectAyioKunNo ratings yet
- The Use of Protocol in Breaking Bad News - Evidence and Ethos PDFDocument7 pagesThe Use of Protocol in Breaking Bad News - Evidence and Ethos PDFBayu Pratama PutraNo ratings yet
- Essay On Fast FoodDocument7 pagesEssay On Fast FoodRuslan Lan100% (1)
- National TB ControlDocument25 pagesNational TB Controlnirmal2444No ratings yet
- 7 Case Definitions of Infectious Disease in MalaysiaDocument110 pages7 Case Definitions of Infectious Disease in MalaysiaICNo ratings yet
- Primary Health Care Presented by SrikanthDocument33 pagesPrimary Health Care Presented by SrikanthHUSSAINA BANONo ratings yet
- Disaster ManagementDocument42 pagesDisaster ManagementLoma Waghmare (Jadhav)No ratings yet
- Communicable Disease Review MaterialDocument43 pagesCommunicable Disease Review Materialrceponelas1127No ratings yet
- Efficacy of Lifestyle Interventions in Patients With Type 2 Diabetes - A Systematic Review and Meta-AnalysisDocument11 pagesEfficacy of Lifestyle Interventions in Patients With Type 2 Diabetes - A Systematic Review and Meta-AnalysisDara Agusti MaulidyaNo ratings yet
- A Study of the Lack of Hiv/Aids Awareness Among African American Women: a Leadership Perspective: Awareness That All Cultures Should Know AboutFrom EverandA Study of the Lack of Hiv/Aids Awareness Among African American Women: a Leadership Perspective: Awareness That All Cultures Should Know AboutRating: 5 out of 5 stars5/5 (1)
- Role of Dietary Fibers and Nutraceuticals in Preventing DiseasesFrom EverandRole of Dietary Fibers and Nutraceuticals in Preventing DiseasesRating: 5 out of 5 stars5/5 (1)
- Winnie MomanyiDocument43 pagesWinnie MomanyiJoshua MokayaNo ratings yet
- Depo ProveraDocument2 pagesDepo ProveraJoshua MokayaNo ratings yet
- A Study To Determine Prevalence and Risk Factors Associated With Chronic Kidney Disease Among Patients Attending Renal Care Unit in Nyamira County Referral Hospital.Document46 pagesA Study To Determine Prevalence and Risk Factors Associated With Chronic Kidney Disease Among Patients Attending Renal Care Unit in Nyamira County Referral Hospital.Joshua MokayaNo ratings yet
- Kenya Medical Training College PO BOX 574-40500 Nyamira Submission Date: January 2023Document39 pagesKenya Medical Training College PO BOX 574-40500 Nyamira Submission Date: January 2023Joshua MokayaNo ratings yet
- A Study On Knowledge Attitude and Practice On Medical Waste Segregation Among Health Care Providers Nyamira County Referral HospitalDocument27 pagesA Study On Knowledge Attitude and Practice On Medical Waste Segregation Among Health Care Providers Nyamira County Referral HospitalJoshua MokayaNo ratings yet
- The Impact of Employee Remuneration and PerformanceDocument12 pagesThe Impact of Employee Remuneration and PerformanceJoshua MokayaNo ratings yet
- Factors Affecting Developmental Milestones Among Children Under Five Years Attending Child Welfare Clinic in Nyamira County Referral Hospital.Document27 pagesFactors Affecting Developmental Milestones Among Children Under Five Years Attending Child Welfare Clinic in Nyamira County Referral Hospital.Joshua MokayaNo ratings yet
- Sindi Artika (ENGLISH FOR NURSE 3. Reading)Document3 pagesSindi Artika (ENGLISH FOR NURSE 3. Reading)Artika SindiNo ratings yet
- Residual Limb Complications and Management StrategiesDocument9 pagesResidual Limb Complications and Management StrategiesTarushi TanwarNo ratings yet
- Bronchial AsthmaDocument39 pagesBronchial AsthmaSaeed mohamed100% (1)
- A Conceptual Study On Yoni PichuDocument3 pagesA Conceptual Study On Yoni PichuResearch ParkNo ratings yet
- Sci Digest Circ Respir Systems v1Document36 pagesSci Digest Circ Respir Systems v1draganNo ratings yet
- Human Physiology - The Basis of MedicineDocument2 pagesHuman Physiology - The Basis of MedicineDozzyNo ratings yet
- NCP Nutrition1Document4 pagesNCP Nutrition1java_biscocho1229100% (1)
- Dental EssayDocument3 pagesDental Essayvaleriana calaniNo ratings yet
- 2018 Abbott Annual - ReportDocument261 pages2018 Abbott Annual - Reportana cuapioNo ratings yet
- Uso Correcto de CubrebocasDocument24 pagesUso Correcto de CubrebocasMarco LeónNo ratings yet
- Fever PDFDocument2 pagesFever PDFMuhammad AkrimNo ratings yet
- Nursing Abbreviations: Aorab Aorart A&E A&P A&WDocument20 pagesNursing Abbreviations: Aorab Aorart A&E A&P A&WivahcamilleNo ratings yet
- Evolution Removable Partial Denture Design: Academics and EducationDocument9 pagesEvolution Removable Partial Denture Design: Academics and EducationSahana RangarajanNo ratings yet
- Lung Ultrasound For Critically Ill Patients - Mojoli F, Bouhemad B, Mongodi S, Lichtenstein D. (Am J Respir Crit Care Med. 2019)Document53 pagesLung Ultrasound For Critically Ill Patients - Mojoli F, Bouhemad B, Mongodi S, Lichtenstein D. (Am J Respir Crit Care Med. 2019)Mr. IncognitoNo ratings yet
- Paracetamol Dosing: For Children in Primary CareDocument3 pagesParacetamol Dosing: For Children in Primary Careacha kyungsooNo ratings yet
- OXYTOCINDocument1 pageOXYTOCINBernardNo ratings yet
- Fisio1 Exc6 Act1Document5 pagesFisio1 Exc6 Act1Fadli Nurul HanifNo ratings yet
- Homeopathic IngredientDocument39 pagesHomeopathic IngredientJehanzeb Zeb100% (1)
- PHECC Field Guide 2011Document125 pagesPHECC Field Guide 2011Michael B. San JuanNo ratings yet
- Lab Report InheritanceDocument14 pagesLab Report InheritanceYusri RaemyNo ratings yet
- Surviving Sepsis Hour 1 Bundle InfographDocument1 pageSurviving Sepsis Hour 1 Bundle InfographLaura PutriNo ratings yet
- OutlineDocument3 pagesOutlinerabia khalidNo ratings yet
- tmp92D8 TMPDocument244 pagestmp92D8 TMPFrontiersNo ratings yet
- Transplant Hepatology: Finanacial Program OrganizationDocument37 pagesTransplant Hepatology: Finanacial Program OrganizationRobert G. Gish, MDNo ratings yet
- Lippincott's PEDIATRIC3 ANSWERSDocument8 pagesLippincott's PEDIATRIC3 ANSWERSNursyNurseNo ratings yet
- IM Injection AdultDocument1 pageIM Injection AdultDaniel TurkeyNo ratings yet
- Male Pelvic Floor - Advanced Massage and BodyworkDocument6 pagesMale Pelvic Floor - Advanced Massage and Bodyworkpujarze2No ratings yet
- Pharmacology MCQDocument46 pagesPharmacology MCQpathan mohid100% (3)
- Epidemiology of Premenstrual Syndrome (PMS) - A Systematic Review and Meta-Analysis StudyDocument4 pagesEpidemiology of Premenstrual Syndrome (PMS) - A Systematic Review and Meta-Analysis StudyPhong Triệu LêNo ratings yet