Download as pdf or txt
You might also like
- Good Night, Sleep Tight PDFDocument20 pagesGood Night, Sleep Tight PDFghetzushu0% (3)
- Sleeping Through the Night, Revised Edition: How Infants, Toddlers, and Parents can get a Good Night's sleepFrom EverandSleeping Through the Night, Revised Edition: How Infants, Toddlers, and Parents can get a Good Night's sleepRating: 3.5 out of 5 stars3.5/5 (21)
- For Information Only, Will Not Be Exchanged When Altered!: Spare Parts ListDocument13 pagesFor Information Only, Will Not Be Exchanged When Altered!: Spare Parts Listhorica7167% (3)
- Access Your ConsciousnessDocument28 pagesAccess Your ConsciousnessReikiportal100% (4)
- BabySleepSite ToddlerSleepSecretsDocument13 pagesBabySleepSite ToddlerSleepSecretsMaryam Haruna YahyaNo ratings yet
- 10 Things Great Sleepers DoDocument24 pages10 Things Great Sleepers DoCesar AraucoNo ratings yet
- 4 Sleep The Gentle TyrantDocument7 pages4 Sleep The Gentle TyrantVivek KushwahaNo ratings yet
- Exploring Sensory Processing Approaches To Address Sleep in ChildrenDocument30 pagesExploring Sensory Processing Approaches To Address Sleep in Childrencarla caroline AraujoNo ratings yet
- Speakout Reading and Listening Extra Advanced Plus Unit 8Document2 pagesSpeakout Reading and Listening Extra Advanced Plus Unit 8Margaridavieira97No ratings yet
- Effects of Sleep Deprivation To The TeenagersDocument19 pagesEffects of Sleep Deprivation To The TeenagersACE BRIANNo ratings yet
- Sweet Dreams: The Power of SleepDocument3 pagesSweet Dreams: The Power of Sleepleangchhiv chheNo ratings yet
- Desordenes Del SueñoDocument8 pagesDesordenes Del SueñoelresidenteNo ratings yet
- Sleep Neurobiology 2Document26 pagesSleep Neurobiology 2kaynnanathosNo ratings yet
- Getting Your Child To Sleep and Back to Sleep: Tips for Parents of Infants, Toddlers and PreschoolersFrom EverandGetting Your Child To Sleep and Back to Sleep: Tips for Parents of Infants, Toddlers and PreschoolersNo ratings yet
- Sleeping Through the Night: How Infants, Toddlers, and Their ParentsFrom EverandSleeping Through the Night: How Infants, Toddlers, and Their ParentsRating: 4 out of 5 stars4/5 (15)
- The Absolute Essentials of Sleep Knowledge (Mini Book)Document63 pagesThe Absolute Essentials of Sleep Knowledge (Mini Book)Sajad MahyaeiNo ratings yet
- Psychology Project SleepwalkingDocument3 pagesPsychology Project Sleepwalkingluis pinedaNo ratings yet
- What Does Science Have To Say About Self Soothing Babies 3Document1 pageWhat Does Science Have To Say About Self Soothing Babies 3Nj NjNo ratings yet
- Brain Basics Sleep 6 10 08 PDF 508 PDFDocument16 pagesBrain Basics Sleep 6 10 08 PDF 508 PDFYrah Gaille VasquezNo ratings yet
- MysterySleep PDFDocument15 pagesMysterySleep PDFNadir AzizNo ratings yet
- Sleep Problems and Sleep Disorders in School Aged ChildrenDocument3 pagesSleep Problems and Sleep Disorders in School Aged ChildrenJackTVNo ratings yet
- DreamDocument13 pagesDreamapi-609508246No ratings yet
- 4 Quick Fixes For Your Sleep Problems: Doctor Formulated SupplementsDocument12 pages4 Quick Fixes For Your Sleep Problems: Doctor Formulated SupplementsjilujNo ratings yet
- BBTI Deck Slide HandoutDocument177 pagesBBTI Deck Slide HandoutteganmichlNo ratings yet
- Nightmares Vs Night TerrorsDocument4 pagesNightmares Vs Night TerrorslindiNo ratings yet
- Every Mind Matters Sleep Presentation KS34Document16 pagesEvery Mind Matters Sleep Presentation KS34Domingo de LeonNo ratings yet
- Iapp Naskar Sleep 2022Document45 pagesIapp Naskar Sleep 2022Dr. Subrata NaskarNo ratings yet
- News - Causes and Effects of Sleep Paralysis - 1700561382Document36 pagesNews - Causes and Effects of Sleep Paralysis - 1700561382Counsel IndiaNo ratings yet
- Engels Ted Talk FileDocument9 pagesEngels Ted Talk FilePssst PssstNo ratings yet
- Gail Williams 2004Document4 pagesGail Williams 2004Messias FilhoNo ratings yet
- Sleep and Learning 3 1Document3 pagesSleep and Learning 3 1haoran2219No ratings yet
- FAQ Sleep LearningDocument33 pagesFAQ Sleep Learningmy_Scribd_pseudoNo ratings yet
- Common Sleep Problems in Children - Pediatrics in Review - 2011Document11 pagesCommon Sleep Problems in Children - Pediatrics in Review - 2011JanelleNo ratings yet
- Lecture 10Document73 pagesLecture 10Madeha AshrafNo ratings yet
- DreamsfinDocument7 pagesDreamsfinMohammed KashifNo ratings yet
- Learn To Lucid DreamDocument87 pagesLearn To Lucid Dreamseth-mars100% (3)
- Consciousness: Claudine Anderson-Atkinson, PH.DDocument69 pagesConsciousness: Claudine Anderson-Atkinson, PH.DOdaine BennettNo ratings yet
- News - Causes and Effects of Sleep Paralysis - 1700561382Document36 pagesNews - Causes and Effects of Sleep Paralysis - 1700561382Counsel IndiaNo ratings yet
- Consciousness: Darren J. Gonzales Faculty, College of Arts and SciencesDocument46 pagesConsciousness: Darren J. Gonzales Faculty, College of Arts and SciencesDarren Javier GonzalesNo ratings yet
- Healthy Sleep: Your Guide ToDocument4 pagesHealthy Sleep: Your Guide ToΓιώργος ΚαραμπέρηςNo ratings yet
- Healthy Sleep: Your Guide ToDocument4 pagesHealthy Sleep: Your Guide Toeric vbNo ratings yet
- Healthy Sleep: Your Guide ToDocument4 pagesHealthy Sleep: Your Guide Toeric vbNo ratings yet
- Research EssayDocument5 pagesResearch Essayapi-583003788No ratings yet
- Nightmares: Important Things To Know About NightmaresDocument2 pagesNightmares: Important Things To Know About NightmaresGermán Ramírez HuertaNo ratings yet
- Managing Insomnia Lesson 1Document22 pagesManaging Insomnia Lesson 1taurus_europe100% (3)
- The Lull-A-Baby Sleep Guide 2: An Essential Guide To Improving a Child's Sleep Quality For Better Growth and DevelopmentFrom EverandThe Lull-A-Baby Sleep Guide 2: An Essential Guide To Improving a Child's Sleep Quality For Better Growth and DevelopmentNo ratings yet
- Managing Your SleepDocument15 pagesManaging Your Sleepmblewis91No ratings yet
- 10 Interesting Facts About Lucid Dreaming That Will Open Your MindDocument7 pages10 Interesting Facts About Lucid Dreaming That Will Open Your MindÁkos VágvölgyiNo ratings yet
- CHP 3 Writing AssignmentDocument2 pagesCHP 3 Writing AssignmentChrizellena AbenalesNo ratings yet
- Program Articles s9k6qr9PGaWgAmFCURMV 426-Night WakingDocument21 pagesProgram Articles s9k6qr9PGaWgAmFCURMV 426-Night WakingAlessandra Sayuri Almeida SilvaNo ratings yet
- Research EssayDocument14 pagesResearch Essayapi-581928438No ratings yet
- Sleep & DreamingDocument26 pagesSleep & DreamingAkosua100% (2)
- Speech: SleepwalkingDocument2 pagesSpeech: SleepwalkingEryna0% (1)
- Sleeping Beauty - Pages 3 and 4Document2 pagesSleeping Beauty - Pages 3 and 4Marianna RochaNo ratings yet
- Enhance Your Dream Life 1.1Document54 pagesEnhance Your Dream Life 1.1Stephanie BradleyNo ratings yet
- Secrets to Falling Asleep - Get Better Sleep to Improve Health and Reduce StressFrom EverandSecrets to Falling Asleep - Get Better Sleep to Improve Health and Reduce StressNo ratings yet
- Misty Williams How Are You Wired To Sleep UpdatedDocument21 pagesMisty Williams How Are You Wired To Sleep UpdatedCarolyn McClendonNo ratings yet
- Sleep Is ScientificDocument42 pagesSleep Is ScientificGlucose DRglucoseNo ratings yet
- Consciousness PsychologyDocument32 pagesConsciousness PsychologyDeea Addine As-SoubNo ratings yet
- UoN STUDENTS SUCCESSFULLY PLACED IN INDUSTRYDocument2 pagesUoN STUDENTS SUCCESSFULLY PLACED IN INDUSTRYMoreen WachukaNo ratings yet
- RFQ For The Procurement of Ipad Cover ..Document12 pagesRFQ For The Procurement of Ipad Cover ..Moreen WachukaNo ratings yet
- Marketing Hacks For All Businesses - LinkedInDocument10 pagesMarketing Hacks For All Businesses - LinkedInMoreen WachukaNo ratings yet
- RFQ-001-2023 Supply of ICT Equipment - PDF - EA Data HandlersDocument1 pageRFQ-001-2023 Supply of ICT Equipment - PDF - EA Data HandlersMoreen WachukaNo ratings yet
- RFQ-001-2023 Supply of ICT Equipment - PDF - EA Data HandlersDocument1 pageRFQ-001-2023 Supply of ICT Equipment - PDF - EA Data HandlersMoreen WachukaNo ratings yet
- Gerard - 07000212 - PHD - RedactedDocument312 pagesGerard - 07000212 - PHD - RedactedMoreen WachukaNo ratings yet
- Table of ContentsDocument1 pageTable of ContentsMoreen WachukaNo ratings yet
- Government Spokesman AdvertDocument3 pagesGovernment Spokesman AdvertMoreen WachukaNo ratings yet
- SafariDocument11 pagesSafariMoreen WachukaNo ratings yet
- Hisense 43A4G 43 Inches Full HD Smart TV - Hisense KenyaDocument2 pagesHisense 43A4G 43 Inches Full HD Smart TV - Hisense KenyaMoreen WachukaNo ratings yet
- 1copy of Openning ResultsDocument1 page1copy of Openning ResultsMoreen WachukaNo ratings yet
- HSM200 FeedbackDocument37 pagesHSM200 FeedbackMoreen WachukaNo ratings yet
- HSM200 Marking Grid Version 3. Final 22.05.2022Document3 pagesHSM200 Marking Grid Version 3. Final 22.05.2022Moreen WachukaNo ratings yet
- HSM200 Assessment Guide Draft Version 6 Final 21.05.22Document7 pagesHSM200 Assessment Guide Draft Version 6 Final 21.05.22Moreen WachukaNo ratings yet
- GENERALISATIONDocument17 pagesGENERALISATIONgreyproperties88No ratings yet
- Wiw3362 W 503 PDFDocument1 pageWiw3362 W 503 PDFabathunNo ratings yet
- LAS in ENGLISH 10 QUARTER 3 WEEK 4 TRENTO NHSDocument23 pagesLAS in ENGLISH 10 QUARTER 3 WEEK 4 TRENTO NHSCherry Mae B. Corria100% (1)
- Ielts Reading Exercise TypesDocument44 pagesIelts Reading Exercise TypesTú VõNo ratings yet
- Week 1 - Assessment #1Document2 pagesWeek 1 - Assessment #1elaineNo ratings yet
- ATR100 Owners Manual PDFDocument20 pagesATR100 Owners Manual PDFHernan Alberto Orozco CastañoNo ratings yet
- Philos and Philos Long: Surgical TechniqueDocument38 pagesPhilos and Philos Long: Surgical TechniqueSamuel HarnaenNo ratings yet
- Needles Found Inside A StrawbeeryDocument2 pagesNeedles Found Inside A StrawbeeryThiz Izz PangiranNo ratings yet
- Balustrade Design Guide For EducationDocument1 pageBalustrade Design Guide For EducationRey Eduard Q. UmelNo ratings yet
- Tenses-Grammar ExercisesDocument3 pagesTenses-Grammar ExercisesUla MisiekNo ratings yet
- Set TheoryDocument3 pagesSet TheoryMaria IvanovaNo ratings yet
- Finallist 2012Document147 pagesFinallist 2012tracker1234No ratings yet
- Will and Going To WSDocument3 pagesWill and Going To WSKatia Belen CARDENAS ROJASNo ratings yet
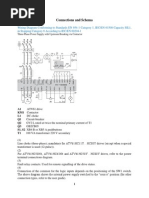
- Connections and SchemaDocument7 pagesConnections and SchemaKukuh WidodoNo ratings yet
- 20181PIR7Document13 pages20181PIR7farahnuratiqah.mohdradziNo ratings yet
- Cronologia - Marvel ComicsDocument9 pagesCronologia - Marvel ComicsrafaelasevedosNo ratings yet
- LTQ Orbitrap Discovery HardwareDocument118 pagesLTQ Orbitrap Discovery Hardwarepribadi socojatiNo ratings yet
- Technical Issues Related To New Transmission Lines in Denmark PDFDocument132 pagesTechnical Issues Related To New Transmission Lines in Denmark PDFAndré Luiz0% (1)
- Crane HI-4EDocument8 pagesCrane HI-4EseowshengNo ratings yet
- Operation Manual: Read Before Flying!Document24 pagesOperation Manual: Read Before Flying!ruup2010 AlexNo ratings yet
- Balancing Chemical Equations HTML Guide - enDocument2 pagesBalancing Chemical Equations HTML Guide - enMiguel ApazaNo ratings yet
- SchizophaniaDocument52 pagesSchizophaniaRujuta BaramateNo ratings yet
- Tugas Makalah Mata Kuliah Steril Mencari Formula Sediaan Salep Mata Dan SuspensiDocument8 pagesTugas Makalah Mata Kuliah Steril Mencari Formula Sediaan Salep Mata Dan SuspensiAfriady Nuur MuhammadNo ratings yet
- Thermal Comfort of BuildingsDocument12 pagesThermal Comfort of BuildingsNavya BhardwajNo ratings yet
- RRN3901 Spare Parts CatalogDocument11 pagesRRN3901 Spare Parts CatalogleonardomarinNo ratings yet
- Reading Comprehension Tests - 83653Document2 pagesReading Comprehension Tests - 83653Henry Rojas VasquezNo ratings yet
- Problemario 2Document2 pagesProblemario 2Frank Hurtado0% (1)
- Walking With God in The DesertDocument24 pagesWalking With God in The DesertF. Remy Diederich100% (2)
- Moeller df51 Manual PDFDocument241 pagesMoeller df51 Manual PDFpraetorianbl0% (2)