Download as pdf or txt
You might also like
- Instructions: After Visit SummaryDocument10 pagesInstructions: After Visit SummaryKelly Arington McgrealNo ratings yet
- The Pocketbook For PHYSIOTHERAPISTS 2nd Gitesh Amrohit Masud PDFDocument408 pagesThe Pocketbook For PHYSIOTHERAPISTS 2nd Gitesh Amrohit Masud PDFemil100% (1)
- Efectoas Adversos AtbDocument13 pagesEfectoas Adversos AtbAgueda MaribelNo ratings yet
- Brit J Clinical Pharma - 2012 - Thomas - An Agenda For UK Clinical Pharmacology Developing and Delivering ClinicalDocument6 pagesBrit J Clinical Pharma - 2012 - Thomas - An Agenda For UK Clinical Pharmacology Developing and Delivering Clinicalwzy76k484hNo ratings yet
- Organophosphate PoisoningDocument7 pagesOrganophosphate PoisoningCLAUDIANo ratings yet
- Fatal Case of Diazepam and Paraquat Poisoning - A Case Report PDFDocument4 pagesFatal Case of Diazepam and Paraquat Poisoning - A Case Report PDFamelameilindaNo ratings yet
- AbriefguidetoadrsDocument5 pagesAbriefguidetoadrsSri HariNo ratings yet
- 392 3 FullDocument2 pages392 3 FullMohammed A MalkawiNo ratings yet
- Drug-Induced Pulmonary DiseaseDocument11 pagesDrug-Induced Pulmonary Diseasetmlicha2No ratings yet
- Unknown Overdose Emerg Med Clin N Am 2007 Erickson (May-22-08)Document33 pagesUnknown Overdose Emerg Med Clin N Am 2007 Erickson (May-22-08)khizerabbasi708No ratings yet
- Cyclophosphamide ToxicityDocument15 pagesCyclophosphamide ToxicityAnonymous 9dVZCnTXSNo ratings yet
- J of Gastro and Hepatol - 2007 - Tostmann - Antituberculosis Drug Induced Hepatotoxicity Concise Up To Date ReviewDocument12 pagesJ of Gastro and Hepatol - 2007 - Tostmann - Antituberculosis Drug Induced Hepatotoxicity Concise Up To Date ReviewputryaNo ratings yet
- Management of Sars Cov2 Infection - Related Digestive DisordersDocument2 pagesManagement of Sars Cov2 Infection - Related Digestive DisordersAdam BennaniNo ratings yet
- Intl Journal of Cancer - 2014 - Landeck - Handling Chemotherapy Drugs Do Medical Gloves Really ProtectDocument6 pagesIntl Journal of Cancer - 2014 - Landeck - Handling Chemotherapy Drugs Do Medical Gloves Really ProtectPhạm Thu HuyềnNo ratings yet
- Prescriber - 2011 - Meisner - Current Treatments For Lower Respiratory Tract inDocument16 pagesPrescriber - 2011 - Meisner - Current Treatments For Lower Respiratory Tract inamanabduwahabNo ratings yet
- International Journal of Basic & Clinical Pharmacology: IjbcpDocument7 pagesInternational Journal of Basic & Clinical Pharmacology: IjbcpDiego GomezNo ratings yet
- Poisoning TreatmentDocument8 pagesPoisoning TreatmentNosheen HafeezNo ratings yet
- The Aproach To The Patient With An Unknow Overdose, Clin Nort 2007Document33 pagesThe Aproach To The Patient With An Unknow Overdose, Clin Nort 2007Diego AmaguaNo ratings yet
- Insights Into Doxorubicin-Induced Cardiotoxicity MolecularDocument14 pagesInsights Into Doxorubicin-Induced Cardiotoxicity MolecularRania T. SabriNo ratings yet
- The Epidemiology of Poisoning: Table 1Document4 pagesThe Epidemiology of Poisoning: Table 1Pin Han NaNo ratings yet
- Managing Amphetamine Dependence: Malcolm BruceDocument8 pagesManaging Amphetamine Dependence: Malcolm BrucejuraiddinNo ratings yet
- Illicit Substances AAGBI 2013Document8 pagesIllicit Substances AAGBI 2013yuyoide6857No ratings yet
- Drug-Induced QT Prolongation and Torsades de Pointes: Matthew Li, Pharmd and Liz G. Ramos, Pharmd, BcpsDocument5 pagesDrug-Induced QT Prolongation and Torsades de Pointes: Matthew Li, Pharmd and Liz G. Ramos, Pharmd, BcpsCalon DokterNo ratings yet
- Introduction & Gen Management of Toxic ConditionsDocument12 pagesIntroduction & Gen Management of Toxic Conditionsblue sapphireNo ratings yet
- Relevant Pharmacological Interactions Between Alkylating Agents and Antiepileptic Drugs: Preclinical and Clinical DataDocument13 pagesRelevant Pharmacological Interactions Between Alkylating Agents and Antiepileptic Drugs: Preclinical and Clinical DataFederico CucchiaraNo ratings yet
- ADR Medicine 36 7 2008Document5 pagesADR Medicine 36 7 2008Indri WidyantiNo ratings yet
- Clinical Practice GuidelinesDocument6 pagesClinical Practice GuidelinesDiana MaicanNo ratings yet
- Cyanide PoisoningDocument5 pagesCyanide Poisoningriz04_fortitudessa5178No ratings yet
- Arritmias Cardiacas Inducidas Por AntibioticosDocument7 pagesArritmias Cardiacas Inducidas Por AntibioticosIrving Torres LópezNo ratings yet
- 150 Years of PharmacovigilanceDocument2 pages150 Years of PharmacovigilanceCarlos José Lacava Fernández100% (1)
- JHMVol16No8 Cohen10740818eDocument4 pagesJHMVol16No8 Cohen10740818eGiancarlo SanteNo ratings yet
- Geria ToxicidadDocument9 pagesGeria ToxicidadGh RossiNo ratings yet
- UKMi QA - Naloxone-Dosing Aug-17 FINAL PDFDocument22 pagesUKMi QA - Naloxone-Dosing Aug-17 FINAL PDFAyman MustafaNo ratings yet
- Prescribing in Patients With Liver Disease: Rakesh K TandonDocument4 pagesPrescribing in Patients With Liver Disease: Rakesh K Tandonjoydeep chakrabortyNo ratings yet
- Stein 2009Document14 pagesStein 2009Med ZinNo ratings yet
- Predicting Acute Complicated Glyphosate Intoxication in The Emergency DepartmentDocument7 pagesPredicting Acute Complicated Glyphosate Intoxication in The Emergency DepartmentTuan LeNo ratings yet
- Litt's Drug Eruption Reference Manual Including Drug Interactions, 13th Edition (Litt's Drug Eruption Reference Manual_ Including Drug Interactions)Document801 pagesLitt's Drug Eruption Reference Manual Including Drug Interactions, 13th Edition (Litt's Drug Eruption Reference Manual_ Including Drug Interactions)amnaakb197No ratings yet
- Faught Et Al-2015-British Journal of Clinical PharmacologyDocument9 pagesFaught Et Al-2015-British Journal of Clinical PharmacologyHendra Wana Nur'aminNo ratings yet
- MainDocument6 pagesMainkamila sNo ratings yet
- LASTDocument10 pagesLASTAgus RiyantoNo ratings yet
- ArtikelDocument3 pagesArtikelJuniver Jhu-Jhu ParapagaNo ratings yet
- Chapter 1: IntroductionDocument27 pagesChapter 1: IntroductionkevinNo ratings yet
- What's New For Fluoroquinolones in The Treatment of Acute Bacterial Skin and Skin Structure InfectionsDocument4 pagesWhat's New For Fluoroquinolones in The Treatment of Acute Bacterial Skin and Skin Structure InfectionsMoisés PonceNo ratings yet
- 2008 - Antituberculosis Drug-Induced Hepatotoxicity Concise Up-To-Date ReviewDocument12 pages2008 - Antituberculosis Drug-Induced Hepatotoxicity Concise Up-To-Date ReviewCarlos LuqueNo ratings yet
- Clinical ToxicologyDocument17 pagesClinical ToxicologyElfahra Casanza Amalda100% (1)
- The More Patients You TreatDocument14 pagesThe More Patients You TreatJulita MelisaNo ratings yet
- Aluminium PhosphideDocument5 pagesAluminium PhosphideMuhammad ZeeshanNo ratings yet
- Emerging Drugs of AbuseDocument4 pagesEmerging Drugs of AbuseKhaled KhapiNo ratings yet
- IntoxicationDocument10 pagesIntoxicationEmőke MátyásNo ratings yet
- Patton Et Al 2018 AnaesthesiaDocument9 pagesPatton Et Al 2018 AnaesthesiadiegoNo ratings yet
- Oral Anticoagulants Beyond WarfarinDocument25 pagesOral Anticoagulants Beyond Warfarinmyqrwd464kNo ratings yet
- Predictors of Morbidities in Organophosphate PoisoningDocument17 pagesPredictors of Morbidities in Organophosphate PoisoningInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Apostila R2Document469 pagesApostila R2Lucas TheotonioNo ratings yet
- Three Serious Drug Interactions That Every Dentist Should Know AboutDocument8 pagesThree Serious Drug Interactions That Every Dentist Should Know AboutDaniela Paulina Riveros DonosoNo ratings yet
- PN 2023 003817.fullDocument15 pagesPN 2023 003817.fullHenrique OliveiraNo ratings yet
- A Case Report and Overview of Organophosphate (OP) PoisoningDocument5 pagesA Case Report and Overview of Organophosphate (OP) PoisoningDhruva PatelNo ratings yet
- Chemicalagentsindisaster: Care and Management in The Intensive Care UnitDocument13 pagesChemicalagentsindisaster: Care and Management in The Intensive Care Unitgarinda almadutaNo ratings yet
- FGA Medical Management Guidelines 508Document21 pagesFGA Medical Management Guidelines 508epraetorianNo ratings yet
- Brit J Clinical Pharma - 2013 - Verhoef - Pharmacogenetic Guided Dosing of Coumarin Anticoagulants Algorithms For WarfarinDocument16 pagesBrit J Clinical Pharma - 2013 - Verhoef - Pharmacogenetic Guided Dosing of Coumarin Anticoagulants Algorithms For WarfarinSusana RocheNo ratings yet
- Dangerous Drug InteractionsDocument27 pagesDangerous Drug InteractionsriniambarwatiNo ratings yet
- Drug-Induced Oral ComplicationsFrom EverandDrug-Induced Oral ComplicationsSarah CoustyNo ratings yet
- Nuclear Medicine Therapy: Principles and Clinical ApplicationsFrom EverandNuclear Medicine Therapy: Principles and Clinical ApplicationsNo ratings yet
- Physiol 93 B3Document1 pagePhysiol 93 B3DonkeyManNo ratings yet
- Pharm 00 B14Document2 pagesPharm 00 B14DonkeyManNo ratings yet
- Cellular Physiology SAQsDocument1 pageCellular Physiology SAQsDonkeyManNo ratings yet
- CEACCP - Latex AllergyDocument4 pagesCEACCP - Latex AllergyDonkeyManNo ratings yet
- CEACCP - KetamineDocument5 pagesCEACCP - KetamineDonkeyManNo ratings yet
- Pharm 02 A10Document2 pagesPharm 02 A10DonkeyManNo ratings yet
- CEACCP - Intrathecal Opioids in The Management of Acute Postoperative PainDocument5 pagesCEACCP - Intrathecal Opioids in The Management of Acute Postoperative PainDonkeyManNo ratings yet
- Pharmacodynamics, Drug Action Targets, PharmacogeneticsDocument21 pagesPharmacodynamics, Drug Action Targets, PharmacogeneticsDonkeyManNo ratings yet
- Pharm 02 A11Document4 pagesPharm 02 A11DonkeyManNo ratings yet
- Pharm 00 B11Document1 pagePharm 00 B11DonkeyManNo ratings yet
- Pharm 00 B15Document2 pagesPharm 00 B15DonkeyManNo ratings yet
- Pharm 00 A9Document2 pagesPharm 00 A9DonkeyManNo ratings yet
- Pharm 00 A14Document2 pagesPharm 00 A14DonkeyManNo ratings yet
- Pharm 00 A12Document1 pagePharm 00 A12DonkeyManNo ratings yet
- Pharm 00 A15Document2 pagesPharm 00 A15DonkeyManNo ratings yet
- Define The Mechanisms of Action and Adverse Effects of Metoprolol, GTN, and Diltiazem When Used To Manage MIDocument2 pagesDefine The Mechanisms of Action and Adverse Effects of Metoprolol, GTN, and Diltiazem When Used To Manage MIDonkeyManNo ratings yet
- Outline The Physiological Consequences of Hyperosmolar Diabetic KetoacidosisDocument2 pagesOutline The Physiological Consequences of Hyperosmolar Diabetic KetoacidosisDonkeyManNo ratings yet
- Compare and Contrast The Pharamcology of Ephedrine and NoradrenalineDocument1 pageCompare and Contrast The Pharamcology of Ephedrine and NoradrenalineDonkeyManNo ratings yet
- Compare and Contrast The Pharmacology of Esmolol and PropanololDocument1 pageCompare and Contrast The Pharmacology of Esmolol and PropanololDonkeyManNo ratings yet
- Compare and Contrast Neostigmine and The Organophosphate CompoundsDocument1 pageCompare and Contrast Neostigmine and The Organophosphate CompoundsDonkeyManNo ratings yet
- Compare and Contrast Atropine and Glycopyrulate, and Discuss The Clinical ImplicationsDocument2 pagesCompare and Contrast Atropine and Glycopyrulate, and Discuss The Clinical ImplicationsDonkeyManNo ratings yet
- Palliative Care HandbookDocument82 pagesPalliative Care HandbookDonkeyManNo ratings yet
- Cholinergic Agents: Cholinergic Receptors Types of Receptor Muscarinic Receptor Nicotinic ReceptorDocument4 pagesCholinergic Agents: Cholinergic Receptors Types of Receptor Muscarinic Receptor Nicotinic ReceptorDonkeyManNo ratings yet
- VOLATILEAGENTSDocument4 pagesVOLATILEAGENTSDonkeyManNo ratings yet
- Base Excess (Be) Measure of Metabolic Acid-Base Status: Dr. David LynessDocument1 pageBase Excess (Be) Measure of Metabolic Acid-Base Status: Dr. David LynessDonkeyManNo ratings yet
- FS Antimicrobial Dosing Obesity AMS Updates Issue4 - Nov2018Document4 pagesFS Antimicrobial Dosing Obesity AMS Updates Issue4 - Nov2018DonkeyManNo ratings yet
- The Physiology of The GIT and The Liver QuestionsDocument44 pagesThe Physiology of The GIT and The Liver QuestionsDonkeyManNo ratings yet
- Comparative Pharmacokinetics of Fentanyl and Alfentanil: Br. J. Anaesth. (1982), 54, 871Document7 pagesComparative Pharmacokinetics of Fentanyl and Alfentanil: Br. J. Anaesth. (1982), 54, 871DonkeyManNo ratings yet
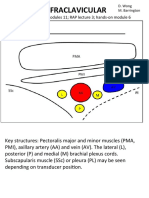
- Infraclavicular: Toolbox: Online Modules 11 RAP Lecture 3 Hands - On Module 6Document4 pagesInfraclavicular: Toolbox: Online Modules 11 RAP Lecture 3 Hands - On Module 6DonkeyManNo ratings yet
- Management of Mixed PainDocument19 pagesManagement of Mixed PainGita FitrianiNo ratings yet
- Hemorrhoids (Final Draft)Document40 pagesHemorrhoids (Final Draft)Orville Villacete50% (2)
- Trimebutine: Drug Delivery Systems IiDocument12 pagesTrimebutine: Drug Delivery Systems Iimerve yamanNo ratings yet
- LoperamideDocument5 pagesLoperamideErick TriardiantoNo ratings yet
- Potts Disease Case AnalysisDocument5 pagesPotts Disease Case AnalysisAdrian MallarNo ratings yet
- Poa Forensic ChemistryDocument21 pagesPoa Forensic ChemistryReizel GaasNo ratings yet
- Drug Study NubainDocument2 pagesDrug Study NubainNylia Atibi100% (1)
- 8th Mid McqsDocument25 pages8th Mid McqsMuhammad Uzair GujjarNo ratings yet
- Does Kratom Show Up On A Drug TestDocument5 pagesDoes Kratom Show Up On A Drug TestHimanshu SharmaNo ratings yet
- Week 6 - Antiparkinsonism AgentsDocument18 pagesWeek 6 - Antiparkinsonism AgentsDino MicaNo ratings yet
- A ThingDocument158 pagesA ThingJillian LilasNo ratings yet
- Dr. Ali's Uworld Notes For Step 2 CKDocument6 pagesDr. Ali's Uworld Notes For Step 2 CKuyesNo ratings yet
- Mechanism of Action For Psychiatric Drugs - EditedDocument6 pagesMechanism of Action For Psychiatric Drugs - EditedPawel kNo ratings yet
- NICE GuidelineDocument30 pagesNICE GuidelineRalucaNo ratings yet
- LDN PDFDocument434 pagesLDN PDFSatyam PatelNo ratings yet
- Pain ManagementDocument162 pagesPain ManagementFASIKAW GIZAWNo ratings yet
- 2001 Pharmacology McqsDocument10 pages2001 Pharmacology McqsKenneth MiguelNo ratings yet
- Guidelines On Management of Postoperative Pain PDFDocument27 pagesGuidelines On Management of Postoperative Pain PDFMarcoNo ratings yet
- Analgesics - Uses, Treatment, RisksDocument5 pagesAnalgesics - Uses, Treatment, RisksHonour JamesNo ratings yet
- Menadment of PainDocument4 pagesMenadment of PainMirza CoricNo ratings yet
- Opioid Reduction Act SummaryDocument2 pagesOpioid Reduction Act SummaryU.S. Senator Tim KaineNo ratings yet
- Drug Study 1Document4 pagesDrug Study 1bibet_martijaNo ratings yet
- HNN215 Drug DiaryDocument10 pagesHNN215 Drug DiaryMaddison MitchellNo ratings yet
- Management of Opioid Withdrawal and Relapse PreventionDocument34 pagesManagement of Opioid Withdrawal and Relapse PreventionJared KeburiNo ratings yet
- Makalah Bahasa InggrisDocument14 pagesMakalah Bahasa InggrisFadhil Zulian AliNo ratings yet
- Post Anaesthesia Shivering - N PadayacheeDocument19 pagesPost Anaesthesia Shivering - N Padayacheexxxvrgnt100% (2)
- For Prescribers - New Limits On Prescription Opioids For Acute PainDocument2 pagesFor Prescribers - New Limits On Prescription Opioids For Acute PainKyle HuaNo ratings yet
- Wa0014.Document18 pagesWa0014.Asma ShoukatNo ratings yet